
Abstract
A 21-year-old Dutch crossbred mare was presented with a 1-month history of weight loss and weakness. Clinical evaluation revealed severe anemia and thrombocytopenia with evidence of hepatic disease and muscular damage. Necropsy findings included diaphragmatic rupture with an extensive retroperitoneal hematoma and severe hepatosplenomegaly. Microscopic findings were characterized by hepatic sinusoidal and splenic red pulp infiltration by atypical CD3-positive lymphocytes. No other nodal or extranodal sites were affected. Hepatosplenic lymphoma with a probable T-cell origin was diagnosed based on gross and histologic findings.
Lymphoma is considered the most frequent neoplasm of the equine hematopoietic system, with an incidence of 0.7–3.2/100,000 horses.16,17 Equine lymphomas are currently grouped into four clinical–pathologic presentations involving primarily either lymph nodes (multicentric form) or extranodal sites such as alimentary canal, skin, or thymus.18,23 The concurrent involvement of hepatic and splenic parenchyma is commonly reported as the result of the staging procedure of multicentric lymphomas in humans4 and horses.1,2,13,15,23 Although the concurrent and restricted involvement of liver and spleen in lymphoma is rare, primary hepatosplenic lymphoma (HSPL) has been described as a distinct disease in humans since 19908 and is well documented.24 HSPL is an extranodal lymphoma characterized by infiltration of hepatic sinusoids and splenic red pulp sinuses predominantly by TCRγδ, CD8-positive T cells.24 Recently, several cases of HSPL expressing TCRαβ have been described.14 In humans, the disease has an aggressive clinical course with unsatisfactory response to chemotherapy.24 In this report, we describe clinical presentation and macroscopic, microscopic, and phenotypic findings of a T-cell HSPL in a mare.
A 21-year-old Dutch crossbred mare developed progressive weight loss and weakness. Three weeks after the initial signs, the horse was referred to the Padova Veterinary Teaching Hospital. The initial physical examination revealed moderate depression, marked subcutaneous edema of the abdominal wall extending to the hind limbs, pale mucous membranes and petechiae in oral and vaginal mucosae. The hemogram revealed a normochromic normocytic anemia (erythrocytes = 4 × 106 cells/µl, hematocrit = 22.9%, hemoglobin = 8.1 g/dl, mean corpuscular volume = 55.1 fl, mean corpuscular hemoglobin = 19 pg, mean corpuscular hemoglobin concentration = 35.1%) and severe thrombocytopenia (103 cells/µl) with prolonged bleeding time after venipuncture and local hematoma formation. The leukogram was characterized by mild leukopenia (4.4 × 103 cells/µl) with a differential of 3,300 neutrophils, 836 lymphocytes, 220 monocytes, and 44 eosinophils. Clinical chemistry data included elevated urea (121 mg/dl) and blood urea nitrogen (56.5 mg/dl) with normal creatinine (1.38 mg/dl) associated with a mild increase of creatine kinase (>1,500 IU/liter) indicative of muscle leakage. Increased bilirubin values (total = 4.96 mg/dl, conjugated/direct = 0.7 mg/dl, indirect/unconjugated = 4.26 mg/dl) and gamma glutamyltranspeptidase (644 IU/liter) suggested cholestasis. Coggins test for equine infectious anemia was negative. Three days after admission, the mare fell suddenly. Despite rehydration and antibiotic and steroid therapy, the horse developed severe weakness, generalized tremors with a pulse of 78 beats/minute, difficult breathing, and a rectal temperature of 38.7 C. Mucous membranes were icteric and pale at this time. Percussion, rectal palpation, and ultrasound revealed a large mass that extended to the anterior abdomen and had a solid to fluid echogenic appearance. The horse's condition deteriorated rapidly, and she was found dead the next morning.
For histologic evaluation, tissue samples were fixed in 10% buffered formalin, routinely processed, and stained. Tumor cell characterization was based on the evaluation of tissue distribution, cell morphology, and immunophenotype. The revised European–American classification of lymphoid (REAL) neoplasms was used for classification.9 Immunohistochemistry of hepatic and splenic sections was performed with an avidin–biotin–peroxidase kit according to the manufacturer's instructions (Vector Laboratories, Burlingame, CA). Sections were incubated with monoclonal anti-human CD79-α antibody (DAKO, Glostrup, Germany) diluted 1:50 and with polyclonal anti-human CD3 antibody (DAKO) diluted 1:900. Antigen retrieval was performed as previously reported.3,13 These two antibodies recognize epitopes conserved in many species, including horses, and have been utilized to characterize equine lymphoid tissues and lymphomas.3,13 Polyclonal anti-equine IgM diluted 1:15,000 (Bethyl Co., Montgomery, TX), anti-equine IgG diluted 1:25, 000 (Bethyl Co.), and anti-human factor VIII diluted 1:500 (DAKO) were also applied. Enzymatic digestion with 1% trypsin at 37 C for 30 minutes was performed prior to incubation with the polyclonal antibodies. Sections of formalin-fixed, paraffin-embedded normal equine popliteal lymph node were used to check CD3, CD79-α, and immunoglobulin antigen distribution and served as positive controls. Negative controls were generated by replacing the primary antibody with nonimmune rabbit serum or a monoclonal anti-human CD8 antibody. Bone marrow (BM) smears were obtained from femoral BM and were stained with May–Gränwald–Giemsa stain.
The necropsy revealed pale mucous membranes with petechiae in oral, rectal, and vaginal mucosae. Diffuse, severe subcutaneous edema extended from the abdominal wall to the hind limbs. Muscular layers of the abdominal wall were dissected by a large amount of poorly coagulated blood that originated from a large mass approximately 100 × 150 cm (large intradiaphragmatic hematoma). The hematoma dissected the pars muscularis of the diaphragm and extended to the umbilical region. The abdominal cavity contained approximately 10 liters of serohemorrhagic fluid. Severe, diffuse splenomegaly and hepatomegaly were present. The spleen and liver had a homogeneous surface and were devoid of nodular lesions. The cut surface of the liver was characterized by vascular and sinusoidal dilation. The ileum and the large intestine were severely thickened, and the cut surface of the intestinal wall was distended by transmural edema. Lungs were bilaterally and diffusely hyperemic, with areas of atelectasis. Peripheral and internal lymph nodes were grossly normal. No mediastinal, abdominal, or cutaneous masses were observed. Histologic sections of the diaphragm contained elevated numbers of erythrocytes embedded in a loose fibrin meshwork. Multifocally, interstitial areas of hemorrhage and fibroplasia dissected the diaphragmatic fibers. Sarcolemmal rupture and hyaline and granular myocyte degeneration were common findings. Interstitial erythrophagocytosis and hemosiderin-laden macrophages were most commonly present between myocytes in areas adjacent to the hemorrhages. Multifocally, diaphragmatic veins contained fibrinocellular thrombi. Hepatic sinusoids and centrolobular and occasionally portal veins were severely dilated and contained increased numbers of erythrocytes and atypical round cells (Fig. 1). Occasionally, random transsinusoidal invasion of the hepatic parenchyma by the neoplastic cells was observed. The neoplastic round cells were medium to large (25–35 μm in diameter) with a small to moderate amount of nongranulated clear cytoplasm. Nuclei were round to oval, often indented, and more frequently variably folded to cerebriform. Chromatin was dispersed to finely granular and often marginated. Nucleoli were mostly inconspicuous, but an occasional prominent, large, irregular central nucleolus or multiple (two to seven) nucleoli were seen. In the spleen, elevated numbers of erythrocytes and atypical round cells infiltrated cords and sinuses of the red pulp, with complete atrophy of the white pulp. BM was normocellular, and myeloid and erythroid series were complete with regular maturation (myeloid:erythroid ratio = 0.8:1). No significant microscopic changes were present in all other organs examined including lymph nodes and mediastinal tissues. Neoplastic cells expressed the CD3-∊ chain (Fig. 2) and were negative for factor VIII, CD79-α, IgG, IgM, and IgA. These results were consistent with a T-cell phenotype. A diagnosis of a large T-cell hepatosplenic lymphoma was made based on clinical, gross, and microscopic findings.
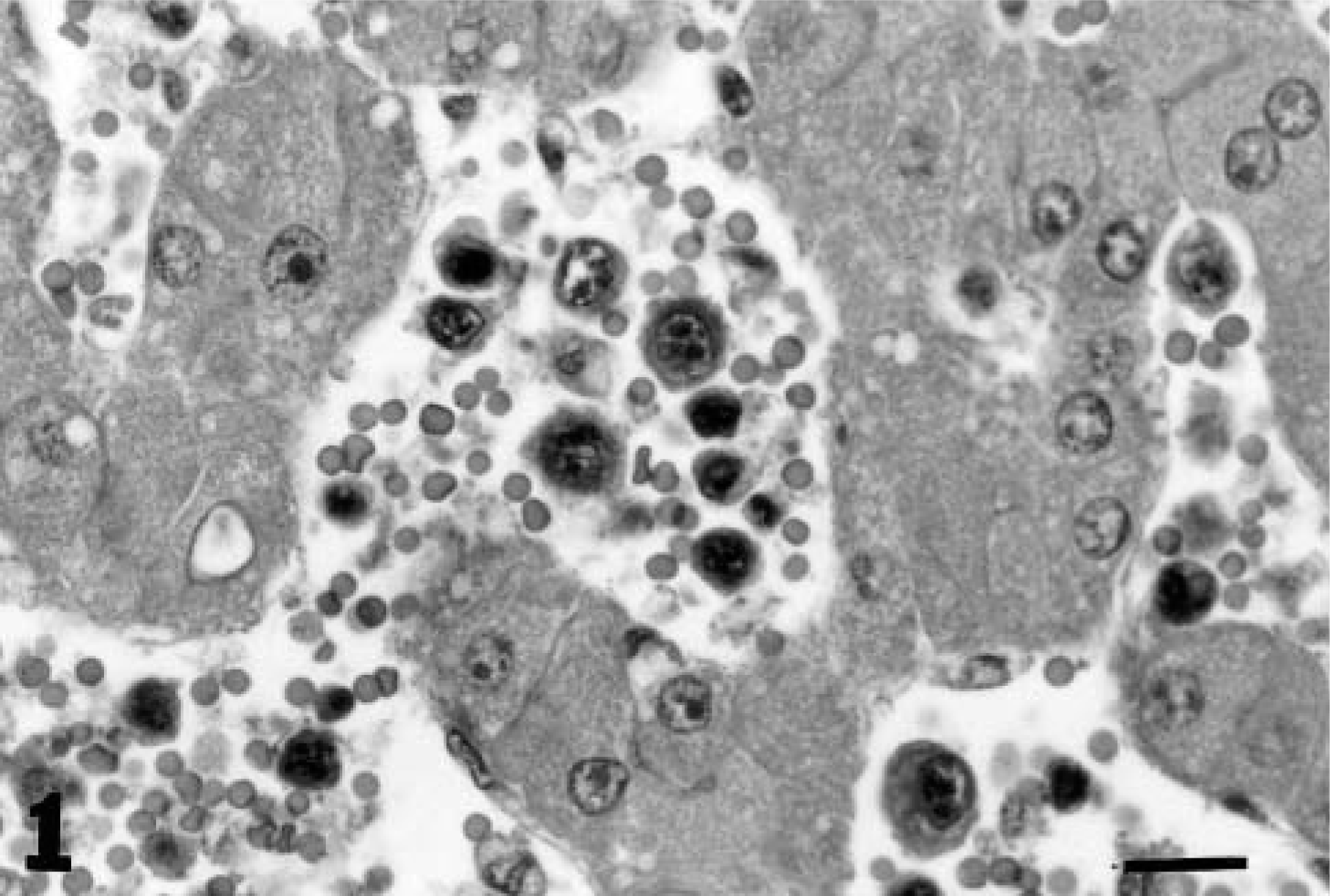
Liver; horse. The hepatic sinusoids contain medium to large atypical round cells with homogeneous cytoplasm and irregular nuclei. HE. Bar = 30 μm.
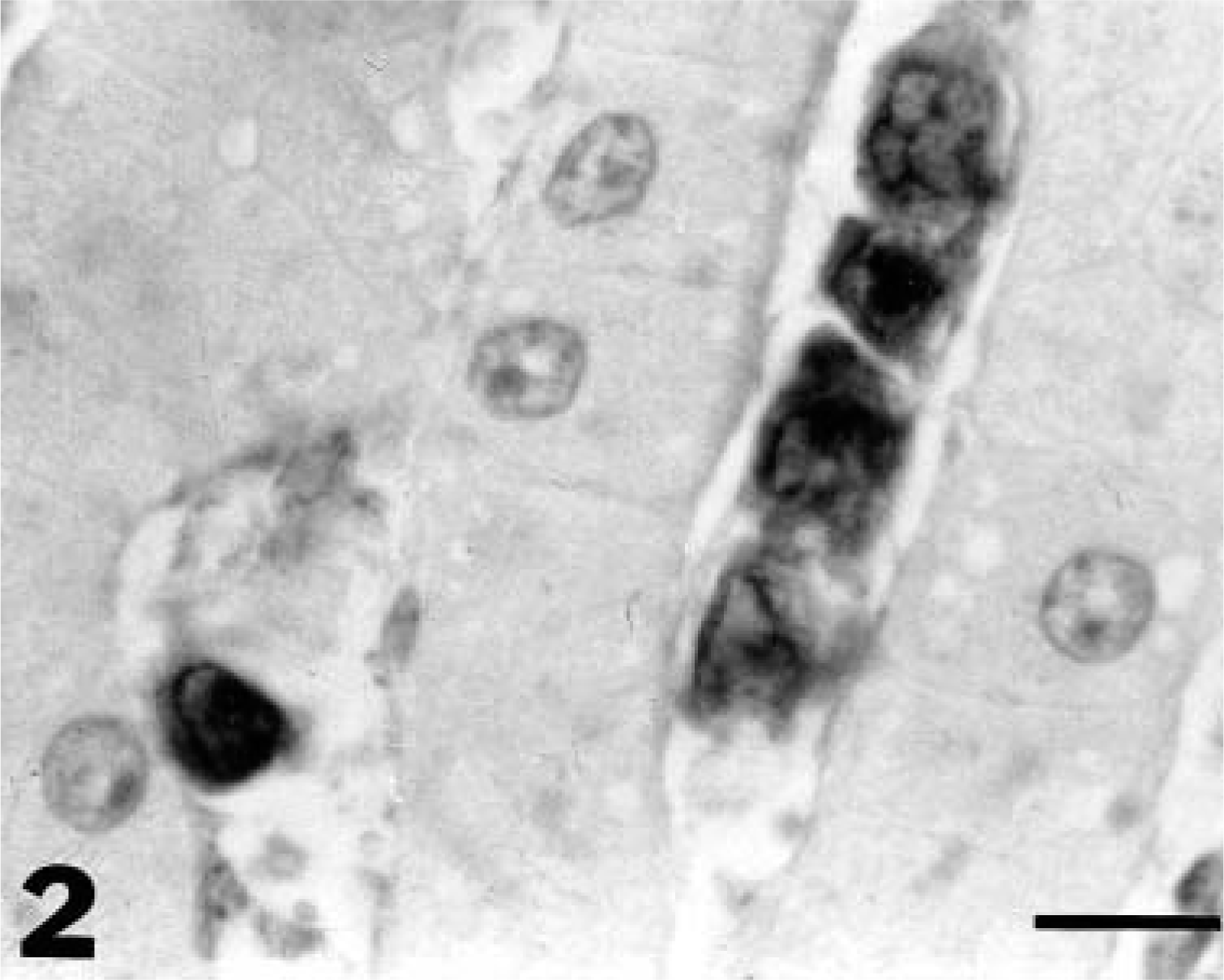
Liver; horse. CD3-positive atypical lymphoid cells in the hepatic sinusoids. Polyclonal anti-CD3-∊, avidin–biotin–peroxidase complex method, AEC chromogen, hematoxylin counterstain. Bar = 33 μm.
In this mare, pathologic findings differed from those in cases of extranodal lymphoma previously reported. The most significant differences were the finding of a diffuse hepatosplenomegaly even though BM peripheral blood, lymph nodes, and other extranodal sites were free of disease. Within the clinical spectrum of equine lymphomas, concurrent hepatosplenic involvement has been identified during the staging procedure of multicentric lymphomas.1,2,13,15,23 In equine multicentric lymphoma, liver and spleen commonly exhibit multiple raised, nodular lesions in contrast with the gross appearance of both organs in the present case.1–3,13,18–20 Diffuse hepatosplenomegaly has been reported in association with lymph node3 and renal13 involvement in two horses. Additionally, the distinctive infiltration of hepatic sinusoids and splenic red pulp in the horse in the present study differs from findings in equine lymphomas and lymphoid leukemias previously described, where expansion of hepatic portal tracts and splenic white pulp by neoplastic cells is the predominant finding.3,15,21 The pathologic presentation in this mare closely resembled that in human HSPL. HSPL is a peripheral lymphoma described as a distinct disease entity in humans in 19908 and has been included in the REAL classification for human lymphomas since 1994.9 The diagnosis of HSPL is based on the clinicopathologic finding of concurrent hepatic and splenic involvement, with occasional invasion of bone marrow sinuses.14 24 Patients with HSPL usually present with fatigue and jaundice associated with hepatosplenomegaly. In humans with HSPL, peripheral cytopenias with a concurrent normocellular bone marrow are the characteristic hematological findings.24 All these clinical features and, notably, a severe thrombocytopenia associated with a normal BM were observed in this mare. Thrombocytopenia is usually the most striking hematologic abnormality reported in nearly all human cases of HSPL.24 Patients with HPSL do not have anti-platelet antibodies, and thrombocytopenia was initially ascribed to hypersplenism. However, in most patients with HPSL, platelets do not return to normal after splenectomy.5 This unusual behavior has prompted researchers to formulate the hypothesis that cytokines, such as γ-interferon produced by malignant T cells, may be involved in selective BM suppression.7,23 However, the correlation between normal BM and peripheral thrombocytopenia has not been fully elucidated. In this horse, the cytology and histology of the BM were normal, and the thrombocytopenia was reported prior to the acute trauma. Thus, the clinicopathologic findings were similar to those associated with HSPL in humans. The diaphragm is the most frequently ruptured muscle in domestic animals, tears developing usually as a consequence of increased abdominal pressure.10 In this horse, the presence of the severe hepatic and splenic enlargement associated with the trauma could explain the rupture of the diaphragm and the spontaneous death. Evidence of splenic red pulp and hepatic sinusoid invasion by neoplastic lymphoid cells closely resembled the microscopic findings associated with human HPSL.8,24 HPSL is considered the prototype of human CD3+ CD8− to weak γδ T cell diseases, although cases expressing TCRαβ with comparable clinicopathologic findings have been recently reported. In this mare, cells had a lymphoid morphology, were negative for all B-cell markers, but expressed the CD3-∊ chain. Expression of surface CD3 is considered specific for T-cell origin. However, the polyclonal antibody utilized in this study identifies the intracytoplasmic ∊ chain of the CD3 antigen. Cytoplasmic CD3-∊ positivity is common to T cells and subpopulations of natural killer (NK) cells.22 Thus, an NK origin cannot be completely ruled out. Although a hepatosplenic presentation has been rarely observed in human NK tumors, it remains the major phenotypic differential diagnosis in humans. Despite widespread involvement of the spleen, the microscopic findings could not clearly elucidate the primary origin of the tumor in this horse. In humans, the origin of HSPL seems to vary depending on the pathologic process. Most cases of γ/δ T-cell HSPL seem to have a splenic derivation, which can be explained by the fact that γ/δ lymphocytes home preferentially to the splenic red pulp.6,11 However, hepatitis C virus infection has been associated with a primary hepatic origin for some cases of HSPL in humans.12 Thus, the primary origin of the tumor in this horse remains uncertain. Collection of fresh material will be fundamental to confirm a T-cell origin of neoplastic cells and to verify the TCR αβ or γδ usage by neoplastic cells in cases of equine HSPL. This is the first documented case of HSPL in the horse, and HSPL should be incorporated into the classification of equine lymphomas.