
Abstract
We describe a case of a dog with hepatosplenic lymphoma, a disease characterized by infiltration of the liver, spleen, and bone marrow with γδ T cells, absence of peripheral lymphadenopathy, and an aggressive clinical course. Physical examination findings, hematologic and biochemical abnormalities, and clinical course of the disease in this patient were similar to those in humans. Immunophenotyping of liver and spleen aspirates supported an antemortem diagnosis of T-cell lymphoma consistent with hepatosplenic lymphoma. The diagnosis was confirmed postmortem by a combination of routine histopathology, showing a consistent pattern of organ involvement, and immunohistochemistry showing the infiltrating neoplastic lymphocytes to be T cells expressing the γδ T-cell receptor. To our knowledge, this is the first reported case of hepatosplenic lymphoma in a dog.
Hepatosplenic T-cell lymphoma (HSTL) was first described as a clinical entity in humans in 1990, and over 40 cases have been reported since then. 4,8,10,17 Humans with HSTL usually present with systemic signs, anemia, and thrombocytopenia. The disease is characterized by infiltration of the liver, spleen, and bone marrow with neoplastic lymphocytes expressing the γδ T-cell receptor (TCR), absence of peripheral lymphadenopathy, and an aggressive clinical course. To our knowledge, there has been no previous report of HSTL in dogs.
Case History and Results
A 5-year-old spayed female Siberian Husky mixed breed dog weighing 24 kg presented to the Veterinary Medical Teaching Hospital (VMTH) for lethargy, anorexia, and weight loss of 2 weeks duration. Evaluation by the referring veterinarian 3 days before presentation found pancytopenia, increased liver enzymes and total bilirubin, and decreased albumin. Antibiotic therapy (tetracycline, 500 mg BID, PO) was started at that time. Abnormalities noted on initial physical examination at the VMTH included lethargy, pyrexia, generalized muscle atrophy, and splenomegaly. A complete blood count (CBC) found a mild, moderately regenerative anemia with slight spherocytosis, moderate thrombocytopenia, and low numbers of slightly toxic band neutrophils (Table 1). Serum biochemical abnormalities were consistent with hepatic insufficiency (Table 2). Direct Coombs' and direct slide agglutination tests at room temperature and 4 C were negative. Partial thromboplastin time was consistently mildly prolonged (Table 2). Moderate proteinuria and bilirubinuria were noted on routine urinalysis; urine sediment contained 0–3 red blood cells (RBCs) per high-power field and rare bilirubin crystals. The urine protein-creatinine ratio was within reference limits (0.76; reference ≤1). A fecal occult blood test was positive. Aerobic and anaerobic blood cultures were negative. No lead was detected in the dog's blood. Ultrasonographic examination of the abdomen found hepatosplenomegaly, a thickened and mildly hypoechoic gallbladder wall, and a coarse echotexture of the liver, findings interpreted as most consistent with cholecystitis and suspicious for hepatitis. Thoracic radiographs were unremarkable.
Hematologic data of a dog with hepatosplenic lymphoma.
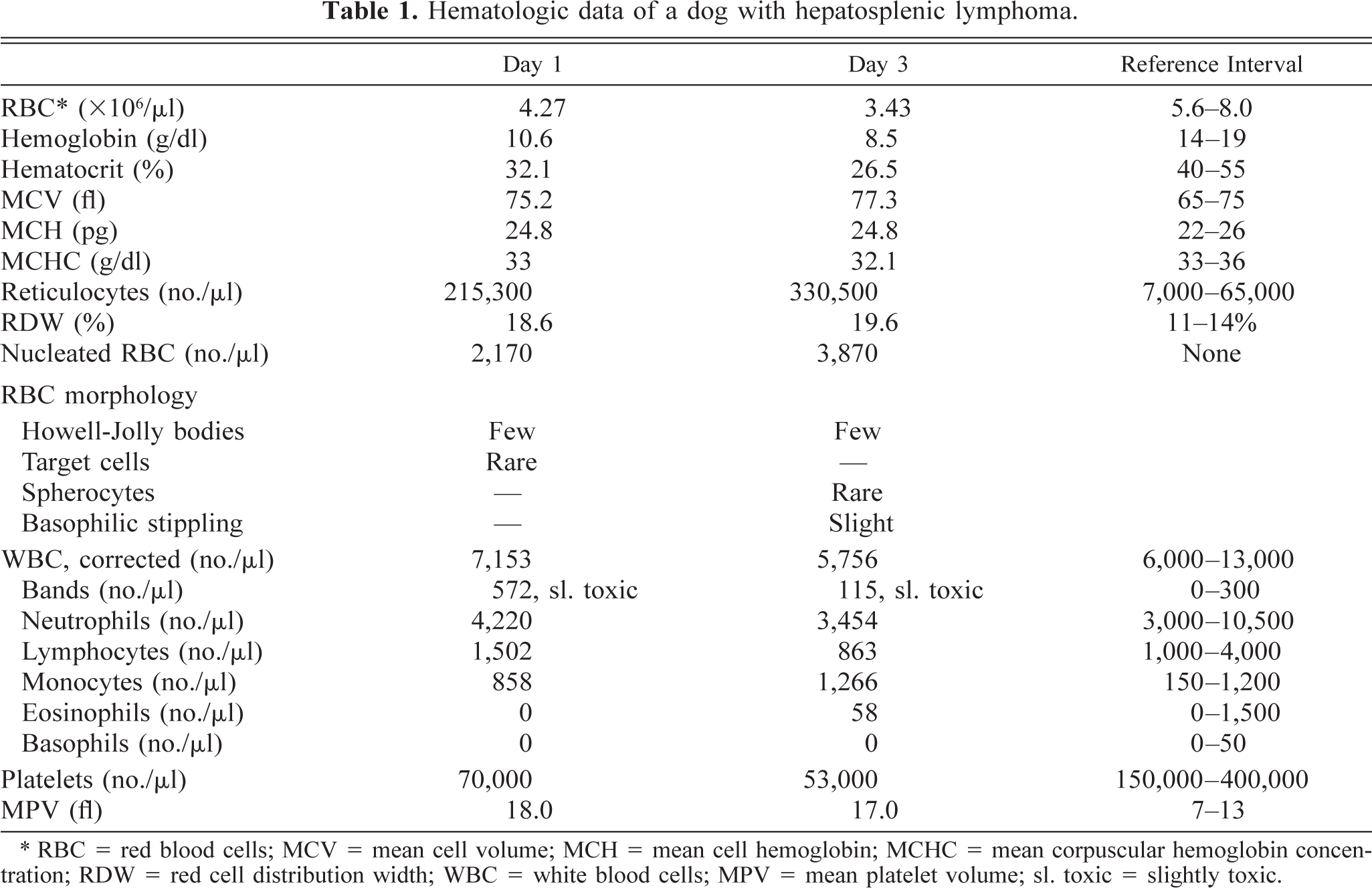
∗ RBC = red blood cells; MCV = mean cell volume; MCH = mean cell hemoglobin; MCHC = mean corpuscular hemoglobin concentration; RDW = red cell distribution width; WBC = white blood cells; MPV = mean platelet volume; sl. toxic = slightly toxic.
Serum chemistry and coagulation profile data of a dog with hepatosplenic lymphoma.
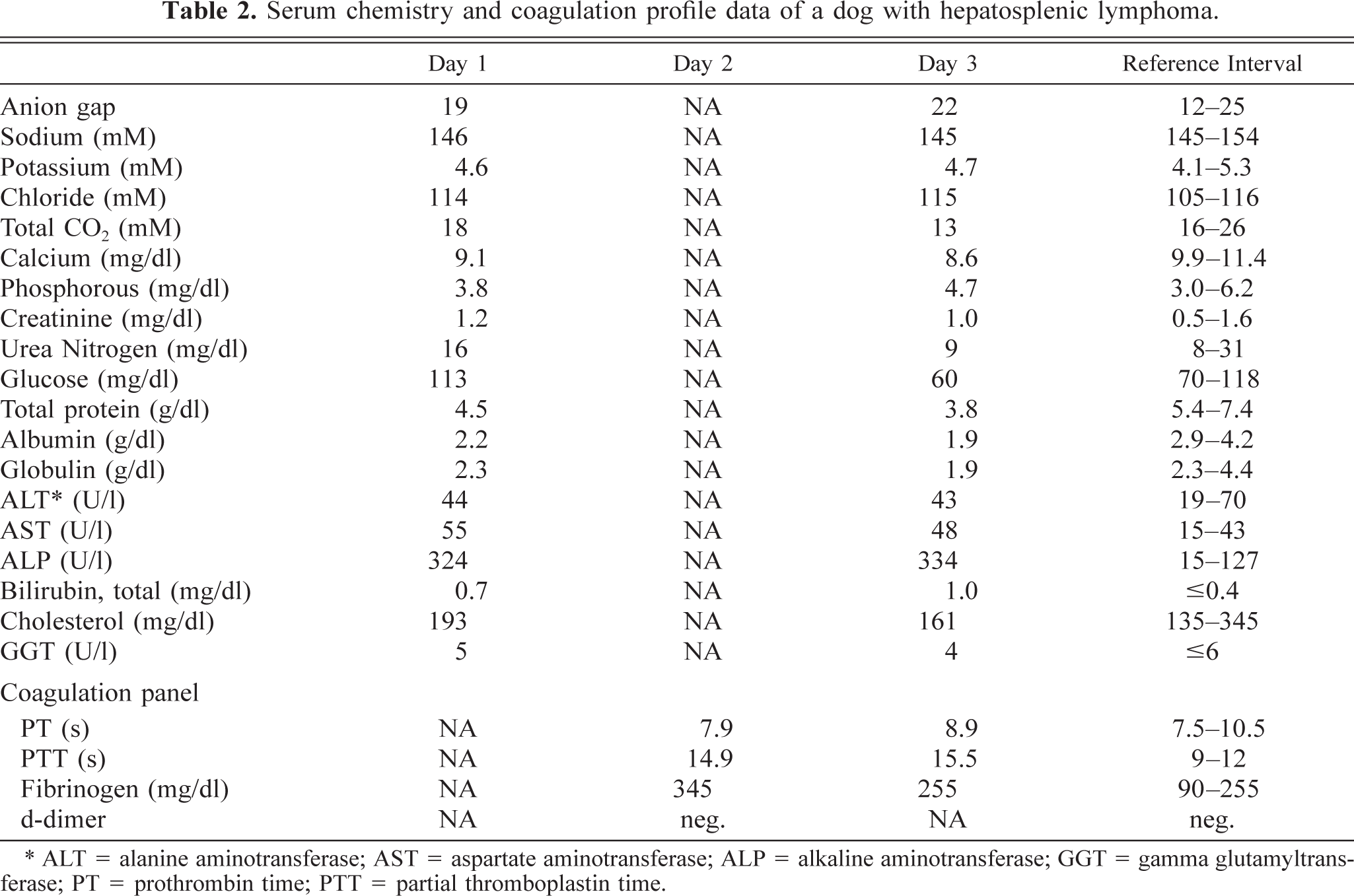
∗ ALT = alanine aminotransferase; AST = aspartate aminotransferase; ALP = alkaline aminotransferase; GGT = gamma glutamyltransferase; PT = prothrombin time; PTT = partial thromboplastin time.
Differential diagnoses on the basis of these findings included infection (cholecystitis/hepatitis), immune-mediated hemolytic anemia (IMHA), immune-mediated thrombocytopenia, and neoplasia. Gastrointestinal (GI) hemorrhage was suspected. Initial treatment included intravenous (IV) fluids (lactated Ringer's solution q.s., 20 mEq KCl, 100 ml/h), altered antibiotic therapy (750 mg ampicillin PO, TID; 136 mg enrofloxacin PO, SID), and GI protectant therapy (24 mg ranitidine IV, BID). Subsequent treatment included vitamin K1 therapy (1 mg/kg SQ, BID), and IV plasma (2 units over 4 hours) and colloids (Hetastarch, 24 ml/hour).
The dog became more lethargic and developed petechiae on the ventral abdomen by day 4. Repeat CBC, serum biochemical analysis, and coagulation panel did not reveal any major new abnormalities. Pre- and postprandial bile acids were increased (pre = 94 µM, post = 147 µM; reference ≤12 and ≤16 µM, respectively). Abdominal ultrasound was repeated and found mild ascites and a hypoechoic gallbladder wall and pancreas, interpreted as edema; other ultrasonographic findings were static. Ultrasound-guided fine-needle aspirates (FNAs) of spleen, liver, and abdominal fluid were submitted for cytologic evaluation and fluid analysis. A bone marrow aspirate was collected for cytologic evaluation and anti-megakaryocyte antibody test (AMAT).
Cytologic examination of spleen (Fig. 1) and liver FNAs found marked, predominantly erythroid, extramedullary hematopoiesis (EMH), increased numbers of macrophages that were often erythrophagic, and many large round cells with dispersed chromatin and deep blue cytoplasm, sometimes with a faint perinuclear clear zone, that often contained one or two phagocytosed RBCs. In the liver, there was also moderate to marked lipid vacuolation within hepatocytes and marked canalicular plugging indicating cholestasis. It was noted that the EMH was appropriate given the dog's anemia, the macrophage hyperplasia and erythrophagia were consistent with IMHA, and the frequently erythrophagic large round cells were probably immature histiocytes; however, as the latter cells could not be definitively identified cytologically, unstained coverslip smears were submitted for immunophenotyping. It was subsequently observed that these cells occasionally contained low numbers of fine azurophilic cytoplasmic granules, usually coalesced together in a perinuclear location, a feature more consistent with a granular lymphocytic, rather than a histiocytic, origin. Bone marrow cytologic findings included unit particles of low to moderate cellularity, with relative erythroid hyperplasia and megakaryocytic hypoplasia. In addition, many large, immature round cells with morphology similar to those in splenic and hepatic FNAs were also seen. The abdominal fluid was a hemorrhagic modified transudate, with nucleated cells that included low numbers of hematopoietic precursors and immature round cells similar to those described previously.
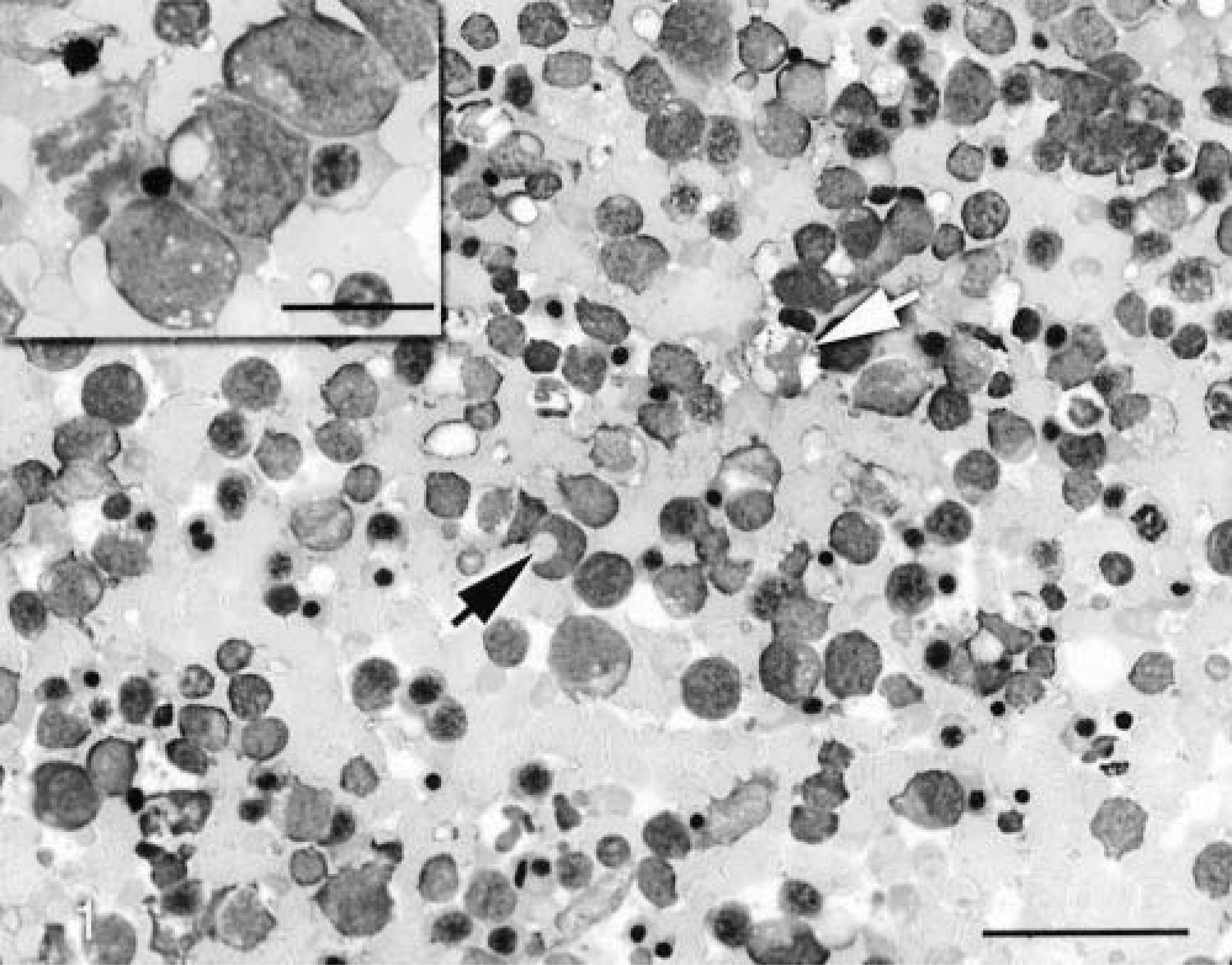
Splenic aspirate. Marked extramedullary hematopoiesis and neoplastic infiltration, with erythrophagic macrophage (white arrow) and erythrophagic neoplastic cell (black arrow). Wright-Giemsa stain. Bar = 50 µm. Inset: Higher power magnification of four of the neoplastic lymphocytes, one of which is erythrophagic and one of which is mitotic. Bar = 20 µm.
AMAT on the bone marrow aspirate was negative. Immunocytochemical staining of spleen and liver aspirates was performed on air-dried, acetone-fixed coverslip smears, using standard streptavidin–peroxidase methodology. 1 Immunostaining showed many cells positive for CD3 (CD3-12, Serotec Inc., Raleigh, NC), sometimes containing single phagocytosed RBC, corresponding in size and number with the large, immature round cells seen on routine cytologic examination. There were much lower numbers of cells staining positive for CD11b (3E10, P. F. Moore, UC-Davis), CD11c (6A1, P. F. Moore, UC-Davis), and CD1c (9H11, P. F. Moore, UC-Davis). Staining of the liver aspirate for CD79a (HM57, Dako Inc., Carpinteria, CA) was negative. These findings were interpreted as HTCL.
The dog continued to deteriorate clinically, vomiting bloody fluid and developing melena by day 5. After the owners were advised of the poor prognosis and available treatment options, which they declined, the dog was euthanatized.
Necropsy was performed. Only hepatomegaly (5.8% body weight [BW]) and splenomegaly (2.2% BW) were detected grossly. However, histologic examination of multiple tissues showed that neoplastic lymphocytes infiltrated most organs examined. Neoplastic cells were variably round to large and bizarre with distinct cell borders and scant to moderate amounts of eosinophilic cytoplasm. Approximately 5% of the neoplastic cells contained an erythrocyte or a presumed fragment of an erythrocyte. There was marked anisokaryosis, with nuclei varying from round and hyperchromatic to oblong or folded, with lightly basophilic and coarsely clumped chromatin. There were occasional binucleate cells, and one to four mitotic figures per high-power field were noted.
Within most tissues, the distribution of neoplastic cells generally reflected a vascular tropism. Neoplastic cells were present in sinusoids throughout the liver, and distinct aggregates were present in portal tracts, where they surrounded vessels and bile ducts (Fig. 2). Neoplastic cells usually surrounded central veins and were present in large numbers in associated lymphatics. The spleen was heavily infiltrated (Fig. 3), and sheets of cells obliterated normal architecture; in less markedly affected areas, neoplastic cells were limited to the red pulp and sinusoids, sparing the white pulp. In the kidney, large numbers of cells accumulated around glomeruli, within the cortical interstitium, and surrounded vessels within the corticomedullary junction. In the lung, alveolar septae were diffusely and markedly cellular (Fig. 4). Neoplastic cells were also found in segmental regions of the submucosa throughout the GI tract, within the bone marrow and tonsils, and in multiple mesenteric lymph nodes. Bone marrow involvement varied from diffuse heavy infiltration in some areas to focal, sinusoidal involvement in less affected areas. In affected mesenteric lymph nodes, there was heavy medullary sinus and cord and paracortical infiltration with relative sparing of the outer cortex. No neoplastic cells were detected in sections of thyroid, adrenals, or stomach. Immunohistochemistry on formalin-fixed (liver, spleen, lung, kidney) and frozen (liver, spleen, lymph node) tissue using methods previously described 1 showed the neoplastic cells expressed CD3 (CD3-12, Serotec Inc. Raleigh, NC), γδ TCR (8H1, P. F. Moore, UC-Davis), CD11d (8H2, P. F. Moore, UC-Davis), CD8α (JD3, P. F. Moore, UC-Davis), CD18 (4E9, P. F. Moore, UC-Davis), CD45 (10C12, P. F. Moore, UC-Davis), and CD45ra (1D3, P. F. Moore, UC-Davis). They did not express CD79a (HM57, Dako Inc., Carpinteria, CA), αβTcR (8G7, P. F. Moore, UC-Davis), CD8β (4G2, P. F. Moore, UC-Davis), or CD11b (3E10, P. F. Moore, UC-Davis). These findings were interpreted as γδ T-cell lymphoma.
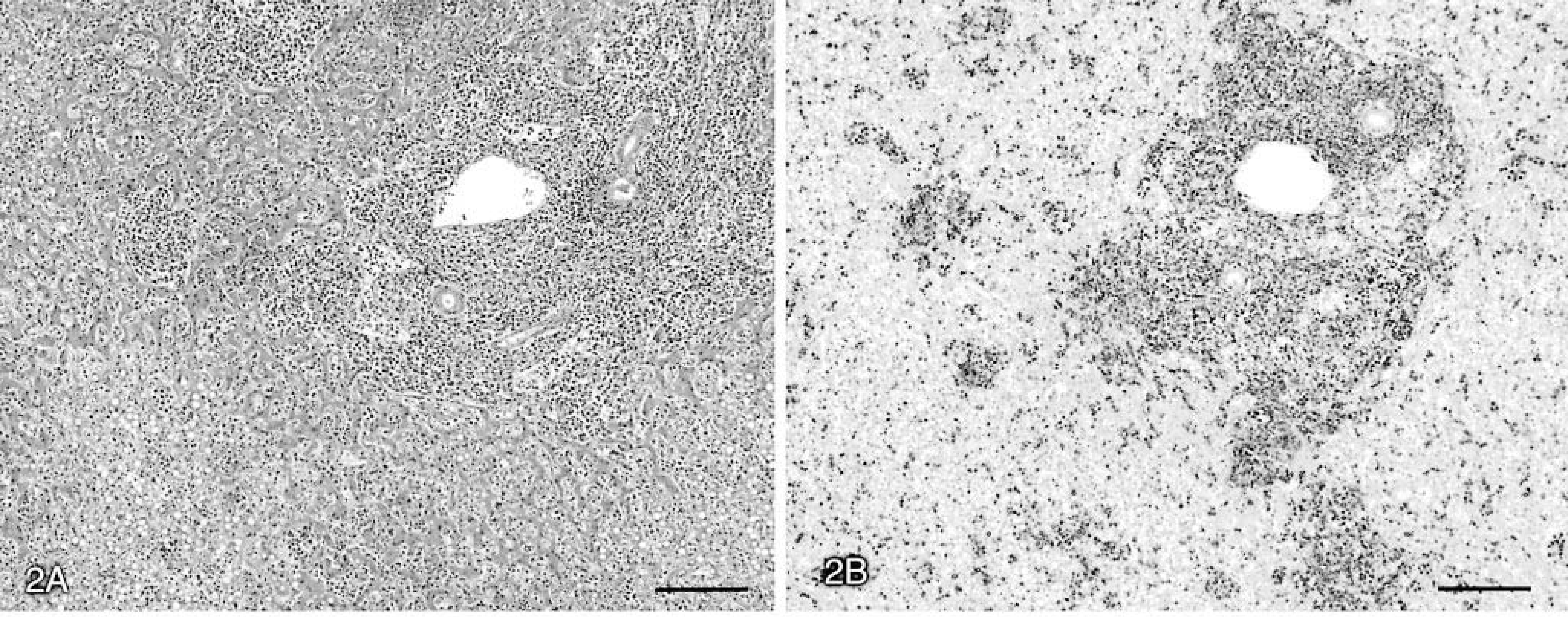
Liver. Marked diffuse sinusoidal infiltration by CD3+ neoplastic cells, with coalescence in periportal areas.
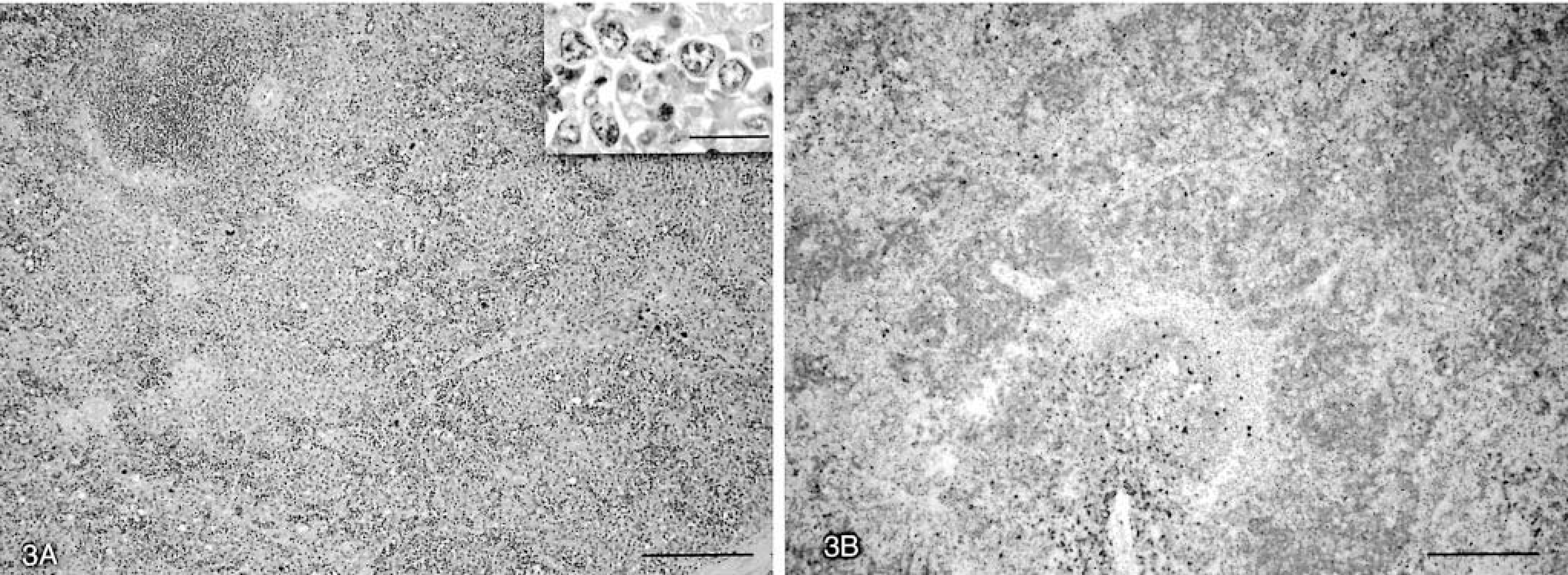
Spleen. CD3+ neoplastic cells are concentrated in areas of red pulp, with relative sparing of the white pulp (upper left, Fig. 3A and lower middle, Fig. 3B).
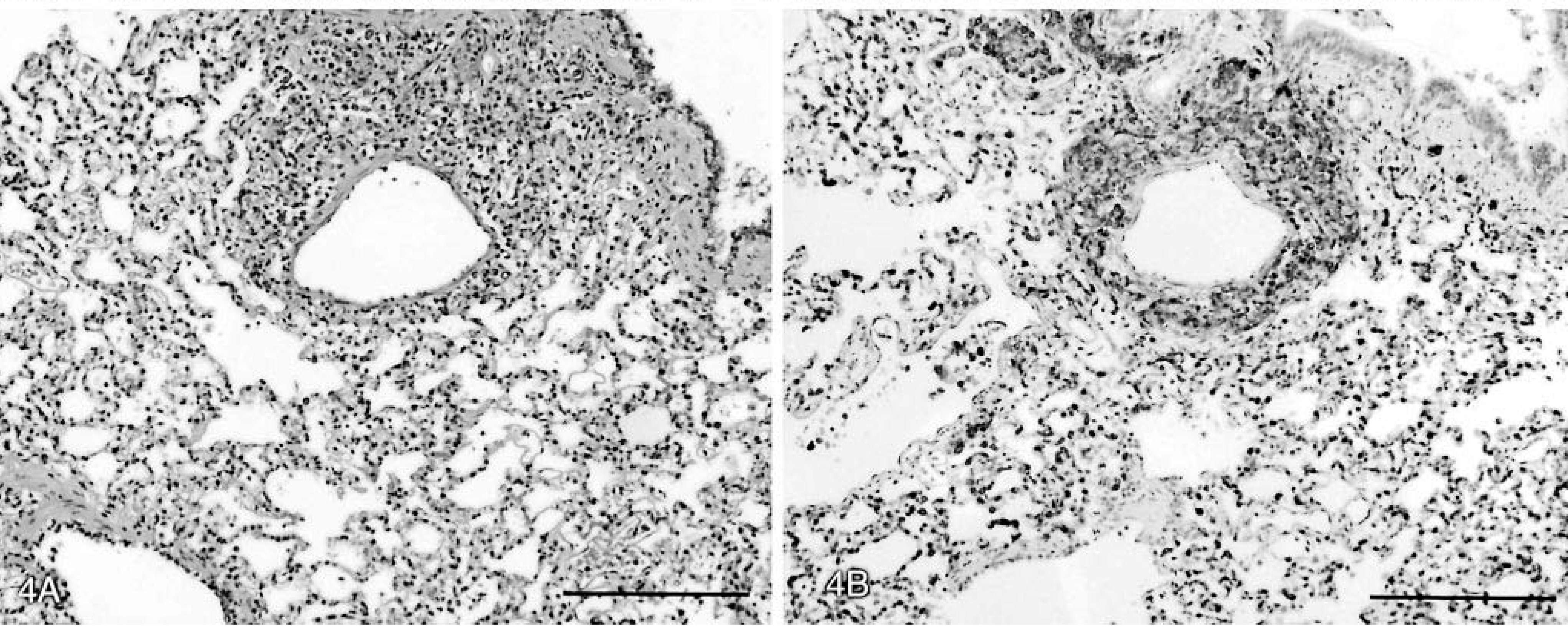
Lung. Marked infiltration of alveolar septae with CD3+ neoplastic cells, with perivascular coalescence.
Discussion
Differential diagnoses for a dog presenting with hepatosplenic lymphoproliferation include hepatosplenic lymphoma, granular lymphocytic leukemia of NK cell or cytotoxic T-cell origin, and other variants of lymphoproliferative disease. This case has many similarities to HSTL as described in humans, typically an infiltrative form of γδ T-cell lymphoma with an aggressive clinical course. As in this canine patient, humans with HSTL generally present with systemic signs and cytopenias; anemia and thrombocytopenia are reported in 84 and 85% of cases, respectively. 17 Concurrent Coombs'-negative hemolytic anemia 10,12,17 and concurrent hemophagocytosis 2,7 have been reported in humans. A case with concurrent hemolytic anemia positive with anti-C3d antibodies and negative with anti-IgG (cold-active) antibodies has also been described. 15
In humans, hepatosplenic γδ T-cell lymphoma occurs predominantly in young men, with a male-to-female ratio of 5 : 1. 4,10 The reason for the predominance in males is unknown. Possible risk factors for developing HSTL include infection with Epstein-Barr virus, immunosuppression, and long-term antigenic stimulation; in cases that have been analyzed cytogenetically, certain chromosomal abnormalities occur with increased frequency, but their exact role in the pathogenesis of the disease is not known. 7,10 Whereas HSTL is the prototypical γδ T-cell lymphoma in humans, especially cells of the Vδ1 subtype, 17 other forms of extranodal γδ T-cell lymphomas may occur, 7 and cases of αβTCR T-cell hepatosplenic lymphoma have been reported. 11
The distribution of disease in this dog was strikingly widespread. Bone marrow involvement is common in humans with HSTL, 7,9,17 but kidney, lung, GI tract, tonsils, and lymph nodes are not common sites. Circulating neoplastic cells are noted in at least 25–50% of human patients during the course of the disease 9 but were not detected in this dog. As seen, neoplastic cells in this dog tended to concentrate in areas of vascular endothelium. Various authors have speculated about the likelihood of neoplastic cells expressing specific surface molecules to explain the tropism of HSTL for certain tissues or tissue compartments, especially endothelial cells of the liver and spleen, but definitive evidence is lacking. 7,10,15 The wide dissemination in this dog may be due in part to the advanced stage of disease. It is also possible that microscopic disease in organs other than liver, spleen, and marrow is under-reported in humans, considering that autopsies have not been performed in some cases. 10
Most cases of HSTL in humans appear to have a primary splenic origin. 17 This can be explained by the consistent finding that γδ T cells in humans normally home preferentially to the splenic red pulp. 3 It is difficult to determine the origin of the tumor in this dog, given the widespread involvement at the time of presentation. However, the tumor cells did express CD11d strongly. In the dog, CD11d is expressed on large granular lymphocytes (LGLs) and on macrophages and T cells in the splenic red pulp. 5,6 Despite their rarity in the blood, CD11d+ γδ T cells constitute more than 30% of splenic T cells in dogs and have an almost exclusive red pulp localization. 13 Therefore, the extensive splenic involvement and the expression of CD11d and the γδ TCR by the malignant cells in this lymphoma suggest a probable (red pulp) splenic origin. Interestingly, canine LGL chronic lymphocytic leukemias that express the γδ TCR invariably express CD11d and are also of primary splenic origin. 16
HSTL in humans typically involves proliferation of double negative (CD4−/CD8−) γδ T cells, with a small subgroup being CD8+. This recapitulates normal biology, as the majority of γδ T cells in humans are also double negative. In contrast, in this case of canine HSTL, the tumor cells expressed CD8α. Canine LGL chronic lymphocytic leukemias and canine mycosis fungoides involving γδ T cells have also been shown to express CD8 most of the time. 14,16
Hemophagocytosis, both by neoplastic γδ T cells and by well-differentiated macrophages, was a prominent feature in this dog. HSTL with concurrent hemophagocytosis is associated with a rapid clinical deterioration in humans. 7 The hemophagocytosis in this dog, together with spherocytosis, suggests an immune-mediated component to the dog's anemia. However, it is not clear whether erythrocyte destruction occurred through a classic antibody-mediated mechanism or, as seems plausible in this Coombs'-negative case, because of hyperactivation of macrophages by cytokines produced by the neoplastic T cells. Direct erythrophagia by the neoplastic cells also likely contributed significantly to the dog's anemia.
The cause of thrombocytopenia in this dog was not clear. Although megakaryocytic hyperplasia was not noted on cytologic examination of the marrow, the increased mean platelet volume suggests regeneration, and the negative AMAT results do not definitively exclude the possibility of immune-mediated destruction of platelets. Another possible mechanism of thrombocytopenia in this dog could be increased levels of inhibitory cytokines produced by or in response to the neoplasm. As noted previously, thrombocytopenia is the most common hematologic abnormality found in humans with HSTL. An immune-mediated pathogenesis has not been shown, and thrombocytopenia was ascribed initially to hypersplenism. However, platelet numbers rarely return to normal after splenectomy. 4 Current hypotheses postulate that cytokines (such as interferon gamma) produced by the malignant T cells may be involved in selective bone marrow suppression. 7,17 The cause of hemorrhage—as indicated by petechiation, melena, positive fecal occult blood test, and erythrocytes in a free-catch urine sample—was not clear but may have involved multiple factors including thrombocytopenia, decreased synthesis of coagulation factors, and paraneoplastic thrombopathy.
This case of γδ T-cell lymphoma in a dog is consistent with the HSTL as described in humans. Physical examination findings, hematologic and biochemical abnormalities, and clinical course of the disease in this patient were similar to those in humans, and immunophenotyping of liver and spleen FNAs supported an antemortem diagnosis of T-cell lymphoma consistent with HSTL. The diagnosis was confirmed postmortem by a combination of routine histopathology, demonstrating a consistent pattern of tissue involvement, and immunohistochemistry showing the T cells to have a γδ TCR phenotype. To our knowledge, this is the first reported case of HSTL in a dog.
Addendum
Since submittal of this report, we have confirmed two additional cases of HSTL in dogs. One dog was a 12-year-old male corgi, and the other was an 11-year-old female spayed mixed-breed. Both dogs presented with anorexia, lethargy, and diarrhea, and splenomegaly was noted clinically in both dogs. Antemortem diagnostics, including immunocytochemistry, indicated a diagnosis of lymphoma in both dogs, most likely HSTL. The neoplastic lymphocytes in one of the dogs (the Corgi) were granular lymphocytes. The neoplastic lymphocytes in the other dog were not. Both dogs were euthanatized because of rapidly deteriorating clinical signs and a poor prognosis. Postmortem examination confirmed hepatosplenomegaly, and HSTL was diagnosed histopathologically on the basis of an extensive and characteristic pattern of infiltration (sinusoidal) in the spleen, liver, and bone marrow with absence of any nodal involvement. The lymphocytes in one case (the Corgi) were CD3+, CD11d+, and TCRγδ+, a characteristic immunophenotype. Lymphocytes in the other case were CD3+ and CD11d+, but TCR expression had not been determined at the time of this writing.
Footnotes
Acknowledgements
We thank David Magliano, Computer Assisted Learning Facility, UC-Davis School of Veterinary Medicine, for help with preparation of photomicrograph images.