
Abstract
A 4-year-old male German Hunting Terrier presented with tremor, dyspnea, trismus, spasms of the musculature of the larynx and pharynx, and hypothermia and subsequently died despite intensive clinical care. Prior clinical signs included vomitus and diarrhea. Microscopic examination of the brain revealed a multifocal nonsuppurative brain stem encephalitis; a few intralesional neurons contained intranuclear inclusions. By immunohistochemistry, Aujeszky disease virus (Suid herpesvirus 1) antigen was detected in neurons in the brain and in ganglion cells of the trigeminal ganglia. Viral culture of brain tissue confirmed the presence of Aujeszky disease virus. Histopathologic findings in the brain with the identification of Aujeszky disease virus by immunohistochemistry and polymerase chain reaction are consistent with Aujeszky disease virus–induced encephalitis. Sequencing revealed a 100% homology of the isolated Aujeszky disease virus with Aujeszky disease virus isolates of wild boar from Eastern Germany.
Keywords
A 4-year-old male German Hunting Terrier presented with tremor, dyspnea, trismus, spasms of the musculature of the larynx and pharynx, and hypothermia. As per clinical history, the dog had been used for hunting 6 days prior to clinical presentation and subsequently showed evidence of clinical disease 3 days later. Prior to the clinical presentation, the dog refused food and water and showed frothy vomitus and bloody diarrhea. All other dogs in the same kennel appeared healthy. The dog was hospitalized but died despite treatment and was submitted for a complete postmortem examination. On macroscopic examination, the only alterations were multifocal acute endocardial petechiae as well as mild diffuse acute pulmonary alveolar emphysema and edema.
Differential Diagnoses
The combined clinical signs (tremor, trismus, spasms of the musculature of the larynx and pharynx, dyspnea, vomitus) were suggestive of a lesion within the brain stem. Due to the sudden onset of clinical symptoms, encephalitis was considered as the primary differential, and a brain tumor was regarded less likely. Causes of encephalitis in dogs include rabies, Aujeszky disease (AKD) and canine distemper, 10 bacterial infections (eg, with Escherichia coli, Streptococcus spp., and/or Klebsiella spp. 17 ), mycotic diseases such as cryptococcosis, 10 and parasitic conditions such as infection with Toxoplasma gondii, Neospora caninum or aberrant migration of Angiostrongylus vasorum larvae. 10 Because of the observed trismus and spasms of the pharyngeal and laryngeal muscles, tetanus was also included in the differentials. 1 Furthermore, exposure to a toxic substance causing gastrointestinal symptoms as well as central nervous signs had to be considered (eg, lead 12 or mercury 4 intoxication). Trismus can also be observed with primary muscle disease, such as masticatory muscle myositis. 14 Because of the reported vomitus and hemorrhagic diarrhea, concurrent gastritis and enteritis had to be ruled out as well.
Microscopic Findings
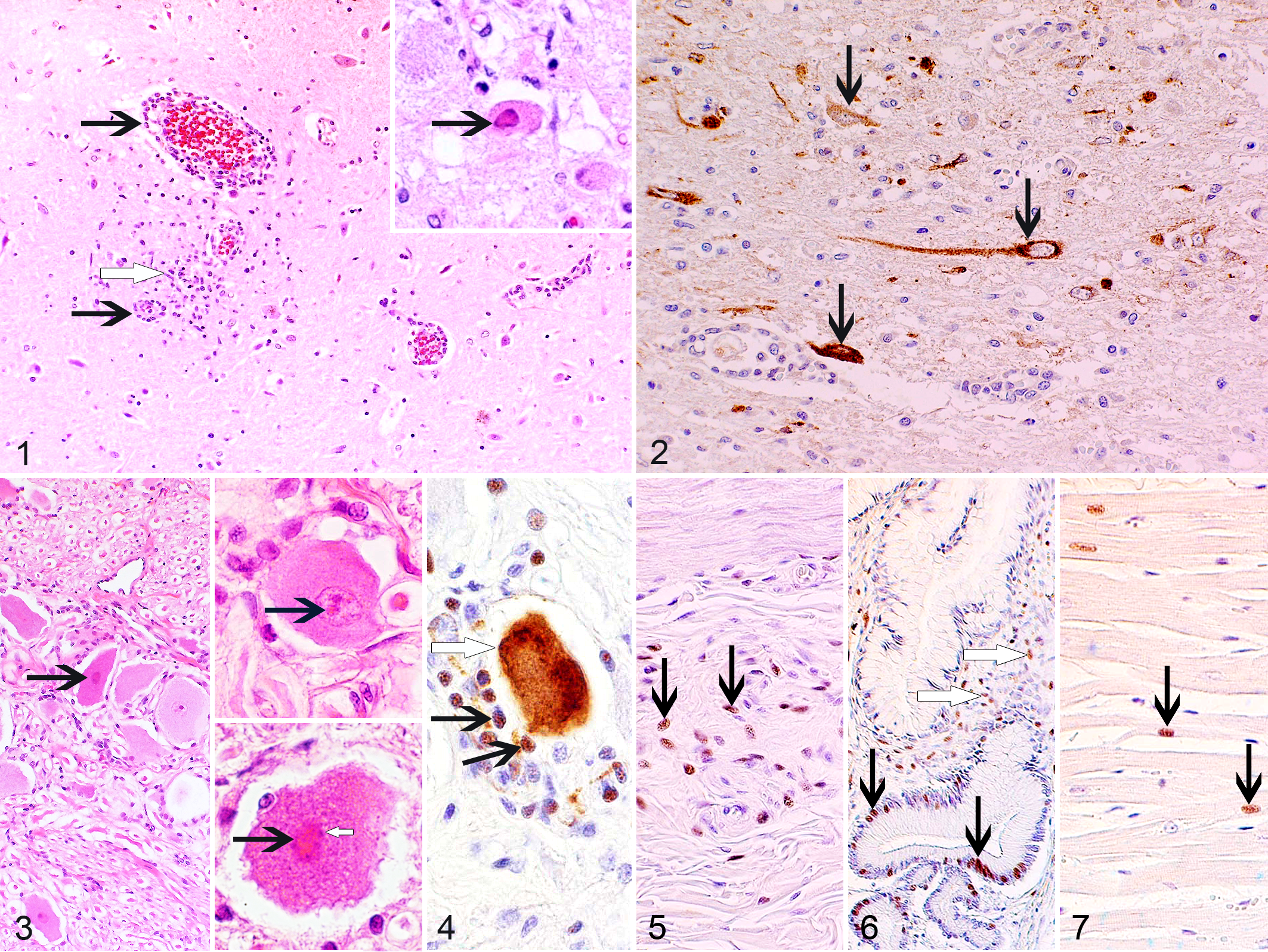
Microscopic examination of the brain revealed a multifocal moderate to marked nonsuppurative encephalitis in the brainstem. The encephalitis was located predominately in the gray matter and was characterized by multifocal perivascular cuffs of lymphocytes, macrophages, and a few plasma cells, as well as multifocal small glial nodules. Within affected areas, a few neurons displayed eosinophilic intranuclear inclusion bodies (Fig. 1). In examined sections of the trigeminal ganglia, rare ganglion cells contained variably sized intranuclear inclusions (Fig. 3). Examined sections of myocardium, left and right masseter muscles, stomach, and intestine showed no histopathologic findings. The microscopic findings in the brain were suggestive of viral encephalitis. Intranuclear inclusion bodies can be observed in canine distemper and AKD. In the present case, infection with AKD virus was regarded as most likely, since only intranuclear inclusion bodies were observed, the intranuclear inclusions were located exclusively in the nucleus of neurons, and there was no demyelination.
Immunohistochemistry and Molecular Diagnostics
By immunohistochemistry, AKD viral antigen was detected in the cytoplasm of neurons within inflamed brain areas (Fig. 2) and of scattered ganglion cells of the trigeminal ganglia (Fig. 4). A positive intranuclear immunoreaction for AKD viral antigen was observed in approximately 40% of satellite cells of the trigeminal ganglia (Fig. 4), approximately 30% of satellite cells of the gastric myenteric plexus (Fig. 5), approximately 30% of glandular epithelial cells and fibrocytes of the gastric mucosa (Fig. 6). and in scattered cardiomyocytes (Fig. 7). AKD viral infection was confirmed by cell culture and polymerase chain reaction on brain tissue. The sequence analysis of a 732-bp fragment (5 k noncoding region of the gC and parts of the open reading frame coding for the N-terminal 223 amino acids of the gC) showed that the identified AKD virus displayed a 100% sequence identity to AKD virus isolates from wild boar (Sus scrofa) in Eastern Germany. Testing for infection with canine distemper virus (polymerase chain reaction) and rabies virus (immunofluorescence) on brain tissue was negative.
Discussion
AKD is caused by infection with Suid herpesvirus 1 (AKD virus, pseudorabies virus). 10 In addition to pigs, its natural (primary) hosts, the virus infects multiple other species, including carnivores. 10,16 In the latter, the disease is usually acutely fatal. 10,16 Since nonfatal disease is almost exclusively observed in pigs, pigs are important as a virus reservoir and for disease transmission. 10,16 Dogs become infected by ingestion of raw meat 2,10,11 or offal from pigs 2 and through contact with infected pigs/pig carcasses. 5,10 Following oronasal infection, the virus is transported by retrograde axonal transport in the central nervous system. 2,10 The virus can also be detected in the blood. 2,10 In dogs, the disease has an incubation time of 2–9 days, 2 and infected dogs usually die within 4 days of the onset of clinical signs. 11 Associated clinical signs include those observed in the present case—that is, trismus, anorexia, vomitus, dyspnea, and muscle spasms. 11 Although unilateral pruritus of the head is considered to be a typical clinical symptom in dogs, 2,5 not all infected dogs develop pruritus. 5,11 Dogs with AKD often show hyperthermia 2 but can also develop terminal hypothermia. 18 In dogs, the disease is not associated with diagnostic macroscopic lesions. 10 Severe pruritus, however, can cause mechanical trauma and automutilation. 2,3 The typical microscopic finding in dogs is a nonsuppurative encephalitis with glial nodules and occasional intranuclear inclusions in neurons and astrocytes; 3,10 the brain stem is commonly affected. 3,5 Occasionally, small areas of hepatic necrosis can be detected. 5 In addition, microscopic alterations (hemorrhages, myocardial degeneration, myolysis, and/or ganglioneuritis) are described in the hearts of experimentally infected dogs. 15 Viral antigens can be located in the nucleus and/or cytoplasm of infected cells. 8,9
Eradication of AKD in domestic pigs has been achieved in multiple countries, including Germany, Sweden, Austria, Denmark, United Kingdom, and the United States. 7,16 Thus, nowadays the disease is rarely observed in domestic animals. Viral presence, however, has been confirmed in populations of wild boar in Germany 13 and multiple other countries, including Italy 16 , France 16 and in feral pigs in the United States. 7 Sporadic cases of AKD have been diagnosed in hunting dogs in Germany 13 and France. 13 In the United States, AKD virus was isolated from a dead Florida Panther, and disease transmission from feral pigs was suspected. 6 Thus, AKD has to be considered as an important differential for central nervous disease in domestic and wild animals with contact to feral pigs or wild boar.
Footnotes
Acknowledgements
We thank Maritta Wipplinger and Hilke Gräfe for performing the immunohistochemistry. We are grateful to Dr. Lucy Woolford for the critical review of the manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.