
Abstract
The aim of the present study was to determine which histopathologic parameters of primary canine mammary carcinomas (CMCs) could predict metastatic spread via the lymphatic system. A modification of the World Health Organization classification was applied to 245 CMCs. In addition to tumor subtype, neoplastic infiltration of the surrounding mammary stroma, vasculogenic mimicry, and micropapillary pattern were evaluated, and 2 histologic grading systems were used for each sample. A statistical analysis was undertaken to determine the relationship between these histopathologic parameters and the detection of lymphatic vessels invasion (LVI) and regional lymph node metastases (RLM). To compare the predictive value for lymphatic spread of the 2 histologic grading systems, the Akaike information criterion was measured. The classification into tumor subtypes was significant (P < .01) in predicting the risk of LVI and RLM. Peripheral infiltration, vasculogenic mimicry, and micropapillary pattern were found in 170 of 245 (69.4%), 32 of 245 (13.1%), and 54 of 245 (22.0%) CMCs. The presence of peripheral infiltration was significantly associated (P < .001) with both LVI and RLM, and a similar relation (P < .05) was found for the micropapillary pattern. Vasculogenic mimicry was not predictive of invasion of the lymphatic system. Both histologic grading systems were significant predictors (P < .001) of the risk of LVI and RLM. The grading system that included a more rigorous evaluation of the neoplastic mitotic activity had the lower Akaike information criterion values, thus indicating a better predictive ability. The study confirms the significant prognostic role for the modified World Health Organization classification of CMCs and the prognostic value of additional histopathologic parameters.
Mammary tumors are the most common tumors of intact female dogs. Forty to fifty percent of cases are considered malignant, with carcinomas being the most common malignant type. 26,39 After mastectomy, the main cause of death in dogs with mammary carcinoma is metastatic disease. Canine mammary carcinomas (CMCs) usually metastasize through the lymphatic system to the regional lymph nodes and subsequently to the lung or, less frequently, other organs (liver, kidneys, spleen, and bone). 6,26,39 In dogs, as in human cases of breast cancer, the histopathologic detection of lymphatic vessels invasion (LVI) and/or regional lymph node metastases (RLM) is associated with poor survival after surgery. 5,7,19,21,22,44
The International Histological Classification of Mammary Tumours of the Dog and the Cat, published in 1999 by the World Health Organization (WHO) and usually applied in veterinary diagnostic pathology, is based partly on prognostic information and recognizes several morphologic subtypes of CMCs. 27 However, CMCs are highly heterogeneous on histomorphology. Recently, additional morphologic subtypes of CMCs with specific histologic and clinical features have been described, and it has been suggested that they be incorporated into the WHO classification. 4,16,32
An infiltrative pattern of growth in CMCs has been documented as a prognostic factor in most univariate analyses. 26 In human breast cancer, other histologic features that, independent of the tumor subtypes, are considered signs of aggressiveness are vasculogenic mimicry (neoplastic cells generate microvascular channels) and a micropapillary pattern (neoplastic cells form small papillae lacking a fibrovascular core). 37,40
For CMCs, the histologic grade of malignancy is of prognostic significance, and many authors have suggested that it be routinely included in the pathology report. 21,26 There are several systems used to assign a histologic grade to CMCs; most are a modification of the method of Ellston and Ellis used for human breast cancers. 6,21,26 In dogs, the predictive value of each specific grading system has not been assessed.
The aim of the present study was to determine which histopathologic parameters could predict the metastatic potential of primary CMCs. In this study, the morphologic subtypes, the presence of peripheral infiltration, vasculogenic mimicry, a micropapillary pattern, and the grade of malignancy were evaluated. Two hundred forty-five CMCs were classified using a modification of the WHO classification that integrates the new morphologic subtypes. The CMCs were graded using 2 histologic grading systems, 6,27 which were compared. The relationship between all the above histologic parameters and the detection of LVI and RLM was evaluated.
Materials and Methods
Sample Collection, Histopathology, and Immunohistochemistry
Two hundred forty-five cases of CMCs submitted to the surgical pathology service of the Laboratory of Pathology and Toxicology at the University of Pennsylvania’s School of Veterinary Medicine between January 2000 and December 2009 were selected for this study. The mammary neoplasms had been surgically resected from 245 female dogs, fixed in 10% buffered formalin, and routinely processed for histopathology. The cases were selected because regional lymph nodes were also submitted for histopathologic evaluation (127 cases) or because carcinoma cells were identified within lymphatic vessels within or adjacent to the mammary neoplasm (118 cases). The cases were reviewed by 2 pathologists, and CMCs were reclassified on the basis of a modified WHO classification
17
that integrated 5 new morphologic subtypes:
Micropapillary invasive carcinoma: an invasive carcinoma displaying more than 50% of micropapillary pattern
4,16,27
Comedocarcinoma: a multilobulated not in situ carcinoma with huge and well-demarcated central necrotic areas involving more than 50% of the neoplastic cell population
Ductal carcinoma: a carcinoma with neoplastic cells arranged in cords lined by a double layer of cells that surround slitlike lumina, usually with focal/multifocal areas of pluristratified squamous epithelial differentiation—the malignant counterpart of the ductal adenoma
Intraductal papillary carcinoma: a carcinoma composed of intraductal papillary projections supported by a fibrovascular stalk—the malignant counterpart of the duct papilloma
Carcinoma and malignant myoepithelioma: a tumor composed of a malignant epithelial cell population and a malignant myoepithelial population—the latter is frequently very pleomorphic and requires immunohistochemistry for confirmation
In addition to the classification into morphologic subtypes, 3 other specific histologic characteristics were evaluated: infiltration by neoplastic cells of the surrounding mammary gland stroma, vasculogenic mimicry, and a micropapillary pattern. All the tumors were graded according to 2 systems proposed by Misdorp
16
and Clemente et al,
6
as summarized in Table 1 and Table 2. Both systems assess the degree of tubule formation, nuclear pleomorphism, and the mitotic activity of carcinoma cells.
Histologic Grading System From Misdorp et al26
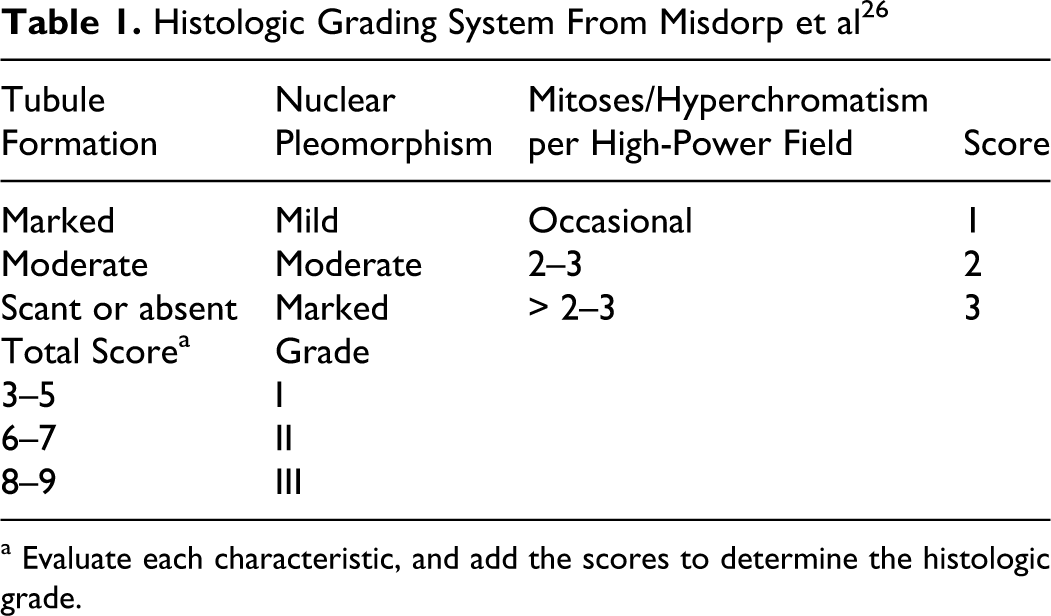
a Evaluate each characteristic, and add the scores to determine the histologic grade.
Histologic Grading System From Clemente et al6
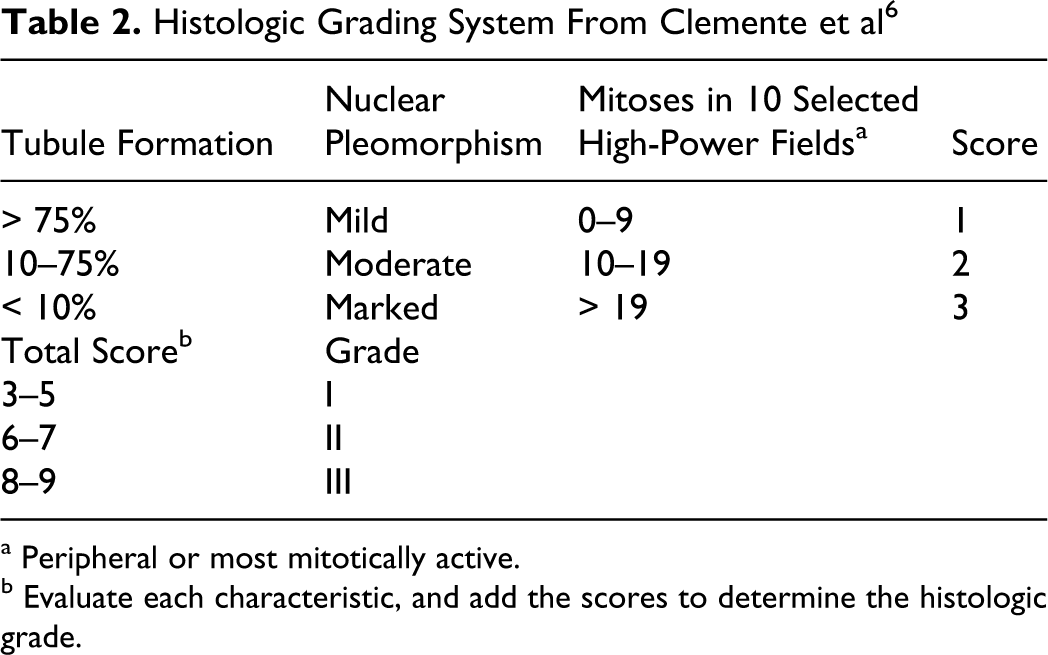
a Peripheral or most mitotically active.
b Evaluate each characteristic, and add the scores to determine the histologic grade.
Immunohistochemistry was used in 18 of the 245 cases to help classify these neoplasms. An immunohistochemical panel of antibodies against cell differentiation markers was applied and included cytokeratin (CK) 8/18 (1:30, NCL-L-5D3, Novocastra, Newcaste Upon Tyne, United Kingdom), CK 14 (1:20, NCL-LL 002, Novocastra), p63 (1:200, 4A4, Santa Cruz Biotechnology Inc., Heidelberg, Germany), calponin (1:200, CALP, Dako, Glostrup, Denmark), and vimentin (1:150, V9, Dako). In ducts and lobules of normal canine mammary glands, CK 8/18 is expressed by luminal epithelial cells, while CK 14, p63, calponin, and vimentin stain the basal/myoepithelial cells. In addition, vimentin is expected to mark the intralobular and interlobular stroma, and p63 and CK 14 have been hypothesized to stain stem/progenitor cells of the mammary gland. 1,2,9,25,43 An automated immunostainer (BenchMark, Ventana Medical System Inc., Tucson, AZ) was used. Epitope retrieval was heat mediated (95°C for 30 minutes) for CK 14, calponin, p63, and vimentin and enzymatic (Ventana Protease 1 for 8 minutes) for CK 8/18. Immunoreactivity was visualized using the ultraView Universal DAB Detection Kit (Ventana Medical System Inc.). Internal positive controls were the normal mammary tissue at the periphery of the CMCs (CK 8/ 18, CK 14, and p63), the smooth muscle cells of blood vessels (CALP), and the connective tissue stroma (vimentin). For negative controls, the primary antibody was replaced with a commercial antibody diluent (Ventana Medical System Inc.). The immunostaining (nuclear for p63 and cytoplasmic for CK 8/18, CK 14, calponin, and vimentin) was described as the percentage of positive cells, counting 1000 cells in at least 10 high power fields (400×). The intensity (mild, moderate, marked) of the immunostaining was also evaluated.
Statistical Analyses
To evaluate if tumor subtypes, peripheral infiltration, vasculogenic mimicry, micropapillary pattern, and both histologic grading systems were good parameters to predict LVI and RLM of primary CMCs, several generalized linear models (GLM) with binomial distribution and a logit link function were performed. Response variables were presence/absence of LVI and RLM. The first 2 models tested the capacity of the classification into tumor subtypes to explain the presence/absence of LVI and RLM. In the analyses, some tumor subtypes were grouped on the basis of their similar morphologic features. Particularly, complex carcinomas were grouped with carcinomas arising in benign mixed tumors, and simple tubular carcinomas were grouped with simple tubulopapillary carcinomas. Invasive micropapillary carcinomas, adenosquamous carcinomas, intraductal papillary carcinomas, lipid-rich carcinomas, and carcinosarcoma were excluded from the statistical analysis because of the small number of cases available. Six other models were used to test the ability of peripheral infiltration, vasculogenic mimicry, and micropapillary pattern to predict the presence of both LVI and RLM. Four other models investigated the associations between the 2 grading systems and both LVI and RLM. In addition, to compare the ability of the 2 grading systems to predict the presence of LVI and RLM, the Akaike information criterion (AIC) was measured. Briefly, the lower the AIC value, the smaller the loss of information (parsimony with maximum likelihood), indicating a better goodness of fit of the statistical model. Therefore, the best histologic grading system for predicting LVI and RLM was expected to be the one achieving the lowest AIC values. Finally, to identify the minimum adequate model to predict LVI and RLM, the most significant parameters were simultaneously tested in a single model using a backward selection procedure. Level of significance was fixed at P < .05.
Results
Animals
The 245 female dogs bearing the 245 CMCs selected for this study were of 52 different breeds and ranged from 5 to 19 years of age (mean, 7.09 years). At the time of diagnosis, 135 of 245 (55.1%) dogs were intact and 110 of 245 (44.9%) were spayed.
Classification of CMCs Into Tumor Subtypes: Histopathology and Immunohistochemistry
On histopathology, the percentages of subtypes diagnosed were comedocarcinoma (50 of 245, 20.4%), simple tubular carcinoma (45 of 245, 18.4%), simple anaplastic carcinoma (36 of 245, 14.7%), simple solid carcinoma (31 of 245, 12.6%), simple tubulopapillary carcinoma (28 of 245, 11.4%), complex carcinoma (10 of 245, 4.1%), ductal carcinoma (7 of 245, 2.9%), carcinoma arising in benign tumor (5 of 245, 2%), invasive micropapillary carcinoma (5 of 245, 2%), adenosquamous carcinoma (4 of 245, 1.6%), intraductal papillary carcinoma (3 of 245, 1.3%), and lipid-rich carcinoma (3 of 245, 1.3%). In comedocarcinomas, the well-defined lobular areas forming the tumor typically had well-demarcated and central necrotic foci characterized by an abundant amorphous eosinophilic material admixed with cell debris, neutrophils, macrophages, and red blood cells (Fig. 1). The surrounding neoplastic cells had a solid (32 of 50, 64%) or tubulopapillary (18 of 50, 36%) organization with a high number of mitoses. In simple tubular carcinomas and in simple tubulopapillary carcinomas, the cells were columnar to cuboidal with variable nuclear pleomorphism. In simple tubular carcinomas, the cells were columnar to cuboidal with variable nuclear pleomorphism and were almost exclusively arranged in tubules (Fig. 2) with very few areas of papillae formation. In simple anaplastic carcinomas, the cells were usually individualized or grouped in small nests and were polygonal to round, with moderate to abundant occasionally vacuolated cytoplasm. Anisocytosis and anisokaryosis were marked (Fig. 3). Karyomegaly, multinucleation, and atypical mitoses were also evident in this tumor subtype. In simple tubulopapillary carcinomas, cells were usually columnar with equally represented areas of tubular and papillary formation (Fig. 4). Simple solid carcinomas were composed of a dense population of polygonal cells. These cells were mainly arranged in nests (Fig. 5) and cords forming irregularly sized lobules, and only rare tubules and/or papillae were found in very small areas of the tumors. In complex carcinomas, the distinctive feature was the presence of interstitial bundles and whorls of well-differentiated spindle cells (myoepithelial cells) admixed with the malignant epithelial component. Myoepithelial cells were usually embedded in a moderate to abundant basophilic matrix and showed mild anisocytosis and anisokaryosis with rare or absent mitoses. Similarly, in carcinomas arising in benign mixed tumors, myoepithelial proliferation was detected in addition to multifocal areas of cartilaginous and/or osseous differentiation. In invasive micropapillary carcinomas, the characteristic small papillae lacking a fibrovascular core were composed of cuboidal to polygonal cells with an intensely eosinophilic cytoplasm and were occasionally surrounded by empty lacunae. In ductal carcinomas, in addition to the double layering of cuboidal cells with hyperchromatic nuclei (Fig. 6), a clear association with the double-layered wall of an ectatic duct was present. In ductal carcinomas, there were often areas of pluristratified squamous epithelial differentiation associated with the duct lumina, which was different from the disorganized squamous metaplasia occasionally found in other tumor subtypes. The cells lining the papillary projections of the intraductal papillary carcinomas were columnar with open-faced nuclei, and there was always an association with the wall of an ectatic duct. The presence of clear cytoplasmic vacuoles in cells exhibiting a solid arrangement were features typically recognized in the lipid-rich carcinoma, and the combination of tubules formation and foci of malignant squamous differentiation was a feature of adenosquamous carcinomas. The remaining 18 of 245 CMCs (7.3%) were not precisely classified at histopathology, because in these cases the carcinomatous component—which was arranged in tubules, papillae, and small nests—was admixed with a second population of pleomorphic (spindle to round to polygonal) malignant cells of unknown origin. These pleomorphic cells—organized in sheets, nests, or thick bundles that expanded the interstitium—often had a scant eosinophilic or vacuolated cytoplasm and a round hyperchromatic nucleus with a single nucleolus (Fig. 7a). These cells showed moderate to severe anisokaryosis and a variable number of mitoses. In 6 of 18 cases (33.3%), these pleomorphic cells were multifocally embedded in a scant, lightly basophilic matrix. Immunohistochemically, in 18 of 18 cases (100%), the carcinomatous component was, as expected, CK 8/18 positive (Fig. 7b) with mild to marked immunostaining of 100% of the cells. Rare (from 1 to 10%) carcinoma cells were also CK 14 positive (Fig. 7c) with a mild to moderate immunostaining. The intermingling pleomorphic cell population was CK 8/18 negative (Fig. 7b) and simultaneously positive for vimentin, CK 14 (Fig. 7c), calponin, and p63 in 17 of 18 (94.4%) cases. In these cases, the immunostaining was moderate to marked with some variability in the percentage of pleomorphic cells that stained positive (from 20 to 100%), depending on the marker and the case. In only 1 of 18 cases (5.6%), the pleomorphic malignant population was exclusively vimentin positive with marked immunostaining of 100% of the cells. According to the histopathology and immunohistochemistry, we identified 17 of 245 cases (6.9%) as carcinomas and malignant myoepitheliomas (pleomorphic population reactive for vimentin, CK 14, calponin, and p63) and 1 of 245 (0.4%) as a carcinosarcoma (pleomorphic population reactive exclusively for vimentin).
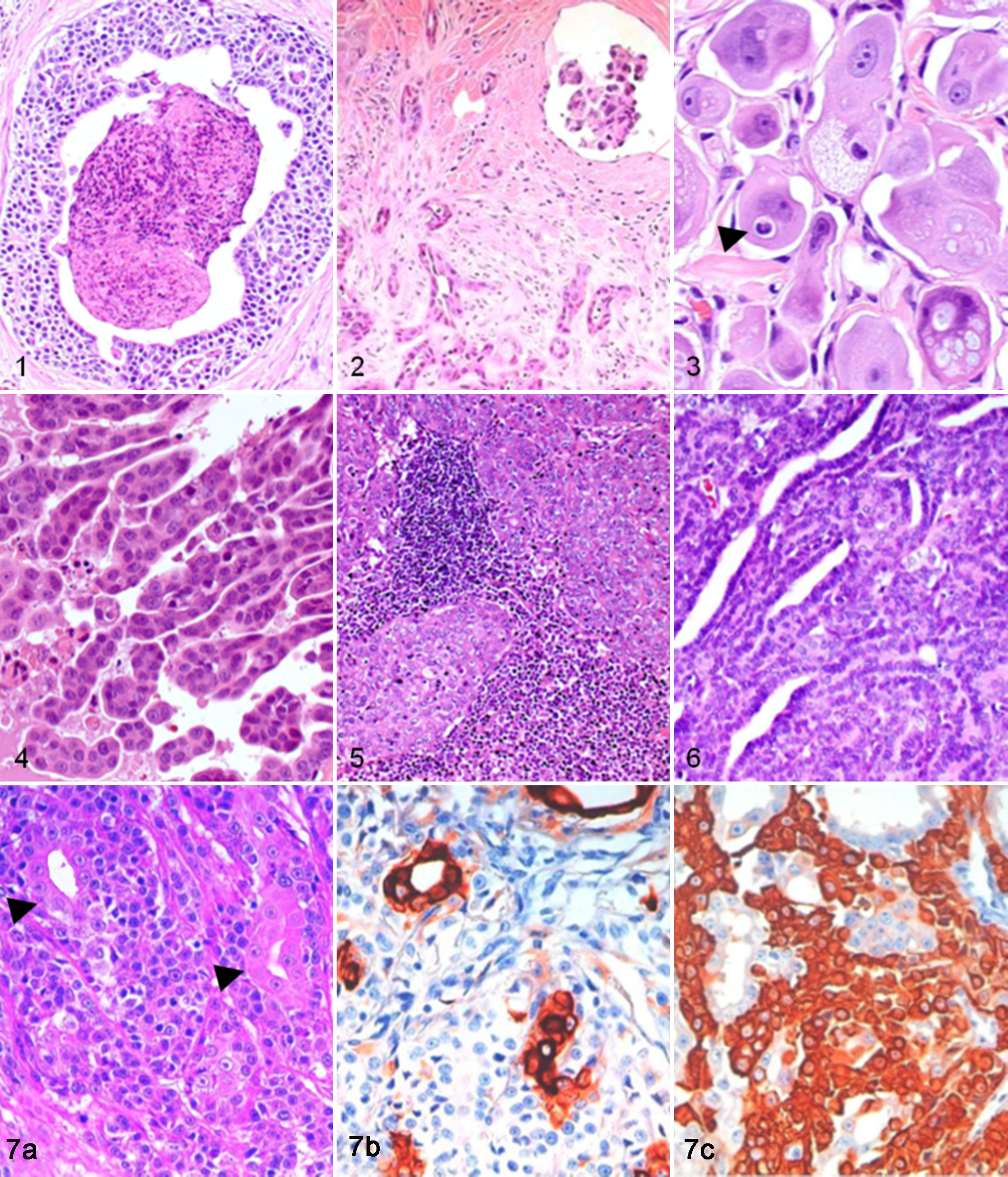
Comedocarcinoma; mammary gland; dog. Well-defined lobular area composed of neoplastic cells arranged in tubules surrounding a well-demarcated central necrotic focus, HE.
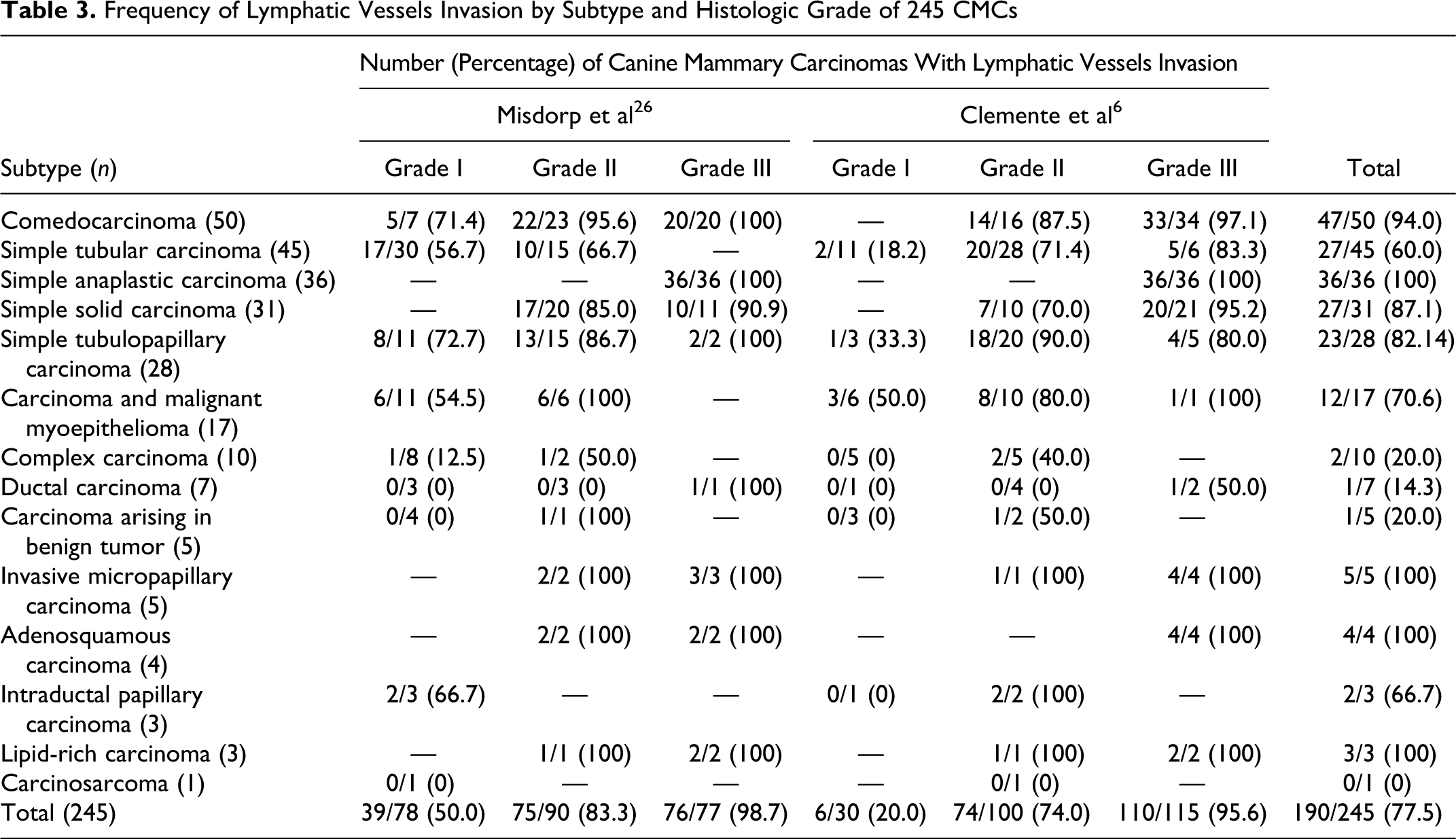
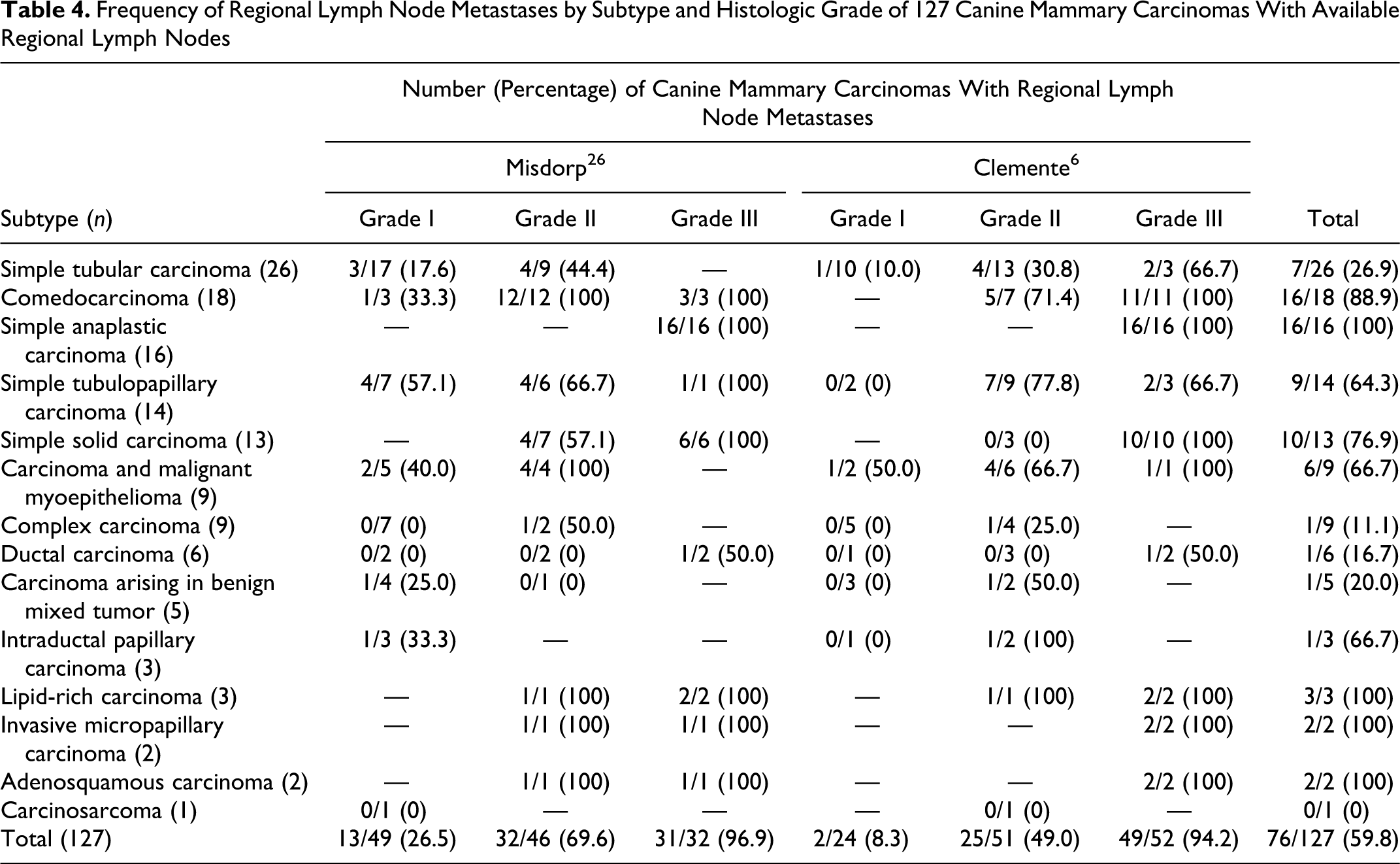
Of 245 CMCs, 190 (77.5%) showed LVI. Regional lymph nodes were available from 127 dogs, and RLM were found in 76 of 127 cases (59.8%). RLM was always associated with presence of LVI, except for 4 of 76 cases (5.3%), which had RLM without LVI. These 4 CMCs were a comedocarcinoma, a simple solid carcinoma, a carcinoma and malignant myoepithelioma, and a carcinoma arising in benign mixed tumor. When LVI was identified and the regional lymph nodes were available (74 cases), RLM were confirmed with the exception of 2 of 74 cases (2.7%): a simple tubular carcinoma and a carcinoma arising in benign mixed tumor. The incidence of LVI and RLM for each tumor subtype is shown in Table 3 and Table 4, respectively. The highest incidence was found with simple anaplastic carcinomas, invasive micropapillary carcinomas, adenosquamous carcinomas, and lipid-rich carcinomas, followed by comedocarcinomas, simple solid carcinomas (Fig. 5), and simple tubulopapillary carcinomas. LVI or RLM was also found in cases of carcinoma and malignant myoepithelioma, intraductal papillary carcinoma, and simple tubular carcinoma. Conversely, complex carcinomas, ductal carcinomas, and carcinomas arising in benign tumors rarely or never showed LVI or RLM.
Frequency of Lymphatic Vessels Invasion by Subtype and Histologic Grade of 245 CMCs
Frequency of Regional Lymph Node Metastases by Subtype and Histologic Grade of 127 Canine Mammary Carcinomas With Available Regional Lymph Nodes
In general, neoplastic cells found within the lumen of the lymphatic vessels or in the regional lymph nodes had an arrangement and cytomorphologic features similar to the cells of the correspondent primary CMCs. In cases of carcinoma and malignant myoepithelioma, neoplastic emboli could be composed of malignant myoepithelial cells (5 of 12, 41.7%), carcinoma cells (1 of 12, 8.3%), or both (6 of 12, 50%). The lymph node metastases of this tumor subtype consisted only of malignant myoepithelial cells in 2 of 6 cases (33.3%) and of both cell populations in 3 of 6 cases (50%). Conversely, neoplastic emboli of complex carcinomas were composed only of carcinoma cells in 2 of 2 cases (100%) without any participation of the myoepithelial component.
In 39 of 190 cases (20.5%) with LVI (13 simple anaplastic carcinomas, 7 simple tubular carcinomas, 7 simple solid carcinomas, 5 comedocarcinomas, 4 simple tubulopapillary carcinomas, and 3 invasive micropapillary carcinomas), the neoplastic emboli were also present within dermal lymphatic vessels.
Infiltration, Vasculogenic Mimicry, and Micropapillary Pattern
Of 245 CMCs, 170 (69.4%) showed infiltration by neoplastic cells of the surrounding mammary gland stroma. For each tumor subtype, the number of cases of infiltrating CMCs is shown in Table 5. An infiltrative growth was always seen in simple anaplastic carcinomas and in invasive micropapillary carcinomas and was detected in the majority of comedocarcinomas, adenosquamous carcinomas, simple solid carcinomas, and simple tubular carcinomas (Fig. 2). In most cases (103 of 170, 60.6%), the neoplastic infiltration was marked, diffuse, and associated with desmoplasia (Fig. 2). Occasionally, in simple anaplastic carcinomas and in simple tubular carcinomas, the infiltrating neoplastic cells were seen as single cells or in small aggregates of cells, and a careful search was often necessary to distinguish them from the admixed plumped stromal fibroblasts of the desmoplastic reaction. Infiltrating tumors were more commonly associated with LVI than noninfiltrating tumors (151 of 170 [88.8%] vs 37 of 75 [49.3%]). There was also an increased frequency of RLM in those dogs with infiltrating CMCs (54 of 70, 77.1%) compared with dogs with noninfiltrating CMCs (22 of 57, 38.6%).
Infiltration, Vasculogenic Mimicry, and Micropapillary Pattern in Relation to Tumor Subtype for 245 Canine Mammary Carcinomas
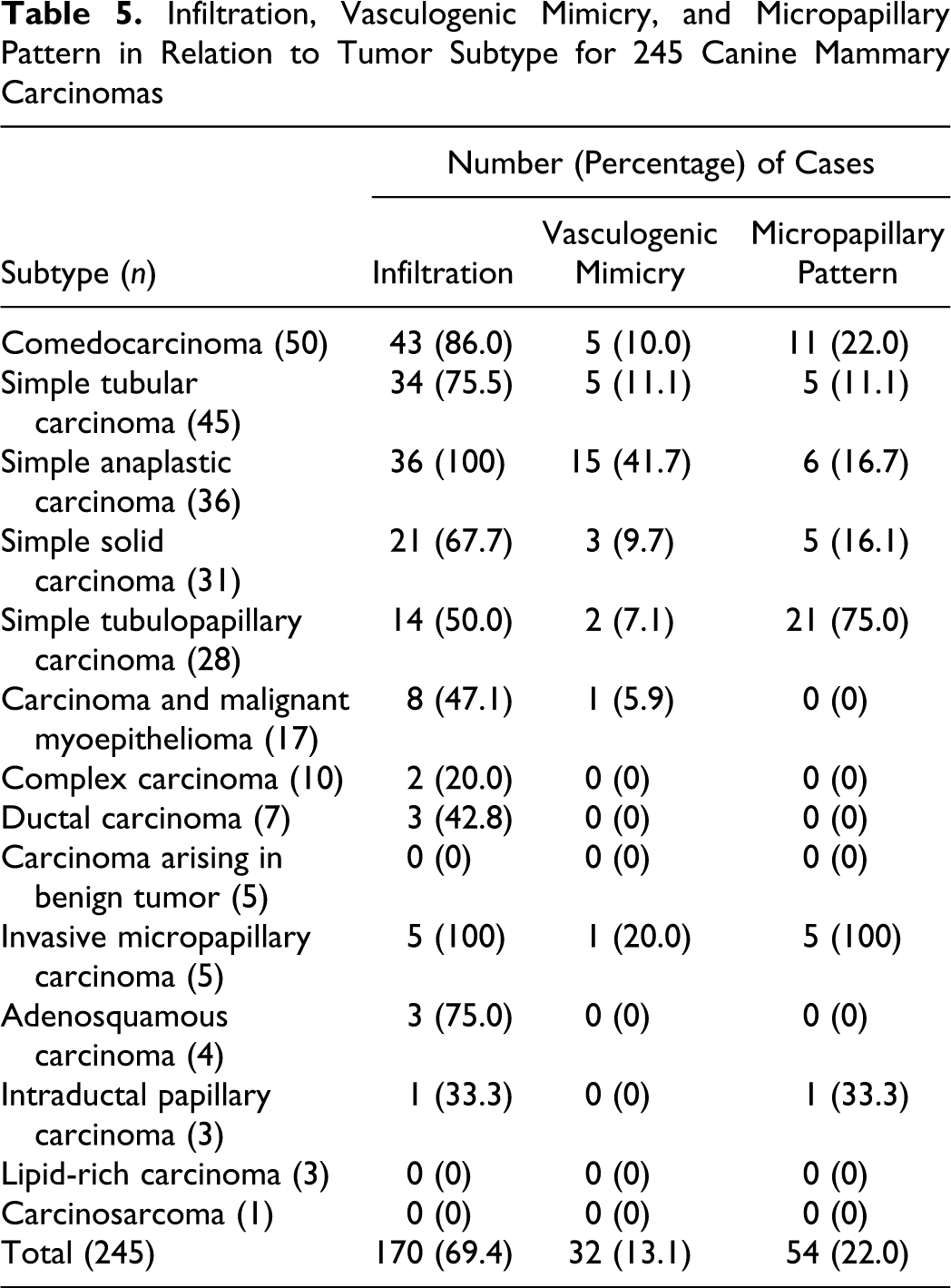
Vasculogenic mimicry was observed in 32 of 245 CMCs (13.1%). It was characterized by individual neoplastic cells with a single cytoplasmic channel (Fig. 3) or by groups of neoplastic cells (2–4 cells) radially arranged around a larger channel. These channels contained granulocytes and erythrocytes (Fig. 3) and, less frequently, other neoplastic cells. In simple anaplastic carcinomas, vasculogenic mimicry, observed in 15 of 36 cases (41.7%), appeared to be relatively common compared with the other subtypes (Table 5). The rate of LVI was higher for CMCs exhibiting vasculogenic mimicry (30 of 32, 93.7%) compared with neoplasms not presenting this feature (159 of 213, 74.6%). The regional lymph nodes of dogs with CMCs showing vasculogenic mimicry (n = 16) compared with those of dogs with CMCs not exhibiting this feature (n = 111) more frequently had RLM (15 of 16 [93.7%] vs 61 of 111 [54.9%]).
A micropapillary pattern was found in 54 of 245 CMCs (22%). In addition to the invasive micropapillary carcinoma—that is, by definition, characterized by a micropapillary arrangement involving more than 50% of the neoplastic population—other morphologic subtypes that sometimes have a micropapillary pattern either focally or multifocal within the tumor were simple tubulopapillary carcinomas (Fig. 4), intraductal papillary carcinomas, comedocarcinomas, simple anaplastic carcinomas, simple solid carcinomas, and simple tubular carcinomas (Table 5). Tumors exhibiting this micropapillary pattern more frequently had LVI than tumors not having this feature (48 of 54 [88.9%] vs 142 of 191 [74.3%]). The regional lymph nodes of dogs with CMCs exhibiting the micropapillary pattern (n = 24) compared with those of dogs with CMCs without this feature (n = 103) more frequently had RLM (19 of 24 [79.2%] vs 57 of 103 [55.3%]).
Histologic Grading
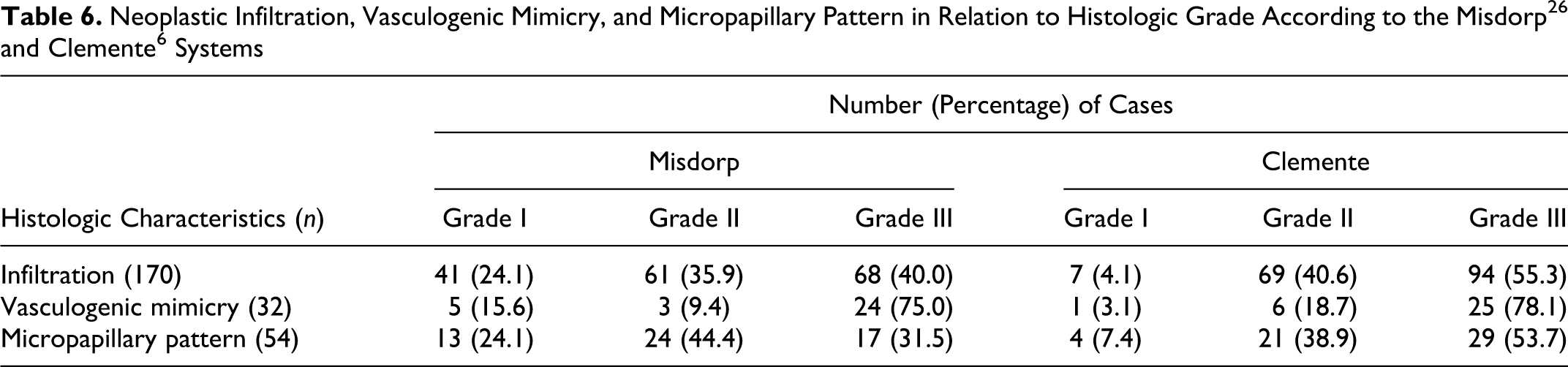
The classification of the CMCs using the 2 histologic grading systems is reported in Tables 3 and 4. There was agreement between the 2 systems that all simple anaplastic carcinomas were grade III tumors. Simple solid carcinomas, invasive micropapillary carcinomas, and lipid-rich carcinomas were either grade II or grade III tumors. Complex carcinomas, carcinomas arising in benign tumors, and intraductal papillary carcinomas were classified as grade I or grade II tumors using both the grading systems. Independent of the grading system used, grade III tumors more frequently showed infiltration and vasculogenic mimicry than grade I and grade II tumors. A similar trend was noted for the micropapillary pattern when the grading was performed according to Clemente and coauthors, but when the Misdorp system was used, the micropapillary pattern was more commonly seen in grade II tumors (Table 6).
Neoplastic Infiltration, Vasculogenic Mimicry, and Micropapillary Pattern in Relation to Histologic Grade According to the Misdorp26 and Clemente6 Systems
The Clemente system, when compared with the Misdorp system, identified a greater number of grade III tumors and a lower number of grade II and grade I tumors when the 190 CMCs with LVI and the 76 CMCs with RLM were evaluated (Tables 3 and 4).
The 4 CMCs with RLM without signs of LVI were grade I (2 of 4, 50%), grade II (1 of 4, 25%), and grade III (1 of 4, 25%) when using the Misdorp system but were grade II (2 of 4, 50%) and grade III (2 of 4, 50%) when using the Clemente system. The 2 CMCs with LVI but without demonstration of metastases in the regional lymph node were grade I and grade II using the Misdorp and Clemente systems, respectively.
The frequencies of LVI and RLM in relation to histologic grade and subtype are shown in Table 3 and Table 4. With both grading systems, an increase in the frequencies of LVI and RLM was observed from grade I to grade II to grade III tumors. When the results of the 2 systems are compared, the most important differences are the frequency of LVI by grade I tumors, which were 50% and 20% using the Misdorp and Clemente systems, respectively. The grade I tumors identified with the Misdorp system have a higher frequency of LVI for some specific subtypes: simple tubulopapillary carcinoma, comedocarcinoma, intraductal papillary carcinoma, simple tubular carcinoma, and carcinoma and malignant myoepithelioma (Table 3).
Statistical Results
The first 2 binomial GLM indicated that classification into tumor subtypes was significant in predicting the risk of both LVI and RLM (P < .01). The presence of infiltration was also significantly associated (P < .001) with LVI and RLM. Similarly, a positive relationship (P < .05) was found for LVI and RLM when there was a micropapillary pattern associated with the neoplasm. However, vasculogenic mimicry was found not to be predictive of invasion of the lymphatic system. The binomial GLM that tested the 2 histologic grading systems on LVI and RLM found that both grading systems were significant predictors of invasion of the lymphatic system. Specifically, the Clemente system performed better, having the lower AIC values (Table 7).
Generalized Linear Models Testing the Association Between the 2 Histologic Grading Systems and Lymphatic Vessels Invasion and Regional Lymph Node Metastases a
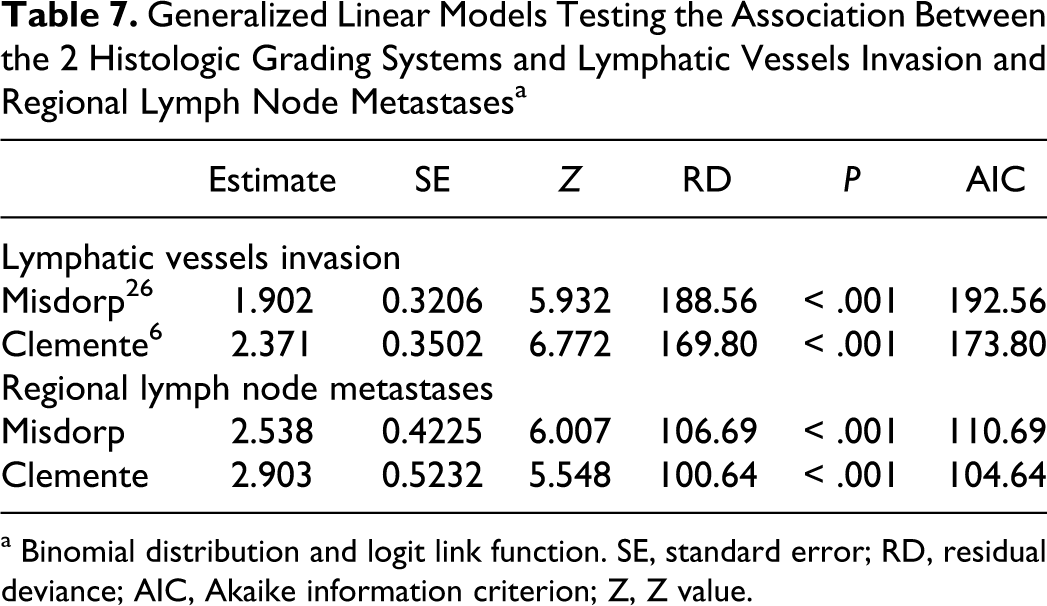
a Binomial distribution and logit link function. SE, standard error; RD, residual deviance; AIC, Akaike information criterion; Z, Z value.
To identify the minimum adequate model to predict both LVI and RLM, the classification into tumor subtypes, infiltration, micropapillary pattern, and Clemente system were simultaneously tested in a single model using a backward selection procedure. All the 4 variables remained significant (all variables with P < .05). Therefore, the best model for predicting both LVI and RLM was evaluating the tumor subtype in conjunction with local infiltration, a micropapillary pattern, and the tumor grade using the Clemente system.
Discussion
Histopathologic examination is considered the gold standard for the diagnosis of CMCs. However, there is little agreement about what information should be included in the pathologist’s report to the clinician, as well as its prognostic significance. 26,31 In the present study, we evaluated different histopathologic parameters on a large group of primary CMCs. A statistical analysis was undertaken to determine which parameters were associated with LVI and RLM.
The first parameter examined was the classification of CMCs into morphologic subtypes. The WHO classification published in 1999 recognized different subtypes, and for some of them behavioral differences were noted. The percentage of dogs surviving 2 years after surgery decreased from simple carcinomas in situ to simple tubulopapillary carcinomas to simple solid carcinomas to simple anaplastic carcinomas. 2,3,5,27 In addition, studies have shown that simple carcinomas are more aggressive tumors than complex carcinomas. 27,28 The modification of the WHO classification used in the present study was found to be a good tool for predicting the metastatic potential of CMCs. Within the group of simple carcinomas, the cell arrangement on histopathology was important because an increase in the metastatic tendency was observed from tubular to tubulopapillary to solid to anaplastic tumors. Two other subtypes were recognized that had significant metastatic potential but were not included in the prior WHO classification: the comedocarcinoma and the carcinoma and malignant myoepithelioma. The central necrotic areas are interpreted as an indication that the neoplastic cells are growing faster and that there is therefore a higher risk of progression to invasive carcinoma. 41,42 The comedo appearance was mentioned in the WHO classification as a feature occasionally detectable in CMC in situ. 27 Those comedocarcinomas identified in the present study were not in situ lesions. The majority of the cases were seen to be infiltrating into the surrounding mammary gland stroma, suggesting a more advanced stage of tumor progression, presumably related to a faster growth. The neoplastic cells that surrounded the areas of necrosis were arranged in a solid or tubulopapillary pattern. These neoplasms, with their comedo pattern of necrosis, despite the solid or tubulopapillary cell arrangement, should be considered as a unique specific entity, with an increased likelihood of LVI and RLM.
Carcinoma and malignant myoepithelioma is an additional subtype not originally included in the WHO classification. For this tumor subtype, immunohistochemistry was necessary to confirm the presence of pleomorphic myoepithelial cells, which lacked their classic morphologic appearance on histopathology. Carcinomas and malignant myoepitheliomas were more aggressive than complex carcinomas and carcinomas arising in benign mixed tumors, which in this and other studies have shown a low tendency to metastasize. The relatively aggressive behavior of carcinomas and malignant myoepitheliomas and their expression of CK 14 and p63, considered by many authors as a stem/progenitor cell marker, might indicate that there is, in this tumor, proliferation of a relatively undifferentiated myoepithelial component, similar to that identified in the basal-like breast cancers of women. 33,34,36 The role of the myoepithelial cells in the carcinogenetic process of human and canine mammary glands is still debatable. There is in vitro evidence to suggest that differentiated myoepithelial cells might be “natural tumor suppressors” inhibiting the growth and invasion of neoplastic epithelial cells. 10,13,27,29 Furthermore, differentiated myoepithelial cells that proliferate within the interstitium show decreased expression of CK14, p63 and calponin and an enhanced expression of vimentin. 11,15,35 This could account for canine complex carcinomas and carcinomas arising in benign mixed tumors having a more favorable prognosis.
Ductal carcinomas had a low tendency to invade lymphatics such that its biological behavior is not very different from its benign counterpart, the ductal adenoma (canine basaloid adenoma). 25,27 The specific histologic features of this tumor subtype are comparable with apocrine ductal carcinomas of dogs and cats. The nomenclature refers to highly specific histomorphology that is unrelated to the human breast ductal carcinoma.
Due to the small number of samples, the remaining tumor subtypes were not included in the statistical analysis, and further detailed investigations are needed to clarify their biological behavior. However, despite the small number of cases, invasive micropapillary carcinomas, adenosquamous carcinomas, and lipid rich carcinomas were often associated with LVI and RLM, as already reported. 4,16,30 Similarly, intraductal papillary carcinoma, the malignant counterpart of the intraductal papillary adenoma (duct papilloma), did invade the lymphatic system in some cases.
The presence of neoplastic emboli within the dermal lymphatic vessels, which was occasionally observed with some of the most aggressive CMCs, leads to blockage of the superficial dermal lymphatic drainage. The outcome is a clinical presentation that resembles an inflammatory process (inflammatory mammary cancer), which has a poor prognosis and a rapid, fatal clinical course, since all the available treatments are usually palliative. 6,8,24
We found that for CMCs, the presence of peripheral infiltration is a significant factor in predicting the likely risk of invasion of the lymphatic system. Therefore, when a diagnosis of mammary carcinoma is made, the tissue surrounding the tumor should be evaluated, and when areas of stromal desmoplastic reaction are found, a careful search for entrapped neoplastic cells should be undertaken. Furthermore, the presence of a micropapillary pattern, independent the tumor subtype, was significantly associated with invasion of the lymphatic system. This result was similar to that found in humans with carcinomas of the breast, stomach, lung, and gallbladder. 18,23,40,45 The aggressive behavior of the cells that produce micropapillae was attributed to their high proliferative activity, stimulation of angiogenesis, and anchorage-independent growth. 14,20 Vasculogenic mimicry was recently described in canine inflammatory mammary cancers and previously in several human malignant tumors, such as breast carcinomas, gliomas, melanomas, and hepatocellular carcinomas. 6,46 Human studies suggested that it furnishes an additional blood supply to the tumor and facilitates hematogenous dissemination. 12,37,46 In dogs this phenomenon was hypothesized to promote the lymphatic spread of tumor cells. 6 In the present study, we found vasculogenic mimicry almost exclusively in simple anaplastic carcinomas, which supports the theory that the formation of these channels is due to a lack of differentiation and marked plasticity of the tumor cells. 46 However, vasculogenic mimicry was not significantly associated with LVI and RLM.
Both histologic grading systems evaluated in this study were significant in being able to predict invasion of the lymphatic system. As expected, an increasing tendency to metastasize was identified from grade I to grade II to grade III tumors. However, the Clemente system had the lowest AIC values, indicating that it was a slightly better model for predicting the risk of LVI and RLM. The Misdorp system, when compared with the Clemente system, tended to underestimate malignancy, with more CMCs invading the lymphatic system classified as grade I or grade II tumors. In particular, the Misdorp system was not reliable when tumors were classified as grade I, because a considerable proportion (50%) of them showed LVI. A possible explanation of the higher predictive ability of the Clemente system is the more stringent and rigorous evaluation of the mitotic activity, which is performed in selected mitotically active parts of the tumor and consists of only counting mitoses without considering hyperchromatic nuclei.
In addition, when tumor subtype was evaluated in conjunction with peripheral infiltration by neoplastic cells, micropapillary pattern, and tumor grade using the Clemente system, these features added significance for predicting the likelihood of LVI and RLM.
In conclusion, this study confirms the significant prognostic role of a modified WHO classification of CMCs. In addition, there are other histopathologic parameters that are of prognostic importance that we suggest should be incorporated into the pathology reports of CMCs.
Footnotes
Acknowledgement
We thank Dr Lorenzo Marini, Department of Environmental Agronomy and Crop Production, University of Padova, Italy, for his advice.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.