
Abstract
The Flat Coated Retriever is a breed at risk of development of histiocytic sarcoma (HS), but in contrast to the disseminated form of disease recognized in the Bernese Mountain Dog, most reports of HS in Flat Coated Retrievers describe a localized lesion affecting the musculature or fascia of limbs. The purpose of this study was to review data and material received though an ongoing Flat Coated Retriever tumor survey to better define the presentation of HS in the breed and to determine the utility of subclassification of tumors arising at different sites by histology and immunohistologic phenotyping. Data on 180 dogs bearing HS-like tumors were available for review, which showed that although the majority (101 lesions, 57%) were primary limb lesions, 47 dogs (26%) had visceral, mainly splenic lesions with no peripheral primary tumor. A detailed histologic and immunohistologic review of 20 limb tumors and 20 splenic tumors showed that 2 distinct phenotypic subtypes could be identified: a histiocytic subtype, most prevalent in the splenic tumors, and a histiocytic–spindle–pleomorphic subtype, mainly seen in the limb tumors. Despite their variable morphology, all tumors expressed major histocompatibility complex class II and the leukocyte antigen CD18, but only those tumors in the spleen consistently expressed CD11d. The majority of tumors also contained a mild to moderate infiltrate of T lymphocytes.
In studies of causes of death in dogs in Sweden and Denmark, the Flat Coated Retriever has been reported to be in the top 5 breeds at risk of developing cancer. 4,23,24 A histopathologic survey of neoplasms in Flat Coated Retrievers in the United Kingdom was started in March 1990, with the support of owners and breeders. 8,25 Preliminary results showed the breed to be particularly prone to developing aggressive soft tissue sarcomas, accounting for 26% of all tumor samples and 44% of malignant tumors. 21 More recently in a cohort study involving 174 dogs followed over 10 years, 32 (18%) dogs died as a result of soft tissue sarcoma. 7 A tumor of similar histologic description has been reported to account for 36% of malignant tumors seen in Flat Coated Retrievers in a referral hospital population in Zurich. 11 Histologically, most of these tumors are poorly differentiated anaplastic round cell or spindle cell tumors, the histogenesis of which is difficult to determine on hematoxylin and eosin–stained (HE-stained) sections. Histiocytes are a heterogeneous group of cells with different morphologic and functional features.
Canine histiocytic disorders were first described in the late 1970s. 13 Several pathologies have been reported, including canine cutaneous histiocytoma, malignant fibrous histiocytoma (MFH), and histiocytic sarcoma (HS) complex. 13,15 –17,29 Cutaneous histiocytoma is a benign tumor; the majority occur in dogs younger than 4 years of age. 14 Cutaneous histiocytomas can be diagnosed by cytology, but histopathologic examination with immunohistochemical staining provides a definitive diagnosis. 13 MFH is a soft tissue sarcoma that may be confused with HS. 13 Recent immunostaining and molecular studies demonstrate that MFH describes a group of undifferentiated pleomorphic sarcomas. 13 The latest World Health Organization classification of tumors has removed MFH. 12
The term histiocytic sarcoma has been adopted to include a spectrum of malignant tumors of neoplastic histiocytes 2 that are immunopositive for the cell surface marker CD18. 5 The term localized histiocytic sarcoma has been proposed to and the multifocal, disseminated form of HS — previously, malignant histiocytosis. The latter is highly breed specific, especially in the Bernese Mountain Dog, where it has been reported with a frequency of 25%. 1 Malignant histiocytosis is also prevalent in Rottweilers and retrievers. In contrast to the multifocal, disseminated form of malignant histiocytosis reported in these breeds, most forms of HS or HS-like tumors reported in Flat Coated Retrievers have been solitary tumors arising in the deep musculature or fascia of limbs or in association with joints. 11,21 However, an aggressive form of HS of the spleen has been reported in Flat Coated Retrievers; 9 in these dogs, the clinical presentation and findings were consistent with a hemophagocytic form of HS described by Moore and colleagues. 20
Our hypothesis is that a visceral, predominantly splenic form of HS is also prevalent in the breed, which may have morphologic differences to the localized form of disease.
The purpose of this study was to review all cases of soft tissue sarcoma submitted to the ongoing Flat Coated Retriever Cancer Survey (FRCS) at the Department of Veterinary Medicine, University of Cambridge, from 1996 to 2009. We aimed to document the clinical presentation and behavior of histiocytic-like sarcoma in the breed and in a representative sample of tumors proposed to characterize the histologic features and antigen expression profiles of localized peripheral tumors, in comparison with those arising in viscera.
Materials and Methods
Patient Data
All data on tumors submitted to the FRCS is held on a FileMakerPro database. Flat Coated Retrievers with tumor samples receiving a diagnosis of “sarcoma” between January 1, 1999, and January 5, 2009, were identified using a database search for the term sarcoma.
The histology reports were examined for diagnosis consistent with anaplastic, poorly differentiated, pleomorphic round or spindle cell sarcoma. All non–soft tissue sarcoma (eg, osteosarcoma) and all differentiated sarcomas (eg, fibrosarcoma) were excluded from the study. Where the sample was reevaluated subsequent to the initial report, the most recent diagnosis was used. Histopathologic findings were not reviewed for all cases.
Data on cases meeting the above criteria were collected from the FRCS submission form, Queens Veterinary School Hospital records, and by telephone contact with the submitting veterinary practice. Information collected included age, sex, tumor location, clinical signs at presentation, evidence of metastasis at diagnosis and euthanasia (based on the judgment of the submitting veterinary surgeon), treatment, survival duration, and histologic diagnosis.
Histologic Classification
Paraffin blocks from 20 localized (limb) tumors and 20 visceral (splenic) tumors were randomly selected for histologic review and further phenotypic classification. The diagnosis of HS in these 40 tumors was indicated by the pathology reports and confirmed by histopathologic reevaluation of samples by one author (F.C.-C.), as well as positive immunostaining for major histocompatibility complex (MHC) class II and CD18. Sections stained with HE were reviewed to assess the distribution, pattern, and cellular morphology of neoplastic cells. Further sections were taken from the paraffin blocks for immunohistochemistry staining. Diagnosis included immunohistochemical evaluation, using the classification scheme defined by Affolter and Moore. 2
Following review of the HE-stained sections of localized and splenic HS, a range of cellular morphologies were identified, including histiocytic cells, spindle-pleomorphic cells, multinucleate histiocytic giant cells, erythrophagocytic cells, and inflammatory cells. For each tumor, the proportion of cell types was estimated in 20 random fields at 20× magnification where neoplastic tissue was present (necrotic and hemorrhagic areas were excluded from the estimation).
HSs were then grouped according to histiocytic subtype (when > 50% of neoplastic cells were histiocytic cells) and histiocytic–spindle–pleomorphic type (when ≤ 50% of neoplastic cells exhibited features of histiocytic cells and the majority of remaining cells exhibited fibroblastic-like features). Estimation of other cell types was recorded but taken into account as only a description for each tumor, given that none of them represented more than 10% in each case with HE staining.
For immunohistochemistry, serial sections of 3 μm were cut from the appropriate blocks and mounted on positively charged slides (Snowcoat, Surgipath Europe Ltd, Peterborough, UK). An automated immunohistochemistry system (Dako Autostainer, Dako, Carpinteria, CA) was used to process the deparaffinized tissues. Endogenous peroxidase activity was inhibited using Dako REAL peroxidase-blocking solution. The immunohistochemical antibodies were MHC class II (HLA-DR, mouse anti-human monoclonal, 1:400, Dako), CD11d (1:500, School of Veterinary Medicine, University of California, Davis, CA), CD18 (1:25, School of Veterinary Medicine, University of California), CD3 (mouse anti-human monoclonal, 1:150, Dako) and CD79a (mouse anti-human monoclonal, 1:400, Dako). Peroxidase activity was demonstrated using diaminobenzidine solution for 10 minutes, and slides were counterstained with Gill’s hematoxylin for 2 minutes before rinsing, dehydrating, clearing, and mounting with coverslips.
Positive control tissues included reactive lymph node or spleen, although many of the tumor sections also acted as internal positive and negative controls for the antibodies. Antibody diluent (Dako) was used in place of the primary antibody to act as a negative control in each immunostaining procedure. For all antibodies, immunopositivity was present in the positive control sections but not detected in the negative controls.
Immunostaining for tumors was considered in 2 categories: negative and positive. Out of the latter 20 random fields of neoplastic tissue at 20× magnification, tumors were further categorized into 3 groups: more than 30% but less than 60% of cells stained, 60 to 90% of cells stained, and more than 90% of cells stained. Immunostaining for infiltrates of T lymphocyte and B lymphocyte was considered and categorized in the same manner as the neoplastic cells.
Statistical Analyses
Survival was estimated using Kaplan–Meier cumulative survival plots. Dogs were censored only for survival beyond the censor date of January 5, 2009, because the tumor could not be reliably ruled out as a contributing factor to death in the cases with survival data available. Fisher exact test (2-tailed) was used for comparison of morphologic and CD11d expression between tumors located in the limb and spleen.
Results
Tumor Location and Presentation
In sum, 180 dogs met the criteria for inclusion in the study: 91 female and 89 male. The mean age at diagnosis was 8.3 ± 3.96 years (range, 0.75 to 13.00; n = 178).
Lesion location was known in 178 dogs: 101 dogs (56.7%) had limb lesions, 47 (26.4%) had visceral lesions, and 30 (16.9%) had lesions at other sites (Table 1 ). There was no significant sex predilection in the sample overall nor any significant difference in the mean age based on sex or tumor location.
Data From Flat Coated Retriever Cancer Survey Database: Site and Signalment of Anaplastic, Histiocytic-Like Sarcomas a
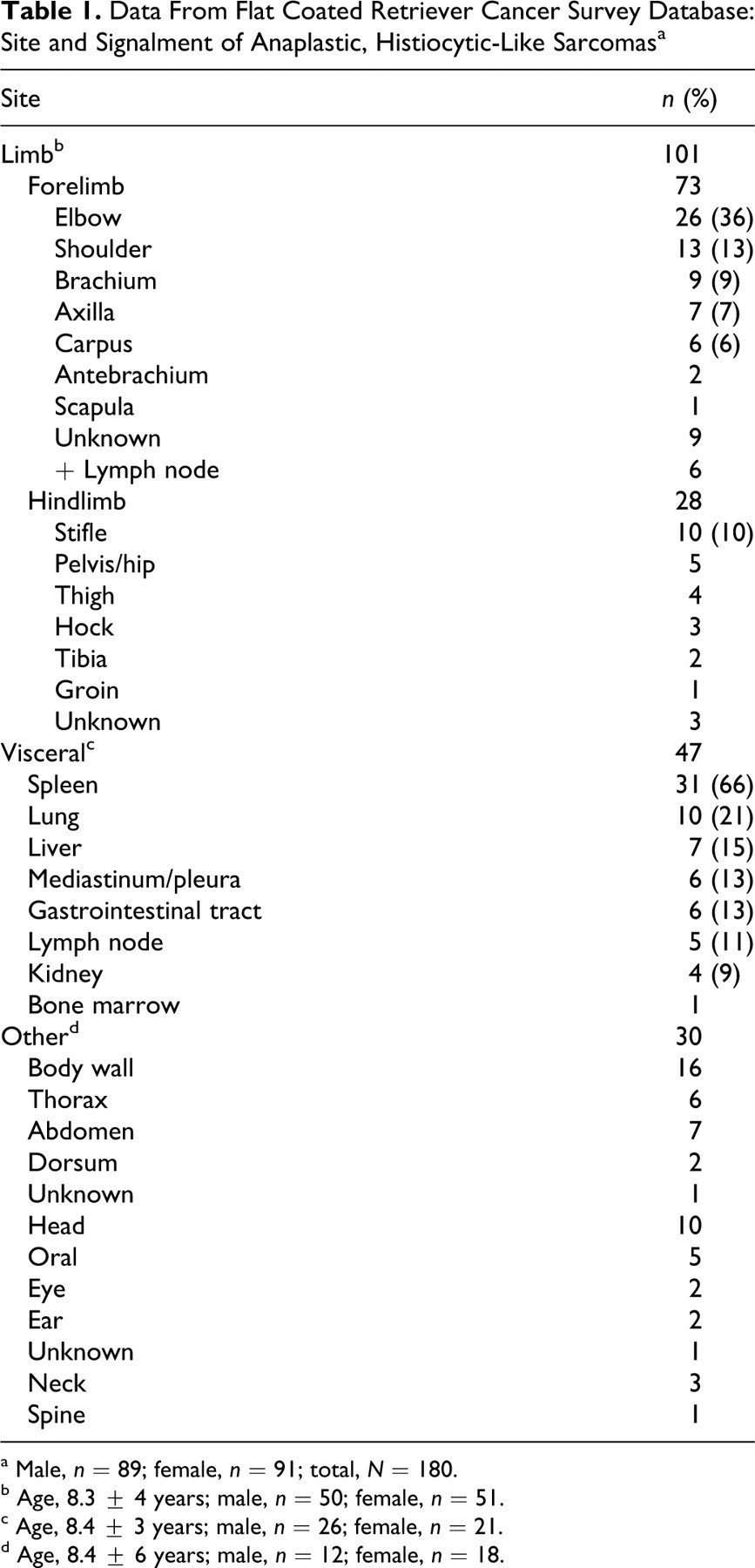
a Male, n = 89; female, n = 91; total, N = 180.
b Age, 8.3 ± 4 years; male, n = 50; female, n = 51.
c Age, 8.4 ± 3 years; male, n = 26; female, n = 21.
d Age, 8.4 ± 6 years; male, n = 12; female, n = 18.
Of the 101 limb tumors, 73 occurred in the forelimb, and 28 were hindlimb lesions. In the forelimb, 26 lesions (35.6%) occurred in the elbow region, and 30 (41.1%) were proximal to the elbow. In the hindlimb, 24 lesions (82.8%) were in the stifle region or more proximally. In total, 59 (58%) limb lesions were periarticular in site, although involvement of the joint was not specified on the submission forms. Of the 47 visceral lesions, 31 (66%) involved the spleen, and 10 (20%) were reported at multiple visceral sites at diagnosis. The majority of the other lesions involved the subcutaneous or muscle tissue of the body wall.
Presenting signs varied with tumor location. For lesions affecting the limbs, the most common reported sign was the presence of a mass with lameness at or preceding presentation by weeks to months. Local lymphadenopathy was detected at presentation in 6 cases (6%). The most common signs and clinical findings for visceral lesions were as follows: an abdominal mass (n = 15, 32%), inappetence (n = 10, 21%), weight loss (n = 6, 13%), lethargy (n = 13, 28%), pale mucous membranes (n = 8, 17%), and respiratory signs (n = 6, 13%). At other sites, the presence of a mass was a presenting sign in the majority of dogs (n = 28, 93%).
Survival Times
Twenty-nine dogs were euthanized at the time of diagnosis, and 5 others were euthanized within 7 days of diagnosis. Twenty-eight dogs received no treatment or symptomatic treatment with prednisolone. Fifty dogs were treated surgically. For limb lesions, this included amputation (n = 11), wide surgical excision (n = 6), and surgical debulking (n = 6). For visceral lesions, surgery included splenectomy (n = 11), enterectomy (n = 1), and lung lobectomy (n = 1). For other sites, all 7 surgeries were mass removal. Seven dogs received multiple treatments: 1 dog had radiotherapy and chemotherapy; 1, surgery and chemotherapy; 2, surgery and radiotherapy; and 3, surgery, radiotherapy, and chemotherapy. Lomustine (CCNU) was the most commonly used chemotherapeutic drug (4 cases).
For those dogs that survived more than 7 days from diagnosis, the overall median survival time was 95.0 ±57.8 days. Tumor location significantly affected survival; median survival for limb tumors was 140 ± 24.4 days, in comparison to visceral tumors, 29 ± 14.6 days, and tumors at other sites, 228 ± 184 days (all SDs based on 95% confidence interval; Fig. 1 ).
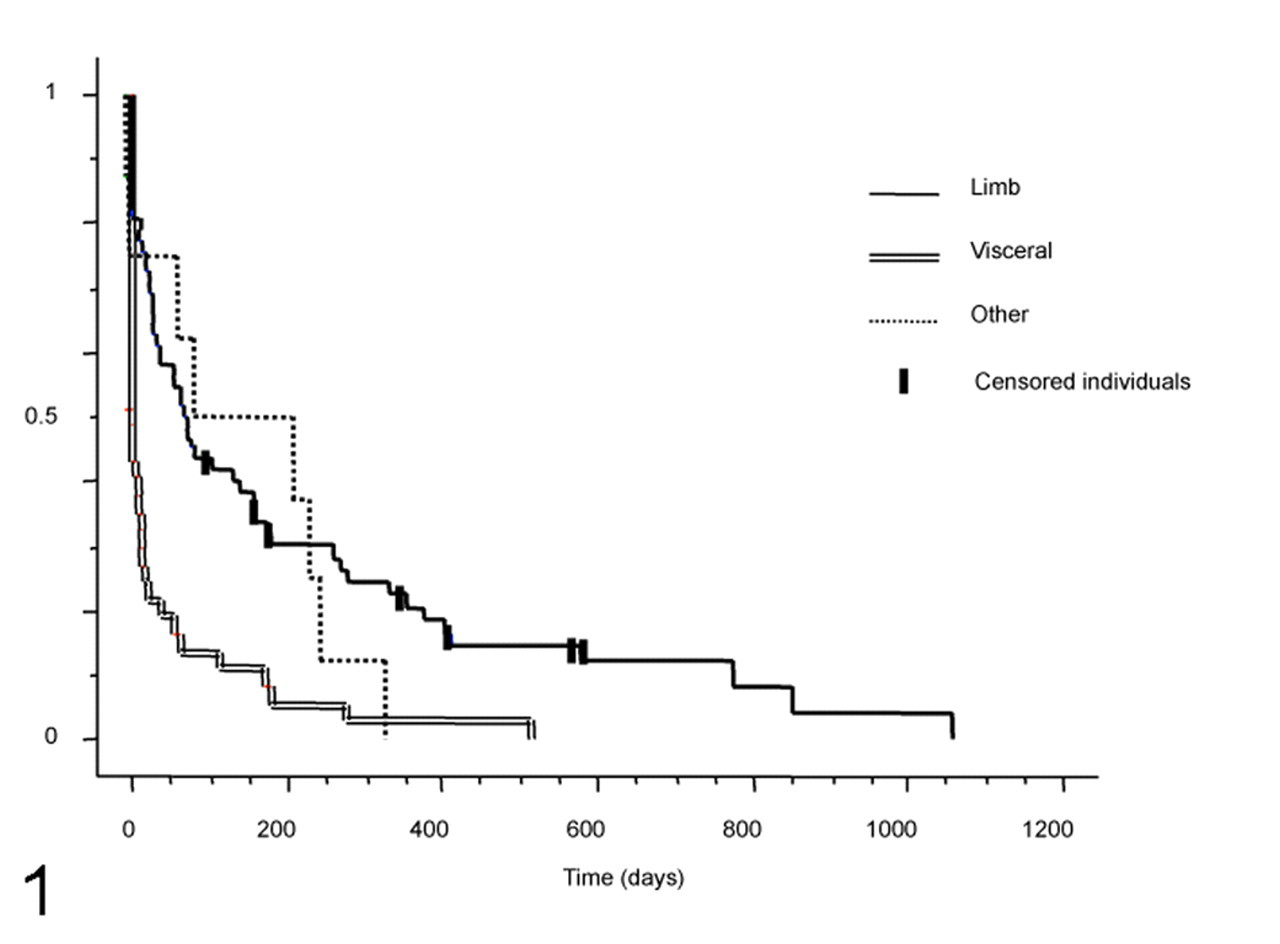
Kaplan–Meier cumulative survival plot for limb, visceral, and other tumor locations for dogs surviving more than 7 days.
Metastasis at the time of euthanasia was reported in 64 cases, including 28 of 101 limb tumors (27.7%), 31 of 47 visceral tumors (66.0%), and 5 tumors at other locations (16.7%). Information on the presence or absence of metastases for the other 116 cases is unknown.
Histologic Classification and Immunohistochemistry
Histopathologic evaluation revealed neoplastic tissue in moderately to poorly demarcated masses in the localized HS involving the skin and subcutis of the extremities and in the splenic HS. The neoplastic lesions were composed of dense sheets of variable numbers of histiocytic cell type, mixed with spindle-shaped pleomorphic cells and variable numbers of multinucleated histiocytic giant cells, erythrophagocytic cells, and inflammatory cells. Erythrophagocytosis was more evident in the splenic tumors than in the limb lesions (data not shown).
Cells within the tumors were described as follows: Histiocytic cells were large round neoplastic cells with indistinct borders and moderate to abundant pale eosinophilic cytoplasm, with occasional cytoplasmic vacuoles or foamy cytoplasm. Nuclei varied in size and were round to oval and frequently indented or vesicular; nucleoli were single or several and prominent. Chromatin was finely stippled or coarse. Spindle-shaped to pleomorphic cells were fibroblast-like cells with cytoplasmic processes and elongated to oval nucleus with stippled chromatin. Histiocytic neoplastic cells were associated with variable numbers of plump mesenchymal cells in different amounts but were more numerous in the localized HS. Neoplastic multinucleated histiocytic giant cells were large round cells or bizarre stellate cells with multiple nuclei. Erythrophagocytic cells contained erythrocytes and hemosiderin deposits that were positive with Perl’s staining. Clusters of inflammatory cell infiltrates varied among sections and ranged from mild infiltrates to a prominent reactive infiltrate. Inflammatory infiltrates consisted of small lymphocytes, plasma cells, neutrophils, and occasional eosinophils.
HSs were diagnosed according to our criteria as histiocytic subtype and histiocytic–spindle–pleomorphic subtype. A marked anisokaryosis and anisocytosis were present in both forms of HSs, with a average mitotic rate of 15 per 10 high-powered fields. The different histologic HS subtypes diagnosed are listed by site in Table 2
and illustrated in Figures 2 and 3
.
Number of Histiocytic Sarcoma Phenotypes Diagnosed in the Localized Subcutaneous and Splenic Forms of Flat Coated Retrievers a
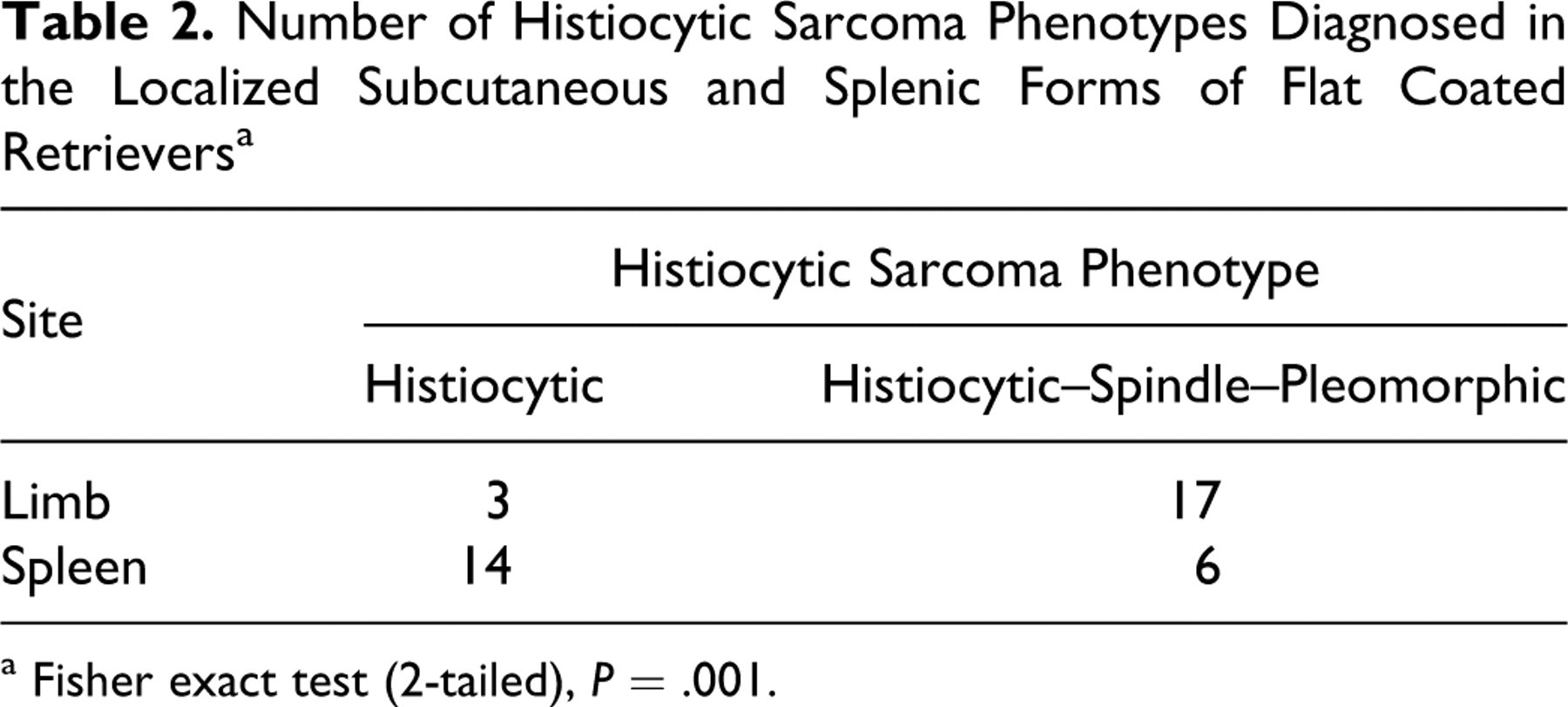
a Fisher exact test (2-tailed), P = .001.
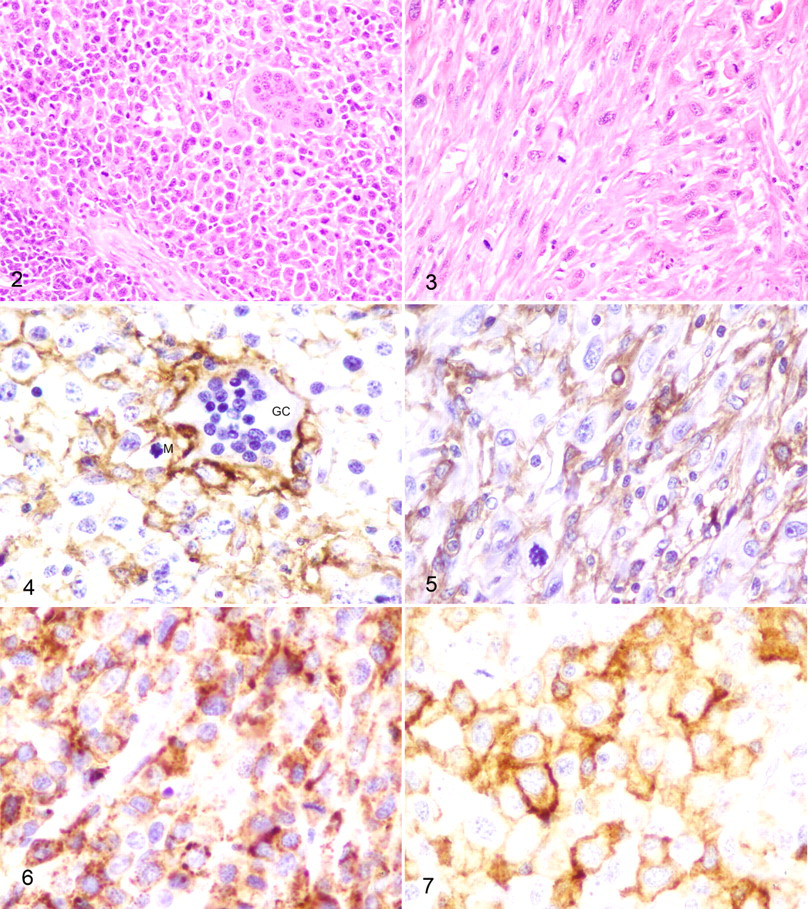
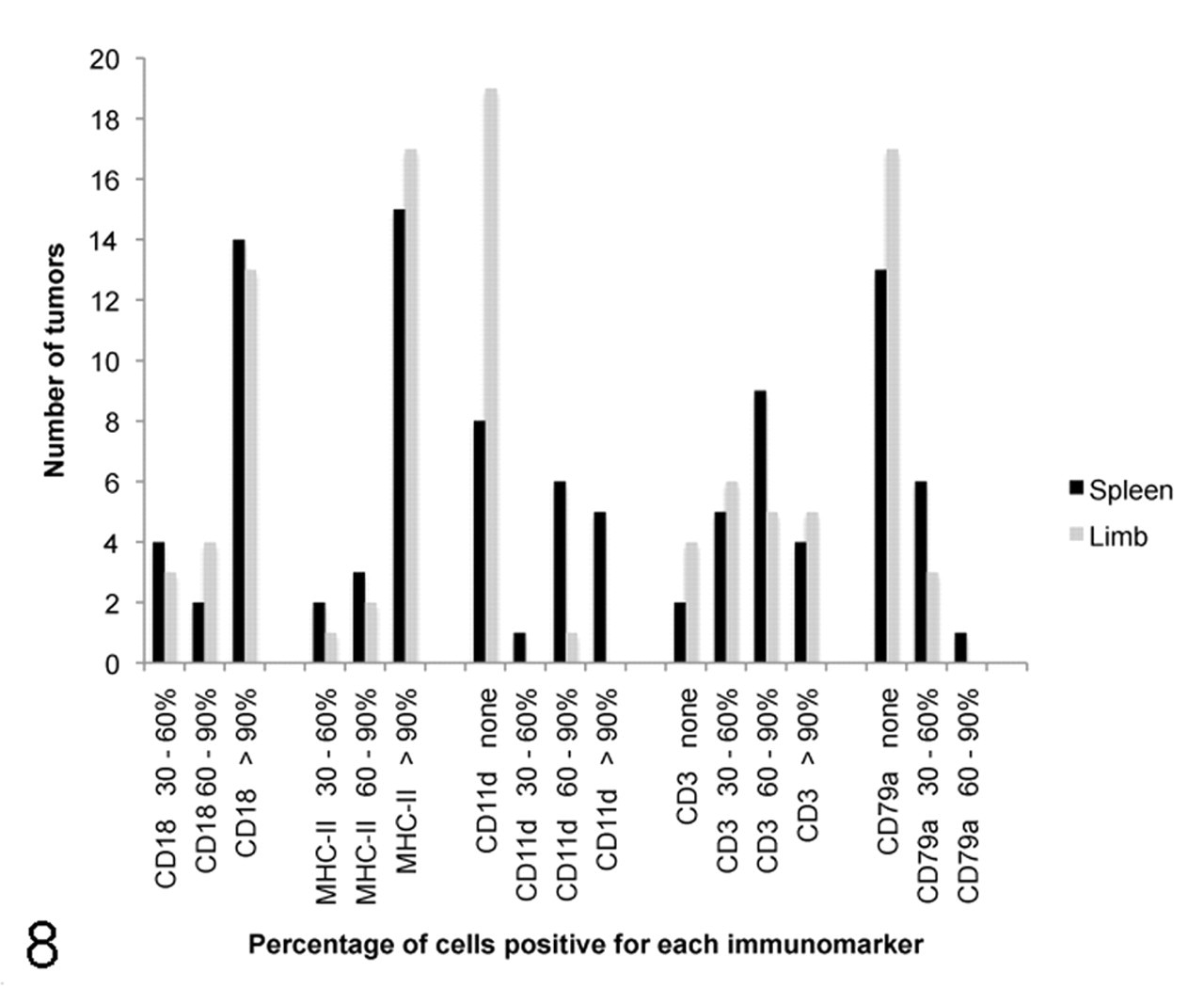
Results of immunostaining for CD18, major histocompatibility complex class II, CD11d, CD3, and CD79a of histiocytic sarcoma in the spleen and limb of Flat Coated Retrievers.
The immunostaining results for both location and HS types are illustrated in Figures 4–7, and the data are given in Figures 8 and 9. Despite their variable morphology, all 40 tumors in this study, whether localized subcutaneous or splenic, consistently expressed MHC II and showed a consistent phenotype with expression of the leukocyte antigen CD18. Immunohistochemistry for CD18 staining was diffusely positive throughout the tumors. A mild to moderate nonneoplastic cell infiltrate expressed either CD3 or CD79a. The number of lymphocytes varied among different tissue samples. The lymphocytic infiltrate was shown to consist predominantly of T lymphocytes.
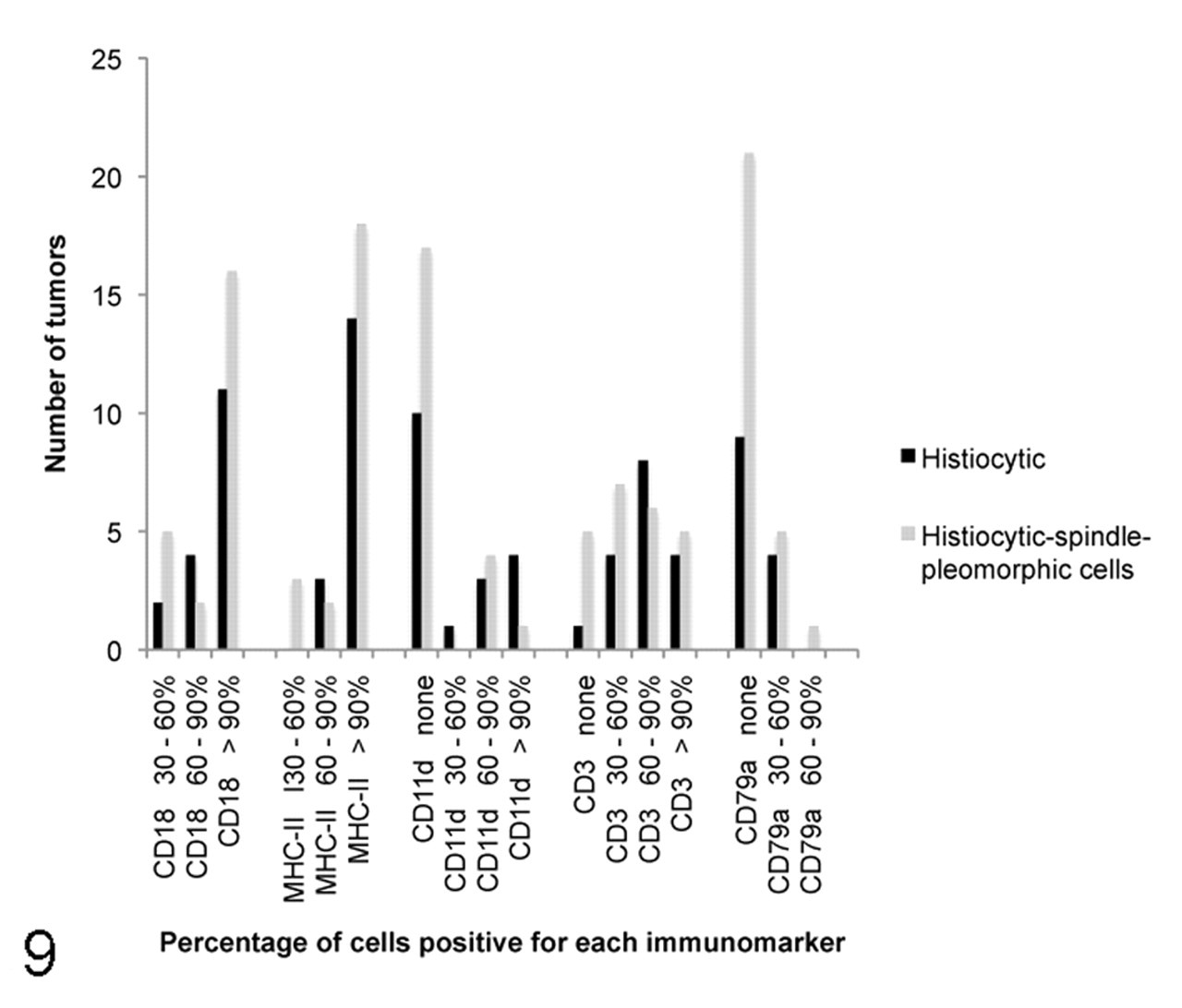
Results of immunostaining for CD18, major histocompatibility complex class II, CD11d, CD3, and CD79a of histiocytic sarcoma phenotypes in the splenic and limb forms of Flat Coated Retrievers.
Discussion
Histiocytic proliferative disorders are prevalent in dogs and comprise a variety of clinical and pathologic presentations with recognized breed predilections. Dendritic cells (DCs) of either Langerhans cell or epithelial and interstitial DC lineage are the proliferating cells in all these diseases. HSs are among the malignant variants of these tumors in dogs, 2 where classification is either into solitary HS (where the primary tumor is localized in one organ with or without metastasis to draining lymph nodes) or disseminated HS (which involves several organs in an apparently multicentric presentation). 2,9
We have reported the Flat Coated Retriever to be at risk of development of HS-like tumors, but these have been predominantly localized lesions with a moderately high metastatic rate. The 180 HS-like tumors identified in the FRCS database represent approximately 30% of all malignant tumors submitted to the survey in the 10-year period. The mean age at presentation of 8.3 years was consistent with previous reports, 11,21,22,28 and no sex predilection was noted. As previously documented, 2,10,19 tumors were most commonly found in the soft tissues and muscle of the limbs, with a strong predilection for the proximal forelimb—particularly, the elbow area. However, the main finding of this study was that a significant number of dogs (n = 47, 28% of total) were affected by a visceral form of the disease, where lesions were often multifocal or disseminated. These dogs presented with vague systemic signs, including anorexia, lethargy, and weight loss, and a palpable abdominal mass was reported in 11 cases. None of these dogs had a primary peripheral soft tissue mass, suggesting that the splenic/visceral lesions were primary as opposed to metastatic. Previous reports have suggested that in Flat Coated Retrievers and Golden Retrievers, HS is generally localized, which is in contrast to Bernese Mountain Dogs and Rottweilers, where HS is invariably disseminated. 2,11 The present study shows that this is not the case and that although HS is most commonly associated with a limb mass in the Flat Coated Retriever, a visceral or disseminated form of the disease is recognized in the breed.
The subcategories of localized and disseminated have been applied to HS to distinguish between those tumors that present as solitary masses and those that are multifocal or disseminated from the outset. The differentiation between localized and disseminated HS might be important prognostically because a truly localized HS carries a more favorable prognosis. 27 However, in Flat Coated Retrievers, HS is an aggressive, malignant tumor with a high rate of metastasis 11 such that those “localized” tumors that present as solitary masses can rapidly disseminate to involve other organs. Based on an examination of the data provided by the FRCS, the 2 main presentations documented are different manifestations of HS that might better be described as soft tissue and visceral rather than localized and disseminated.
HSs have a range of histologic appearances 21 such that the diagnosis of HS can be microscopically complex and the nomenclature, confusing. 9 Histologic findings in HS include diffuse proliferation of neoplastic histiocytes, multinucleated histiocytic giant cells, spindle cells, anaplastic cells, and in some cases, the presence of erythrophagocytic cells. 3,18,19 Lymphocytic infiltrates in HS have also been mentioned. 21 In our study, histopathologic examination revealed that HSs contain a heterogeneous population of cells, including the histiocytic–spindle–pleomorphic cells, multinucleated histiocytic giant cells, erythrophagocytes, and lymphocytes. We were able to identify 2 distinct histologic subtypes—namely, histiocytic and histiocytic–spindle–pleomorphic. To date, HS has largely been reported as a single tumor entity, and further classification into subtypes—as in other tumors or by applying a grading system of malignancy (as in soft tissue sarcoma)—has not been described. This study has shown that HS tumors can be subclassified on the basis of cellular morphology (or phenotype) and expression of cell surface antigens; that this correlates with tumor location may ultimately prove useful in predicting biological behavior and prognosis.
In our study, the histiocytic–spindle–pleomorphic subtype was significantly more common in the localized soft tissue form than in the splenic form, with the latter being the predominantly histiocytic subtype, as is consistent with previously described HS of the spleen. 9 This observation could be related to the tissue microenvironment being different from the splenic parenchymatous microenvironment. Collagen and fibroblasts are more numerous in the dermis than in the spleen, which could account for the high proportion of spindle cell type in HS at this site. Alternatively, an interaction with neoplastic histiocytic cells could induce dermal spindle cell proliferation within the tumor. Azakami and colleagues 3 described a monomorphic cell type in canine HS in culture that appeared to originate from cells of the mononuclear phagocytic system, which is in contrast to the variable cellular morphology observed in our tumors. Phagocytosis is a feature of macrophages, and in our study, some cases had mild to moderate erythrophagocytosis, as described in the hemophagocytic variant of HS in the spleen. 19,20
Immunohistochemical staining is an increasingly important technique to accurately identify the cell of origin in poorly differentiated tumors such as HS. 2,13,28 Identification of histiocytes can be achieved with molecules involved in antigen presentation, such as MHC II molecules and the β2 integrins CD11d/CD18. 20 In normal spleen, the β2 integrin expression by histiocytes is highly ordered. 20 CD11d is exclusively expressed by red pulp macrophages beyond the marginal zone, 20 whereas in neoplastic conditions, CD11d expression becomes disordered, as found in the Flat Coated Retrievers of this study. On the basis of immunohistochemistry, HS is CD18+. 2 CD18 is the common subunit of β2 adhesion integrins and is expressed in histiocytes, DCs, lymphocytes, and polymorphonuclear leukocytes. 6 It is also known that integrin αDβ2 (CD11d/CD18) upregulation on differentiated macrophages may facilitate their retention at sites of inflammation. 30 In our study, cellular morphology and immunostaining with CD18+, MHC II, CD3–, and CD79a– phenotype were the criteria for diagnosis of HS. 2 Neoplastic histiocytes in the localized and splenic form dominantly expressed the leukocyte integrins CD18 and MHC II. But only those in the spleen expressed CD11d.
CD11d is a marker of red pulp macrophages. 26 Localized subcutaneous HSs were consistently CD11d–, whereas 60% of splenic HS expressed CD11d+. The latter suggests that these tumors arise from splenic red pulp and bone marrow macrophages, which express the β2 integrin CD11d. 20 In our study, we were able to quantify the level of expression of CD11d in immunopositive cells from 30% to more than 90%. No previous reports in the literature have documented an estimation of the percentage of immunopositive cells, so it is not certain (1) whether normal CD11d+ red pulp macrophages could interact with CD18+ neoplastic cells and be stimulated to proliferate as part of the HS complex to give this result or (2) whether these splenic HS tumors truly originate from splenic red pulp macrophages and represent the hemophagocytic variant of canine HS as previously described. 20 However, one would need to demonstrate a Coombs-negative regenerative anemia, ideally combined with results of bone marrow examination, to confirm this. Such data were not available for the dogs in our study. In contrast to the splenic tumors, the localized subcutaneous limb tumors lacked expression of CD11d, which supported their origin from interstitial DCs. 2
Lymphoid biomarkers were included in this study to rule out lymphoma, but immunostaining for lymphocytes demonstrated the presence of a lymphoid infiltrate in many tumors; furthermore, the majority of lymphocytes present in localized subcutaneous and splenic HS expressed CD3, consistent with T lymphocytes, which suggests a cell-mediated immune response. This finding corresponds with previous reports where tumors have an inflammatory infiltrate shown to consist predominantly of T lymphocytes. 20 Lymphocytes might play an important role in tumor growth, immunotherapy, and tumor regression. The proportion of CD79a and CD3 immunopositive cells has been reported in MFH from Flat Coated Retrievers. 22 A higher proportion of CD3+ cells was found, confirming that most tumors had a mild or moderate lymphoid infiltrate mainly consisting of T lymphocytes, whereas B lymphocytes were absent or in lower numbers.
We have not attempted to correlate any of the histologic or immunohistochemical findings with survival or prognosis, because few dogs included in the 40 reviewed tumors received treatment. Indeed, 5 dogs with localized tumors and 16 with splenic/visceral lesions were euthanized at the time of tumor diagnosis (the latter often during exploratory celiotomy), making the number of dogs with any survival data too few to subject to any statistical analysis.
To our knowledge, this is the first study where the proportion of histiocytic neoplastic cells, spindle neoplastic cells, and T lymphocytes and B lymphocytes has been reported to diagnose and subclassify HS. In this study, the localized subcutaneous form of HS showed predominantly histiocytic–spindle–pleomorphic morphology and was consistently CD11d–, with one exception, whereas the splenic form showed predominantly histiocytic morphology and had 60% CD11d+ expression, indicating that CD11d could be used as an aid in diagnosis of both forms and possibly as biologically behavior-predictive factor. HS may encompass proliferation of other cell types, including lymphocytes. Histopathologic and immunophenotypic evaluation of involved organs are required for a definitive diagnosis of HS and to further characterize tumors into subtypes. Future studies will focus on further classification of these tumors using molecular techniques.
Footnotes
Acknowledgements
We are grateful to the breeders and owners of Flat Coated Retrievers who contributed information and samples. We thank the numerous clinicians and pathologists who contributed case material for this report. We would also thank Madeline Fordham, Helen Skelton, and Rayna Skoyles for technical assistance in conventional and immunohistochemistry preparation of tissue sections.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.