
Abstract
This article reports the case of a male patient in his 70s with middle aortic syndrome (MAS). The patient was admitted with abdominal pain, abdominal distension, vomiting, and cessation of defecation for 2 days as chief complaints and was diagnosed with intestinal obstruction. Enhanced computed tomography and vascular reconstruction revealed distal occlusion of the abdominal aorta. The celiac trunk, superior mesenteric artery, and inferior mesenteric artery were not visualized, whereas bilateral renal arteries maintained blood flow. Given the patient’s history of intermittent claudication and uncontrolled hypertension, the condition was ultimately diagnosed as MAS secondary to Takayasu’s arteritis, with bowel obstruction identified as a secondary manifestation of MAS. After insertion of a nasointestinal obstruction catheter, the patient’s symptoms of intestinal obstruction were relieved. However, the obstruction recurred, and the patient subsequently improved following vascular reconstruction. During postoperative follow-up to date, intestinal obstruction has recurred only once due to improper diet and resolved after dietary modifications. MAS is relatively rare in clinical practice, particularly among older patients. We hope that this case study provides clinicians with an opportunity for learning and knowledge exchange, thereby contributing to improved diagnostic and therapeutic approaches for patients with similar conditions.
Keywords
Introduction
Middle aortic syndrome (MAS) is a rare vascular condition characterized by segmental stenosis or occlusion of the distal thoracic and abdominal aorta as well as the ostia of the primary branches of the proximal abdominal aorta. 1 In most cases, the etiology of MAS remains unclear, and its clinical incidence is exceedingly low. MAS predominantly affects the visceral, renal, and lower limb arteries, which can lead to ischemia of the viscera and lower limbs, resulting in clinical manifestations such as severe renovascular hypertension, intermittent claudication, and abdominal colic. The formation of robust intestinal collateral circulation, particularly the arc of Riolan, can enhance visceral blood supply and reduce the likelihood of abdominal pain in patients with MAS. 2 In this case report, we described an adult male patient with MAS whose primary clinical manifestation was recurrent intestinal obstruction, accompanied by uncontrolled hypertension and intermittent claudication of both lower limbs. The diagnosis was primarily established using enhanced computed tomography (CT) and vascular reconstruction. Symptoms of intestinal obstruction were successfully alleviated via the placement of a nasointestinal obstruction catheter. Subsequently, with the assistance of vascular surgeons, the patient underwent an axillofemoral bypass using a prosthetic graft, which successfully restored blood supply to the intestines and lower limbs. Concurrently, with health education, the patient adopted dietary modifications, and no further episodes of intestinal obstruction have occurred to date. To the best of our knowledge, the vascular occlusion pattern observed in this case is relatively uncommon. We hope that this case report provides valuable insights for the diagnosis and management similar conditions.
Case presentation
The patient and his family provided written informed consent for publication, agreeing to the disclosure of clinical data, imaging data, and additional medical information. We have deidentified all patient details. The reporting of this study conforms to Case Report (CARE) guidelines. 3
In August 2024, a man in his 70s was admitted to our hospital (The Second Affiliated Hospital of Dalian Medical University) with a 2-day history of abdominal pain, bloating, and cessation of bowel movements, accompanied by nausea and vomiting. He reported no recent history of fever or significant weight loss. His medical history included hypertension (160/95 mmHg) and intermittent claudication. He had no history of smoking. As this was his first hospitalization, he had not previously undergone systematic examinations; therefore, a history of Takayasu arteritis (TA) remained unclear. Physical examination revealed visible abdominal distension and intestinal patterns, with scattered mild tenderness across the abdomen, no rebound tenderness or muscle guarding, and hyperactive bowel sounds at a frequency of six times per minute. Laboratory blood tests did not reveal any remarkable abnormalities. Abdominal CT scans initially showed significant dilation of the small intestine and widening of the abdominal aorta.
After admission, the patient received symptomatic treatments, including gastrointestinal decompression, anti-inflammatory fluid replacement, and enema. Enhanced CT demonstrated segmental stenosis of the abdominal aorta; occlusion of the abdominal trunk, superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and bilateral iliac vessels; and the formation of intra-abdominal collateral circulation and collateral vessels in the abdominal wall and retroperitoneum (Figures 1 to 3). Based on the patient’s medical history, clinical presentation, and imaging findings, the final diagnosis was MAS secondary to TA.

Vascular reconstruction. The proximal segment of the abdominal aorta shows robust blood flow and is well-developed, with adequate perfusion to the bilateral renal arteries. The distal abdominal aorta is absent, and the celiac trunk, superior mesenteric artery, inferior mesenteric artery, and iliac vessels are not visualized. The distal abdominal aorta is supplied by an extensive collateral circulation network. Green arrow indicates abdominal aorta; white arrow indicates renal artery; red arrow indicates collateral circulation.

Cross-sectional image of enhanced CT. The bilateral renal arteries maintain a satisfactory blood supply. The distal abdominal aorta is occluded, and an extensive collateral circulation network is evident within the abdominal cavity, abdominal wall, and retroperitoneum. This collateral circulation compensates for the blood supply to the bilateral iliac vessels. Red arrow indicates renal artery; green arrow indicates iliac vessels; orange arrow indicates common iliac artery; blue arrow indicates collateral circulation. CT: computed tomography.

Coronal image of enhanced CT. Red arrow indicates distal occluded abdominal aorta; yellow arrow indicates proximal abdominal aorta; green arrow indicates bilateral renal arteries; orange arrow indicates bilateral iliac vessels; blue arrow indicates collateral circulation network. CT: computed tomography.
On the third day of hospitalization, after the patient and family members provided written informed consent for treatment, a nasointestinal obstruction catheter was placed and meglumine diatrizoate was administered. Subsequently, the patient’s symptoms of intestinal obstruction improved markedly, with relief of abdominal pain and the resumption of defecation. Consultation from the vascular surgery department was obtained regarding treatment options. However, given the high technical difficulty, significant risks, and prolonged ischemia associated with revascularization surgery, which could potentially exacerbate the condition through reperfusion injury, surgical intervention was not pursued after discussion with the family. A follow-up abdominal CT confirmed the disappearance of the gas–liquid level in the intestinal tract and passage of meglumine diatrizoate to the anus. The patient was discharged without discomfort after removal of the drainage tube and resumption of a normal diet.
Unfortunately, the patient was repeatedly hospitalized for intestinal obstruction over a 4-month period due to underlying intestinal hypoperfusion. Although conservative management provided symptomatic improvement each time, his nutritional status progressively deteriorated, with a total weight loss of approximately 15 kg and a minimum body mass index (BMI) of 14.2 kg/m2. By the end of 2024, after obtaining written informed consent for treatment from the patient and his family, percutaneous mesenteric artery balloon angioplasty was attempted in the vascular surgery department to improve intestinal blood supply; however, the procedure was unsuccessful. Following expert consultation, the patient underwent an axillofemoral bypass using a prosthetic graft, which was performed successfully. Postoperatively, the patient was prescribed rivaroxaban (10 mg, qd) for anticoagulation and atorvastatin (10 mg, qd) for lipid management.
Thereafter, blood supply to the intestines and lower extremities gradually improved, with a marked reduction in episodes of intestinal obstruction and intermittent claudication. During follow-up, the patient experienced only one recurrence of intestinal obstruction in March 2025, which was attributed to improper dietary intake. After dietary modifications, including adoption of a liquid and soft diet, enteral nutritional supplementation (Fresubin), and small and frequent meals, no further episodes occurred. The patient achieved a bowel movement frequency of once every 2 days, and BMI recovered to 19.6 kg/m2. A follow-up examination in August 2025 revealed a reduction in collateral circulation in the abdominal cavity and left lower extremity, absorption of the obstruction site, and restoration of the previously twisted mesentery (Figure 4). The patient’s bypass vessels maintained good patency, and no complications such as bleeding were observed.
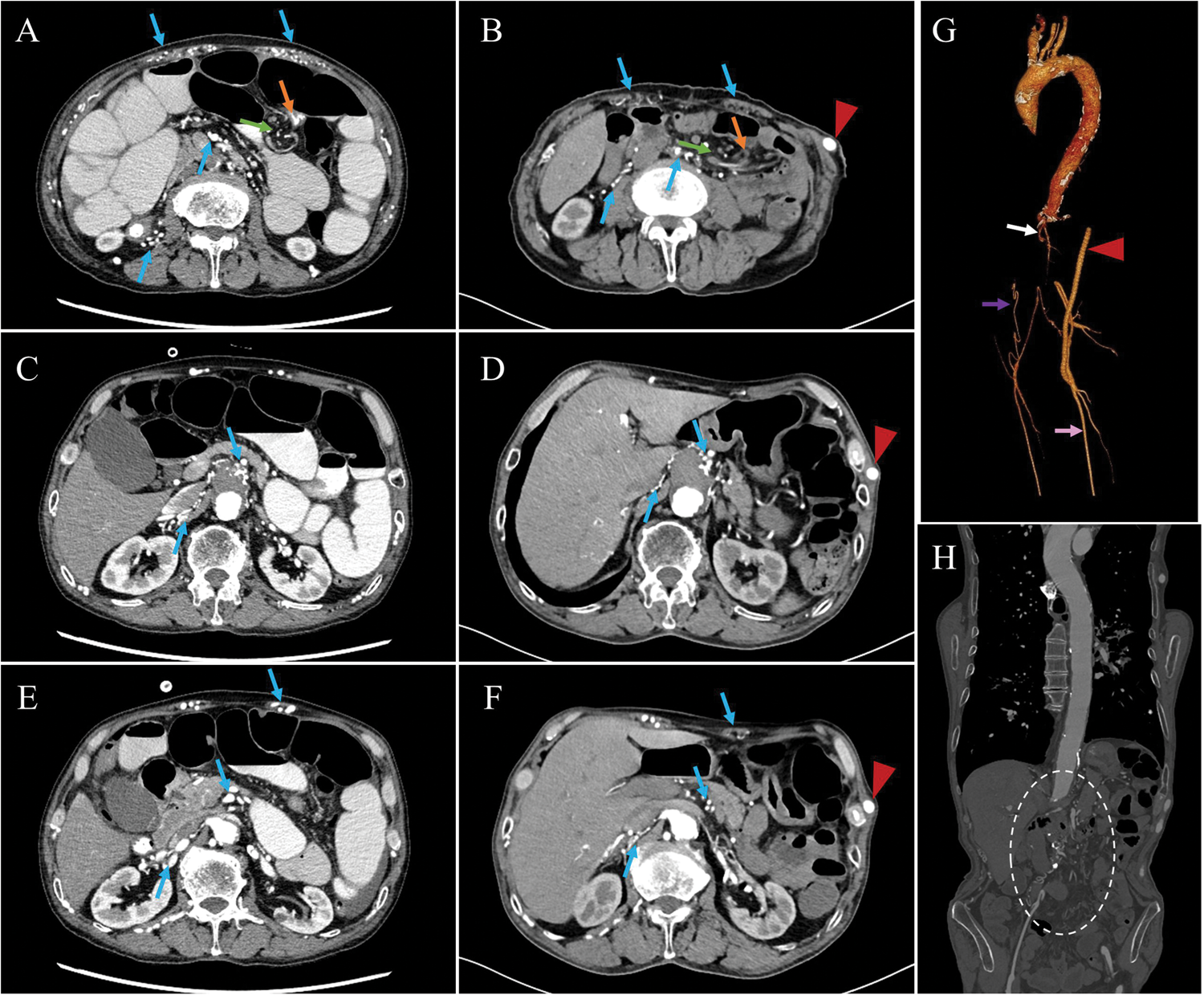
Comparison of CTA findings before and after revascularization. Collateral circulation in the abdomen and left lower limb is reduced, with improvement of intestinal adhesions and mesenteric torsion. The bypass grafts are patent, and the previously occluded abdominal vessels did not recanalize. (a, c, e) CTA results from August 2024; (b, d, f) CTA results from August 2025; (g) three-dimensional CTA vascular reconstruction from August 2025; (h) coronal view of the entire aorta on CT from August 2025. Blue arrows indicate collateral circulation in the abdominal wall and retroperitoneum; orange arrows indicate sites of intestinal adhesions; green arrows indicate torsion of the mesentery; white arrows indicate bilateral renal arteries; purple arrows indicate collateral circulation of the lower limb arteries with poor blood supply; pink arrows indicate lower limb vasculature after restoration of blood flow; red arrows indicate partial bypass graft; white dashed oval indicates occluded celiac artery. CT: computed tomography; CTA: computed tomography angiography.
Discussion
MAS predominantly occurs in children and young adults, and its etiology and pathogenesis remain unclear. It is currently believed to result from genetic and acquired factors. Genetic causes include conditions such as neurofibromatosis type 1 and tuberous sclerosis, whereas acquired factors can be classified as inflammatory (e.g. TA) or noninflammatory (e.g. postsurgical fibrosis and radiotherapy). 4 Prior studies have indicated that TA and atherosclerosis are the predominant causes of MAS in adults. 5 In our case, multiple arterial stenoses demonstrated on imaging suggest that the patient most likely had acquired MAS secondary to TA.
MAS is typically characterized by segmental stenosis or occlusion of the middle portion of the aorta and its branches, with renal artery occlusion being most common, followed by the SMA, abdominal trunk, some iliac vessels, and rarely the IMA. Clinical manifestations vary according to the location and severity of vascular stenosis and can include severe refractory hypertension, abdominal pain, and intermittent claudication.6–8 Vascular aniography is the “gold standard” for diagnosing MAS, although computed tomography angiography (CTA), magnetic resonance angiography (MRA), and ultrasound may also be utilized. MAS is rarely encountered in clinical practice, particularly in older patients. In this case, the patient’s bilateral renal arteries were patent, whereas the SMA, IMA, celiac trunk, and bilateral iliac vessels were occluded. Multiple tortuous arterial collateral circulations were observed in the abdominal wall and retroperitoneum, supplying the intestinal and iliac vessels. The patient’s vascular occlusion pattern is rarely reported in the literature, and the occurrence of abdominal gastrointestinal symptoms is even more uncommon. The patient presented with intestinal obstruction, which may have been caused by long-term ischemia and reperfusion of the intestines, leading to impaired intestinal function and abdominal adhesions.
Due to the rarity of the disease, no definitive optimal treatment has been established. Blood pressure control with medications is a crucial aspect of management, and surgical interventions, including balloon dilation, stent placement, or open surgical reconstruction, are considered based on the patient’s vascular anatomy and overall condition. If left untreated, MAS can lead to severe complications, including hypertension, heart failure, renal failure, recurrent abdominal pain, and intestinal necrosis.9–11 In Japan, six patients with MAS underwent extra-anatomical bypass surgery. A 5-year follow-up demonstrated that this procedure is safe and effective, capable of preventing renal failure and significantly alleviating ischemic symptoms such as headache, abdominal pain, claudication, and heart failure. 11 Additionally, a retrospective study investigating intravascular aortic stent implantation for the treatment of MAS secondary to TA demonstrated that interventional treatment can improve cardiovascular outcomes by enhancing hemodynamics, reversing left ventricular remodeling, and improving cardiac function. 12 In our case, the patient’s hypertension was controlled with oral amlodipine besylate (5 mg, bid), maintaining blood pressure at 130/90 mmHg. Additionally, treatment with nasointestinal obstruction catheter decompression alleviated the patient’s abdominal symptoms. However, recurrent episodes of intestinal obstruction persisted, ultimately necessitating vascular reconstruction. The initial balloon angioplasty was unsuccessful, whereas axillofemoral bypass surgery successfully relieved abdominal and lower limb symptoms. Postoperatively, the patient was maintained on long-term rivaroxaban for anticoagulation. The patient is currently in good condition but requires long-term follow-up by a multidisciplinary team to prevent potential complications, including congestive heart failure and renal dysfunction.
Conclusion
This case report describes an older patient with MAS secondary to TA, who was hospitalized multiple times for recurrent intestinal obstruction, accompanied by hypertension and intermittent claudication. Diagnosis was confirmed via CTA, and the patient’s symptoms were ultimately resolved through nasointestinal obstruction catheter decompression and vascular reconstruction. Further studies are needed to clarify optimal management strategies for MAS, particularly in complex cases and across different age groups.
Footnotes
Acknowledgments
AI tools were employed for language polishing. We confirm that AI was used only for minor language refinement and not for content generation. Furthermore, all AI polished content has been carefully reviewed to ensure no alteration of the original meaning.
Authors’ contributions
Chen Wang, Yu Chen, and Yuqiang Tang wrote the manuscript and prepared the figures. Zhengdong Zhao and Fuwen Luo reviewed the manuscript. All authors have read and approved the final manuscript.
Consent to participate
Informed consent was obtained from the patient and their family for the publication of clinical and imaging data.
Consent for publication
The patient and their family have provided consent for the submission of this case report to the journal.
Data availability
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the study.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This article does not contain any studies with human or animal participants. The research adhered to the principles outlined in the Declaration of Helsinki and obtained exemption from the Medical Ethics Committee of the Second Affiliated Hospital of Dalian Medical University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.