
Abstract
The widespread occurrence and severity of tuberculosis make it a major global health concern. Abdominal issues often affect the intestine, peritoneum, and lymph nodes, with retroperitoneal involvement being rare. We herein present a case involving a 51-year-old man who experienced abdominal pain and fever. He had a history of pulmonary tuberculosis 1 year prior, which had been cured 6 months before presentation to our hospital. Abdominal unenhanced computed tomography revealed incomplete bowel obstruction. Abdominal enhanced computed tomography showed significant enlargement of the retroperitoneal lymph nodes, which were compressing the intestinal lumen. Colonoscopy indicated that the terminal ileum and colon were normal. Ultrasound-guided percutaneous lymph node aspiration was performed, and Mycobacterium tuberculosis fluorescence staining was positive. After anti-tuberculosis treatment, the patient’s abdominal pain and fever improved. Retroperitoneal lymph node tuberculosis presents atypically, and obtaining histopathology early is therefore crucial for diagnosis and treatment.
Introduction
The prevalence and severity of tuberculosis make it a significant global public health issue. 1 If left untreated, tuberculosis can spread widely through blood-borne transmission from an initial infection or the reactivation of dormant illnesses. The intestine, peritoneum, and lymph nodes are frequently affected by abdominal tuberculosis. 2 Incidences of retroperitoneal involvement are rare. 3 The present case study details an intestinal blockage accompanied by a retroperitoneal mass, ultimately diagnosed as tuberculosis. This case emphasizes the importance of timely and accurate diagnosis. This report adheres to the CARE guidelines. 4
Case presentation
A 51-year-old man presented for evaluation of abdominal pain and fever. He had a history of pulmonary tuberculosis 1 year previously, which had been cured 6 months before presentation to our hospital. Abdominal examination revealed tenderness around the umbilicus. Most laboratory test results were within normal limits, including the T-SPOT.TB test, tuberculosis smear fluorescence, erythrocyte sedimentation rate, white blood cell count, serum amylase, prothrombin time, alanine aminotransferase, total bilirubin, creatinine, carbohydrate antigen 199, carcinoembryonic antigen, hepatitis B surface antigen, human immunodeficiency virus antibody, syphilis antibody, anti-nuclear antibody, and hepatitis C antibody. However, significant elevations were found in the serum C-reactive protein level (88.9 mg/L), carbohydrate antigen 125 level (201 kU/L), and D-dimer level (8.25 mg/L) (Table 1).
Patient’s laboratory results.

WBC: white blood cell; N: neutrophil; HB: hemoglobin; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; PT: prothrombin time; ALT: alanine aminotransferase; TB: total bilirubin; Cr: creatinine; CA199: carbohydrate antigen 199; CA125: carbohydrate antigen 125; CEA: carcinoembryonic antigen; TSF: tuberculosis smear fluorescence; HbsAg: hepatitis B surface antigen; HIV-Ab: human immunodeficiency virus antibody; Sp Ab: syphilis antibody; ANA: anti-nuclear antibody; HC Ab: hepatitis C antibody.
An abdominal X-ray and unenhanced computed tomography revealed incomplete bowel obstruction (Figures 1 and 2). Enhanced abdominal computed tomography showed significant enlargement of the retroperitoneal lymph nodes, compressing the intestinal lumen (Figure 3). A subsequent colonoscopy indicated that the terminal ileum and colon were normal (Figures 4 and 5).

Bowel obstruction suggested through abdominal X-ray.

Diagnosis of incomplete bowel obstruction confirmed by abdominal unenhanced computed tomography.

Abdominal enhanced computed tomography showing significant enlargement of retroperitoneal lymph nodes compressing the intestinal lumen.

Normal appearance of the colon under colonoscopy.

Normal appearance of the terminal ileum under colonoscopy.
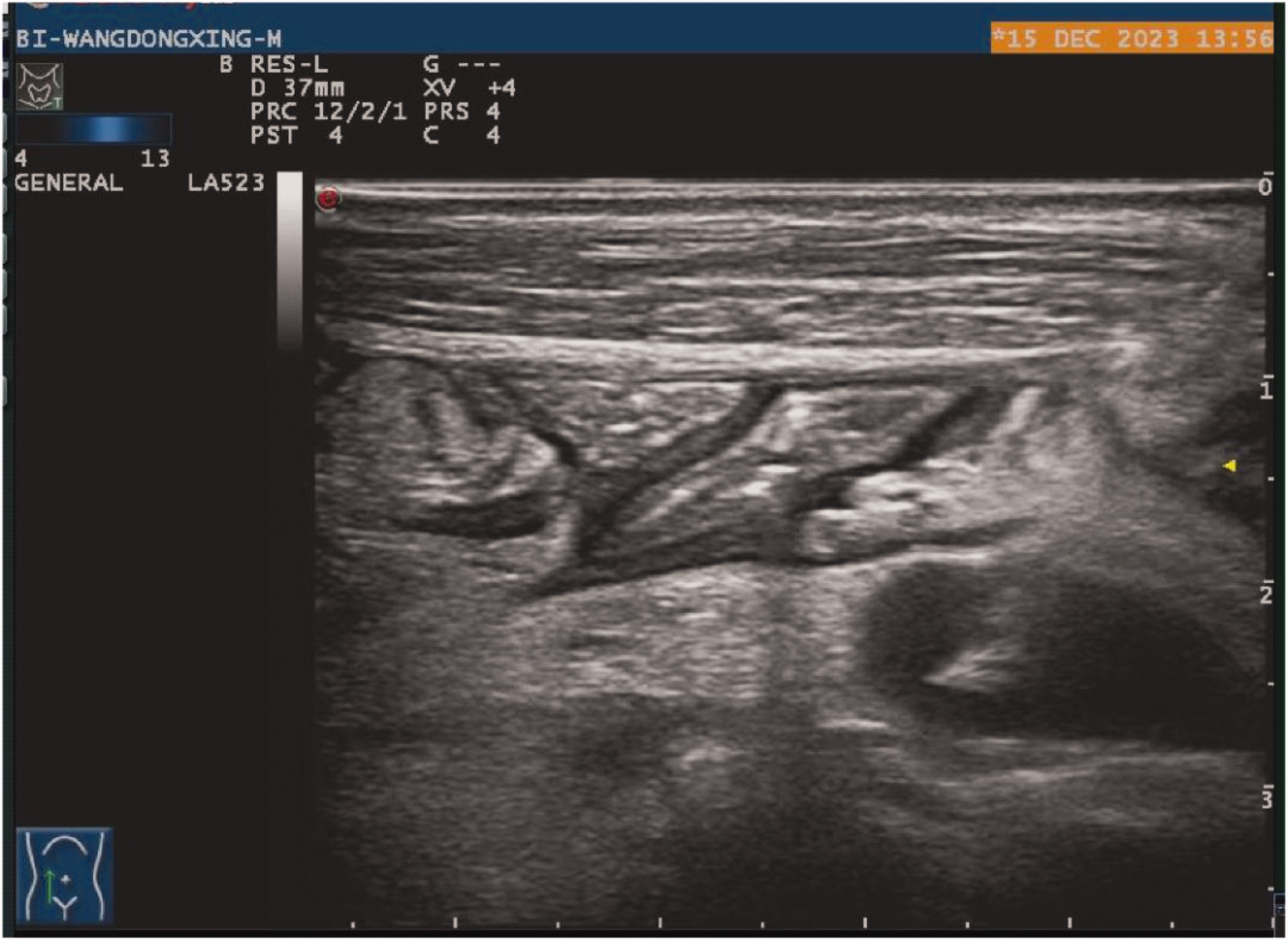
Ultrasound-guided percutaneous lymph node aspiration was performed to clarify the diagnosis (Figures 6–8), and Mycobacterium tuberculosis fluorescence staining was positive (Figure 9). Following anti-tuberculosis treatment, the patient’s abdominal pain and fever improved.
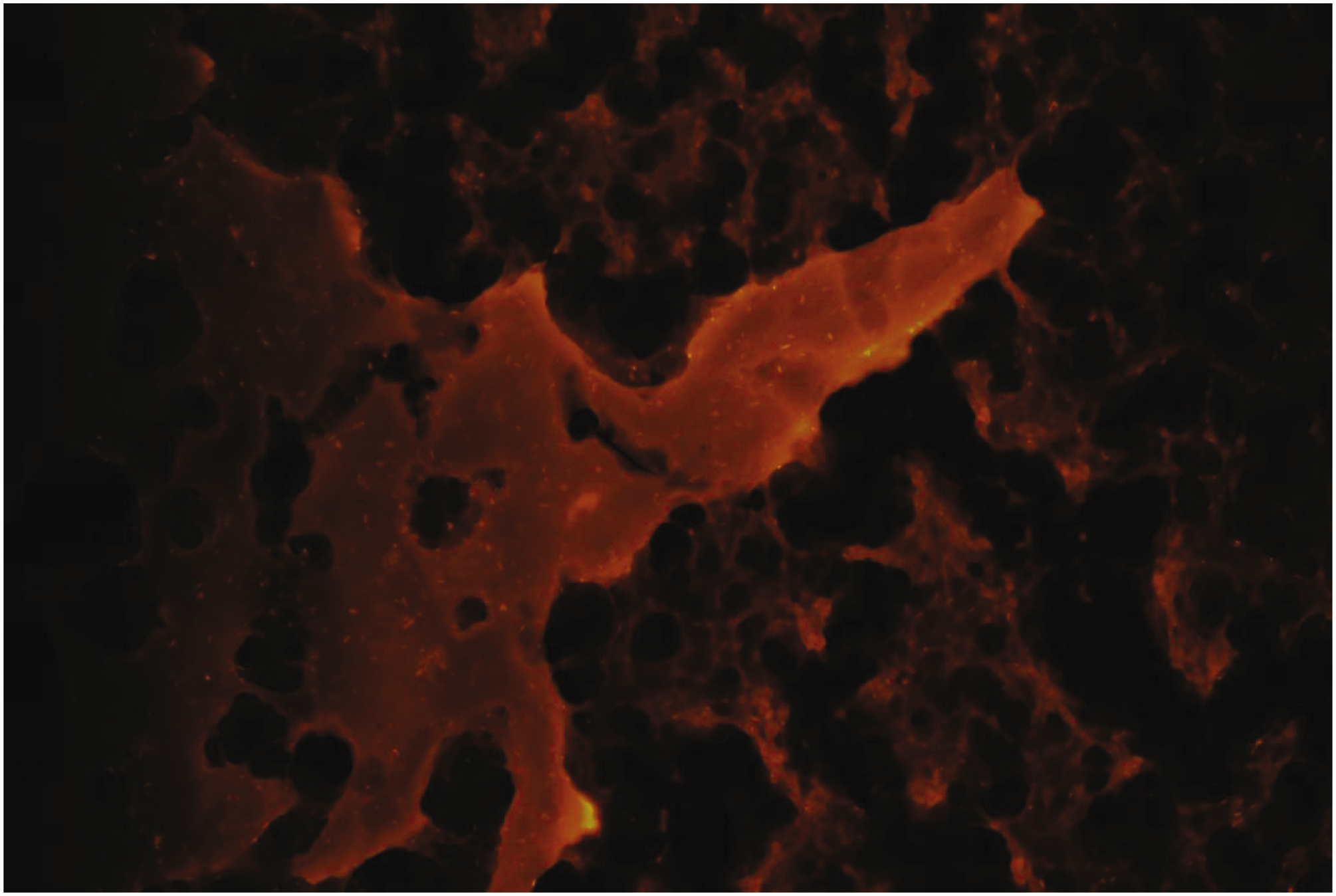
Positive Mycobacterium tuberculosis fluorescence staining.

Retroperitoneal lymph node visualized under ultrasound.
Performance of ultrasound-guided percutaneous lymph node aspiration.
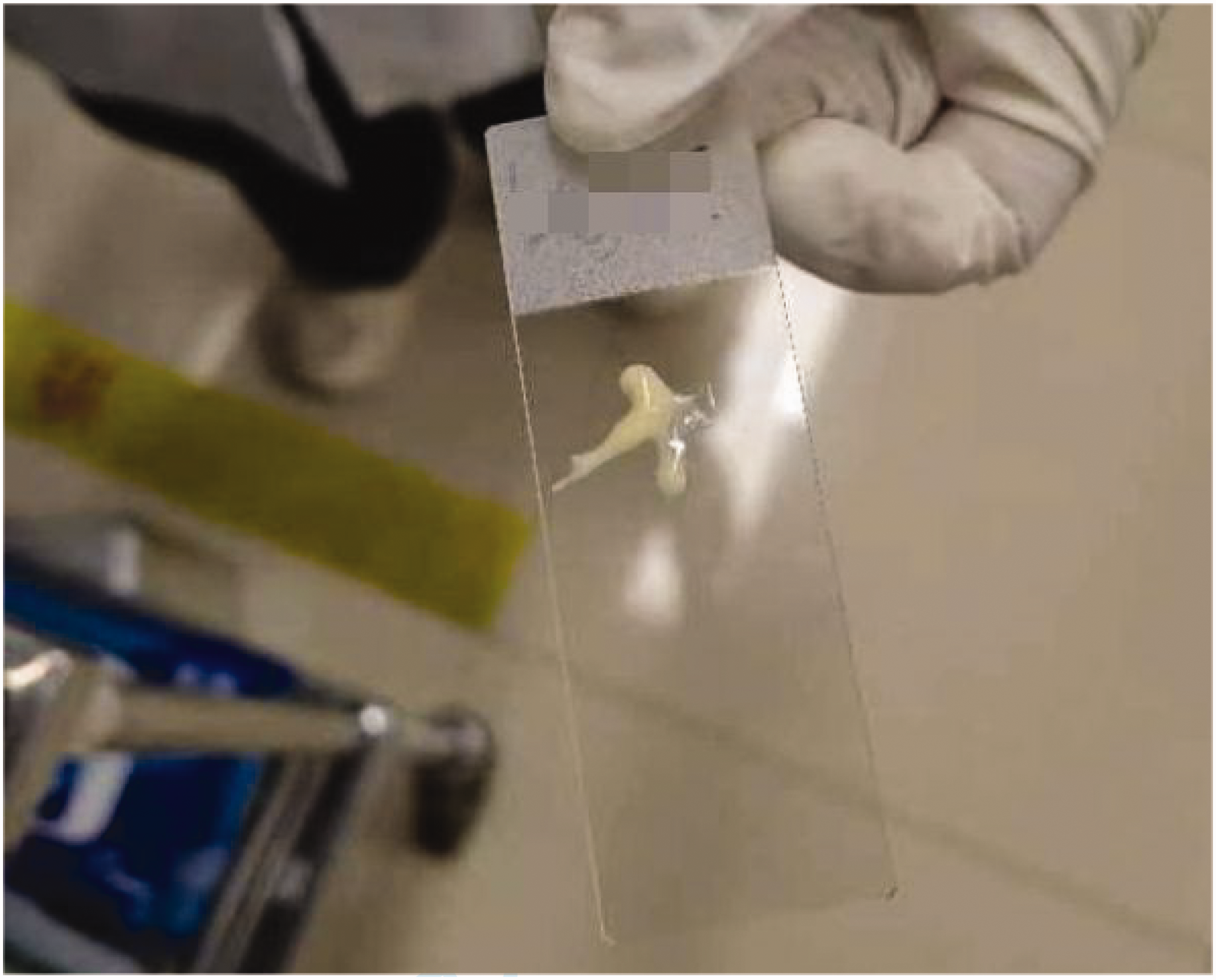
Pus aspirated from the retroperitoneal lymph node.
Discussion
The global burden of tuberculosis is significant, with an estimated 1.7 billion individuals infected by M. tuberculosis. Without treatment, widespread tuberculosis can develop secondary to hematogenous dissemination from the initial infection or the reactivation of dormant disease. 5 The abdominal area is commonly affected, accounting for 5% to 10% of all cases. 6 Reports of retroperitoneal lymph node tuberculosis are rare, and there are no known reports of intestinal obstruction caused by retroperitoneal lymph node tuberculosis. Early detection and appropriate management often result in successful clinical and radiological outcomes of anti-tuberculous therapy. 7
In this case, extrapulmonary tuberculosis was initially not considered because the patient had been cured of pulmonary tuberculosis 6 months earlier. However, his symptoms of abdominal pain and fever persisted despite treatment for intestinal obstruction. Subsequent ultrasound-guided percutaneous lymph node aspiration confirmed retroperitoneal lymph node tuberculosis.
Conclusion
The symptoms of retroperitoneal lymph node tuberculosis are atypical, and histopathological analysis should be performed as soon as possible for early diagnosis and treatment.
Footnotes
Acknowledgement
The authors thank Professor Delin Liu for his assistance in the diagnosis of this case.
Author contributions
Yuandong Zhu designed the study. Fulong Zhang wrote the manuscript. Jing Xu collected the clinical information. Yuandong Zhu revised the manuscript. All authors read and approved the final manuscript.
Data availability statement
The data analyzed in this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Ethics approval and consent to participate
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the ethics review committee of HangZhou XiXi Hospital (202401141400000250708). The committee waived the requirement for informed consent.
Funding
No funding was received for this study.