
Abstract
Introduction
This retrospective study evaluated the preliminary results of combining retrograde tibial intramedullary nail with lateral less invasive stabilization system for treating distal femoral fractures.
Patients and methods
This retrospective analysis included 11 patients with distal femoral fractures who were treated with retrograde tibial intramedullary nail and less invasive stabilization system. The collected data included patient demographics, injury mechanism, surgery duration, intraoperative blood loss, bone union time, femoral–tibial angle, visual analog scale scores, knee range of motion, Hospital for Special Surgery scores, and complications.
Results
The surgery duration ranged from 83 to 115 min, and blood loss varied from 120 to 210 mL. Patients were monitored for 9 to 15 months, achieving complete bone healing and full weight-bearing within an average duration of 5.3 ± 0.8 months and 55.7 ± 6.5 days, respectively. At the final follow-up, the visual analog scale scores ranged from 0 to 3, and the femoral–tibial angle measurement ranged from 169° to 174°. The knee range of motion ranged from 120° to 135°, and Hospital for Special Surgery scores ranged from 69 to 95. One patient developed a superficial incisional infection; no other complications were observed.
Conclusion
The primary outcomes demonstrated that the retrograde tibial intramedullary nail–less invasive stabilization system combination provides stable fixation with minimal surgical trauma, rapid recovery, and a low complication rate, leading to favorable outcomes in distal femoral fracture management.
Keywords
Introduction
Distal femoral fractures, located within 9 cm of the joint surface and affecting the metaphysis or joint, account for approximately 1% of all fractures and 3%–6% of femoral fractures. Among these, Arbeitsgemeinschaft für Osteosynthesefragen (AO)/Orthopaedic Trauma Association (OTA) Classification of Fractures and Dislocations type A is the most prevalent, representing approximately 47% of cases. 1 These fractures follow a bimodal distribution: younger males typically experience high-energy trauma, while older females are more prone to low-energy injuries. 2 These fractures frequently present with displacement, comminution, and intra-articular involvement and may occasionally require open treatment, which is further complicated by significant deforming forces exerted by the surrounding musculature. 3
Surgical intervention remains the standard treatment, aiming for anatomical reduction, stable fixation, and early rehabilitation. 4 However, in cases of complex fractures, such as in the presence of medial supracondylar bone loss, low trans-condylar bicondylar fractures, periprosthetic fractures, nonunion following less invasive stabilization system (LISS) fixation, severe osteoporosis, and highly comminuted fractures, 5 LISS plate fixation may be unstable due to inadequate screw anchorage, insufficient bone engagement, or a lack of medial femoral support. This instability increases the risk of complications, including fracture displacement, bone resorption, and hardware loosening or breakage during early rehabilitation, leading to a high complication rate in complex distal femoral fractures treated with LISS plates.6,7
Stable fixation is essential for optimal biomechanical conditions that promote healing and enable early weight-bearing in complex distal femoral fractures. 8 To reduce the complications associated with single-method fixation, combined techniques are commonly employed, such as dual plating on the medial and lateral sides 9 or retrograde femoral intramedullary nailing with LISS. 10 Medial locking plates provide greater reductive control and stability in cases of medial comminution, preventing the characteristic “golf club” deformity associated with single LISS plating. 11 They are particularly beneficial for patients with medial bone defects or osteoporosis. However, the absence of specialized medial plates for distal femoral fractures 12 and the risk of neurovascular injury due to the complex medial anatomy remain significant concerns. 13 Retrograde femoral intramedullary nails are generally ineffective for periprosthetic fractures following closed-box total knee arthroplasty (TKA) 14 and require insertion through the knee joint, potentially compromising postoperative knee function. These limitations highlight the need for innovative combined fixation strategies for complex distal femoral fractures.
Retrograde tibial nails (RTNs) are widely used for distal tibial fractures due to their favorable biomechanical properties and clinical outcomes.15,16 Although previous studies, including our study,17,18 have demonstrated their effectiveness, their application in distal femoral fractures has not yet been explored. This primary study evaluated the clinical efficacy of a novel combined fixation technique—RTN with LISS—in treating distal femoral fractures.
Patients and methods
Patient selection
This retrospective study was conducted at a Level 1 trauma center between June 2021 and December 2022, adhering to the ethical principles of the Declaration of Helsinki (1975), as revised in 2024. The reporting of this study conforms to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 19 Informed consent was obtained from all 11 participants, and we have de-identified all patient details in this study.
The inclusion criteria encompassed the following: (a) distal femoral fractures classified as AO/OTA types A2, A3, C1, or C2 as well as periprosthetic distal femoral fractures post-TKA classified as Rorabeck types I and II and (b) patients aged ≥18 years with fully developed skeletal structures. The exclusion criteria included the following: (a) patients aged <18 years or those with immature distal femoral epiphyseal closure; (b) pathological or old fractures; (c) peripheral nerve or vascular injuries; (d) inadequate follow-up data or follow-up duration <3 months; and (e) major organ injuries contraindicating surgery.
Preoperative preparation
Preoperative assessment involved a comprehensive medical history review, thorough physical examination, and imaging studies, including full-length femur X-rays, anteroposterior and lateral knee and ipsilateral hip views, and three-dimensional computed tomography of the knee.
For open fractures, debridement, suturing, and temporary external fixation were performed upon admission, accompanied by antibiotic administration. The timing of secondary surgery was determined based on the wound healing progress. External fixation was removed 2 days prior to definitive surgery once the wound and pin sites were dry. For closed fractures, the affected limb was elevated, and tibial tubercle traction was applied preoperatively.
Surgical procedure
The patient was placed in the supine position under spinal or general anesthesia. A translucent triangular pad was positioned in the popliteal fossa to maintain approximately 30° of knee flexion, and gentle longitudinal traction was applied to suspend the affected limb. A lateral incision was made over the lateral femoral condyle, extending to the tibial tubercle. The subcutaneous tissue and fascia lata were dissected to expose the femoral condyles. For C1 and C2 fractures, hematoma evacuation was performed, and the intercondylar fragments were reduced and temporarily stabilized with 2.0-mm Kirschner wires. Reduction was confirmed using C-arm fluoroscopy before definitive fixation with cannulated screws. A 5.0-mm Schanz screw was inserted into both the proximal femur and tibia, followed by the application of a lower limb traction device. Under fluoroscopic guidance, traction was applied to restore femoral length. If the alignment remained unsatisfactory, posterior angulation was corrected using a towel roll placed beneath the femoral shaft, while varus or valgus deformities were adjusted with bone-holding forceps. Following reduction, an appropriately sized LISS plate (Double Medical Technology Inc., Xiamen, China; titanium alloy) was inserted through the distal femoral incision and positioned across the fracture site. Screw holes were drilled, and single cortical locking screws were initially placed to prevent interference with RTN insertion. Subsequently, these screws were replaced with definitive fixation. Fluoroscopy was used to confirm proper alignment, and the femoral length was compared with that of the contralateral limb to ensure anatomical restoration.
A 2-cm longitudinal incision was made over the medial epicondyle. After dissecting the subcutaneous tissue, the medial epicondyle was exposed, identifying the attachment sites of the medial collateral ligament, adductor magnus, and medial head of the gastrocnemius. The RTN entry point was located approximately 0.5 cm anterior to the medial epicondyle. A guide wire was inserted at an angle of approximately 40° to the femoral mechanical axis in the anteroposterior view, ensuring alignment with the RTN curvature. In the lateral view, the guide wire was centered within the femoral canal. A hole reamer and cannulated awl were advanced along the guide wire to create a pathway into the medullary canal while preserving the medial collateral ligament and adjacent structures. The RTN (Double Medical Technology Inc., Xiamen, China; titanium alloy; diameter: 8.0 mm ×length: 140 mm) was assembled onto the targeting device and inserted with controlled force and slight rotational movements until flushing with medial epicondyle of the femur. Fluoroscopy confirmed proper reduction and nail positioning. Three distal cancellous locking screws and two proximal cortical locking screws were inserted using the targeting device, and an end cap was placed at the tip of the nail (Figure 1).

A diagram of combined RTN and LISS plate fixation in complex distal femoral fractures (AO/OTA A3). The green implant indicates the LISS plate, and the blue implants represent the locking screws of the LISS plate. The red implant indicates RTN, and the yellow implants represent the five locking screws of the RTN. AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.
Postoperative management
Anticoagulation therapy was initiated 12 h postoperatively, and prophylactic antibiotics were administered for 24 h. Starting on the first postoperative day, quadriceps isometric exercises and hip and knee flexion–extension movements were performed. The range of motion (ROM) was progressively increased based on pain tolerance, initially starting with full extension and advancing to 70° of flexion. These exercises were continued for a minimum of 2 weeks or until pain-free active movement was achieved.
Outcome assessment
The key perioperative parameters, including operative duration, intraoperative blood loss, and complications, were recorded. Follow-up evaluations included routine clinical visits and monthly X-rays performed to assess bone healing. Pain levels and functional outcomes were measured using the visual analog scale (VAS), femoral–tibial angle measurements, Hospital for Special Surgery (HSS) scores, and knee ROM. Early weight-bearing was encouraged, with partial weight-bearing using crutches initiated 2–4 weeks postoperatively. The transition to full weight-bearing was determined based on fracture characteristics, bone integrity, soft tissue status, and patient tolerance, with the timing documented accordingly.
Results
The study included 11 patients (5 males, 6 females) aged 28–80 years (mean: 56.5 ±17.5 years). The injury mechanisms included traffic accidents (four cases), falls from heights (one case), tumble injuries (falls and stumbling, four cases), and crush injuries (two cases). Fractures were classified according to the AO/OTA system: two cases each of type A2, A3, C1, and C2. Additionally, three patients with femoral periprosthetic fractures following TKA were classified as type II per the Rorabeck’s system. One patient sustained an open fracture (Gustilo IIIA). Associated injuries included rib fractures (three cases), hemopneumothorax (one case), ipsilateral calcaneal fracture (one case), and ipsilateral metatarsal fracture (one case) (Table 1).
Characteristics of the patients.
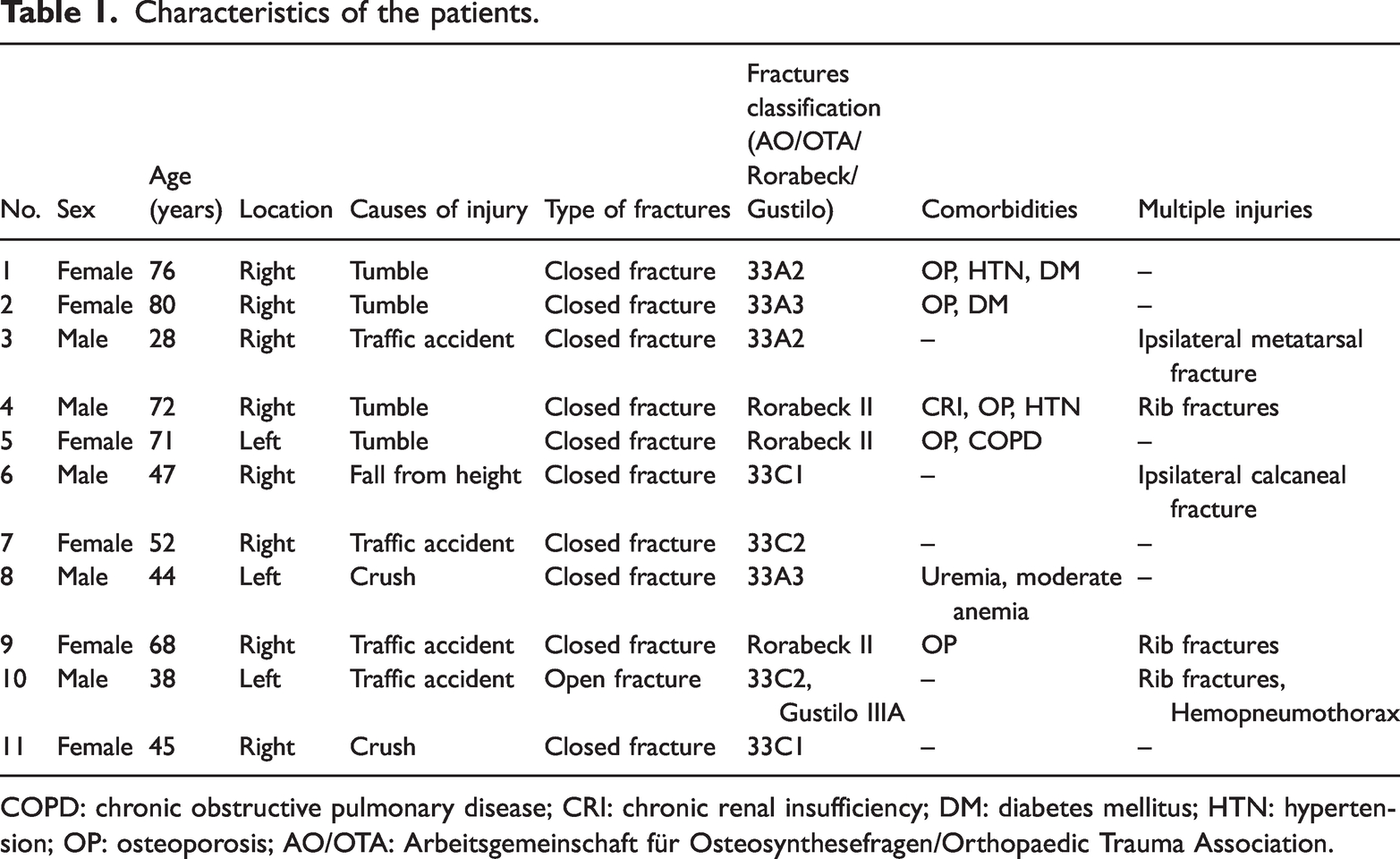
COPD: chronic obstructive pulmonary disease; CRI: chronic renal insufficiency; DM: diabetes mellitus; HTN: hypertension; OP: osteoporosis; AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.
The surgery duration ranged from 83 to 115 min (mean: 98.3 ± 9.0 min), with intraoperative blood loss ranging from 120 to 210 mL (mean: 167.8 ± 24.3 mL). Six patients with preoperative anemia required homologous packed red blood cell transfusions intraoperatively or postoperatively. Bone defects in five patients were managed with allografts or autologous iliac bone grafts.
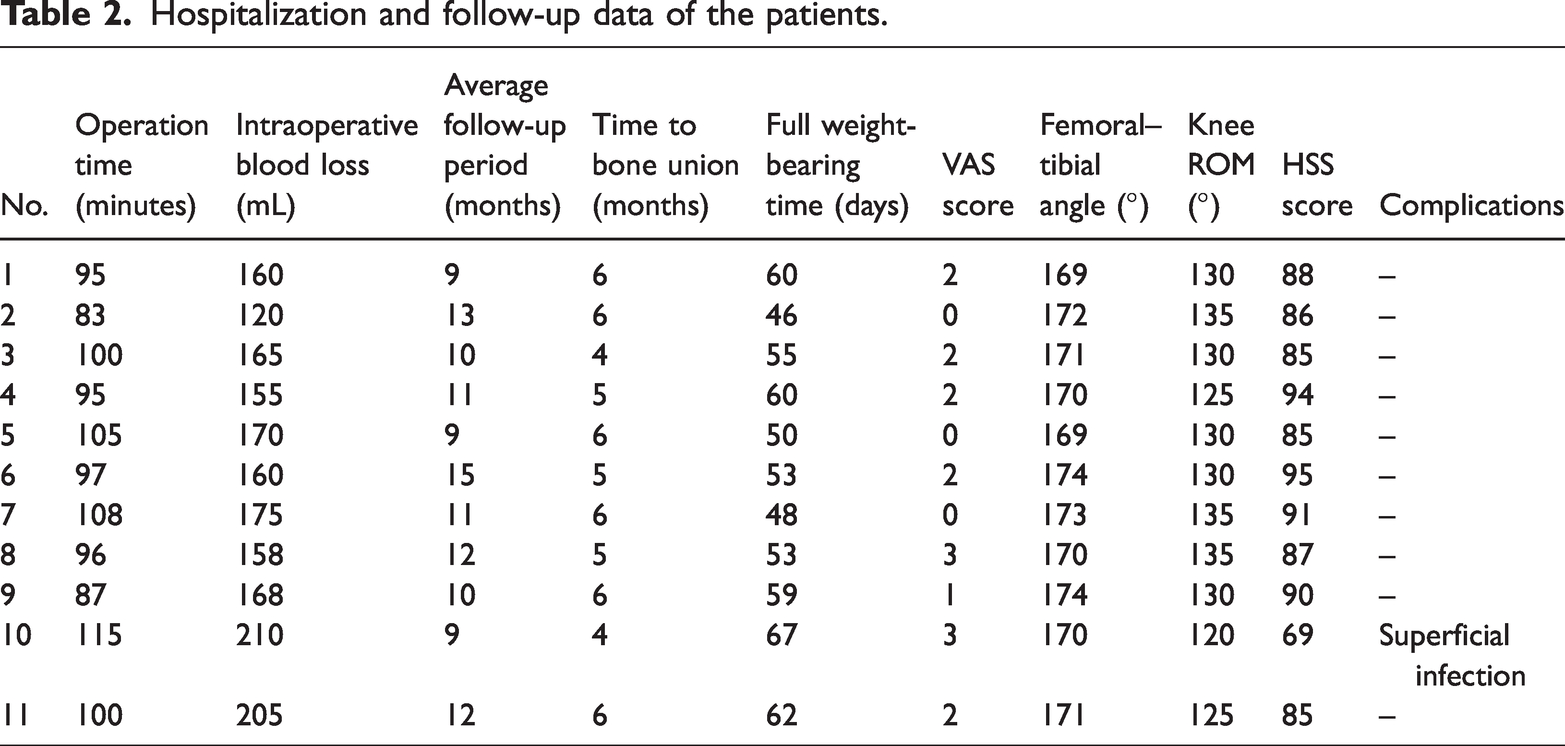
Follow-up ranged from 9 to 15 months (mean: 11.0 ± 1.9 months). Fracture healing occurred within 4–6 months (mean: 5.3 ± 0.8 months), and full weight-bearing was achieved between 46 and 67 days postoperatively (mean: 55.7 ± 6.5 days). At the final follow-up, the VAS scores ranged from 0 to 3 (mean: 1.5 ± 1.1), the femoral–tibial angle from 169° to 174° (mean: 171.2° ± 1.8°), knee ROM from 120° to 135° (mean: 129.5° ± 4.7°), and HSS scores from 69 to 95 (mean: 86.8 ± 6.9). The clinical outcomes were rated as excellent in six cases, good in four, and fair in one, yielding a 90.9% excellent-to-good rate. One patient developed a superficial infection, which resolved with debridement, drainage, and dressing changes. No other complications, including neurovascular injury, fracture displacement, delayed healing, nonunion, limb length discrepancy, malalignment, or hardware failure, were observed (Table 2).
Hospitalization and follow-up data of the patients.
Representative cases are illustrated in Figure 2 (Case 5), Figure 3 (Case 2), Figure 4 (Case 7), and Figure 5 (Case 1).
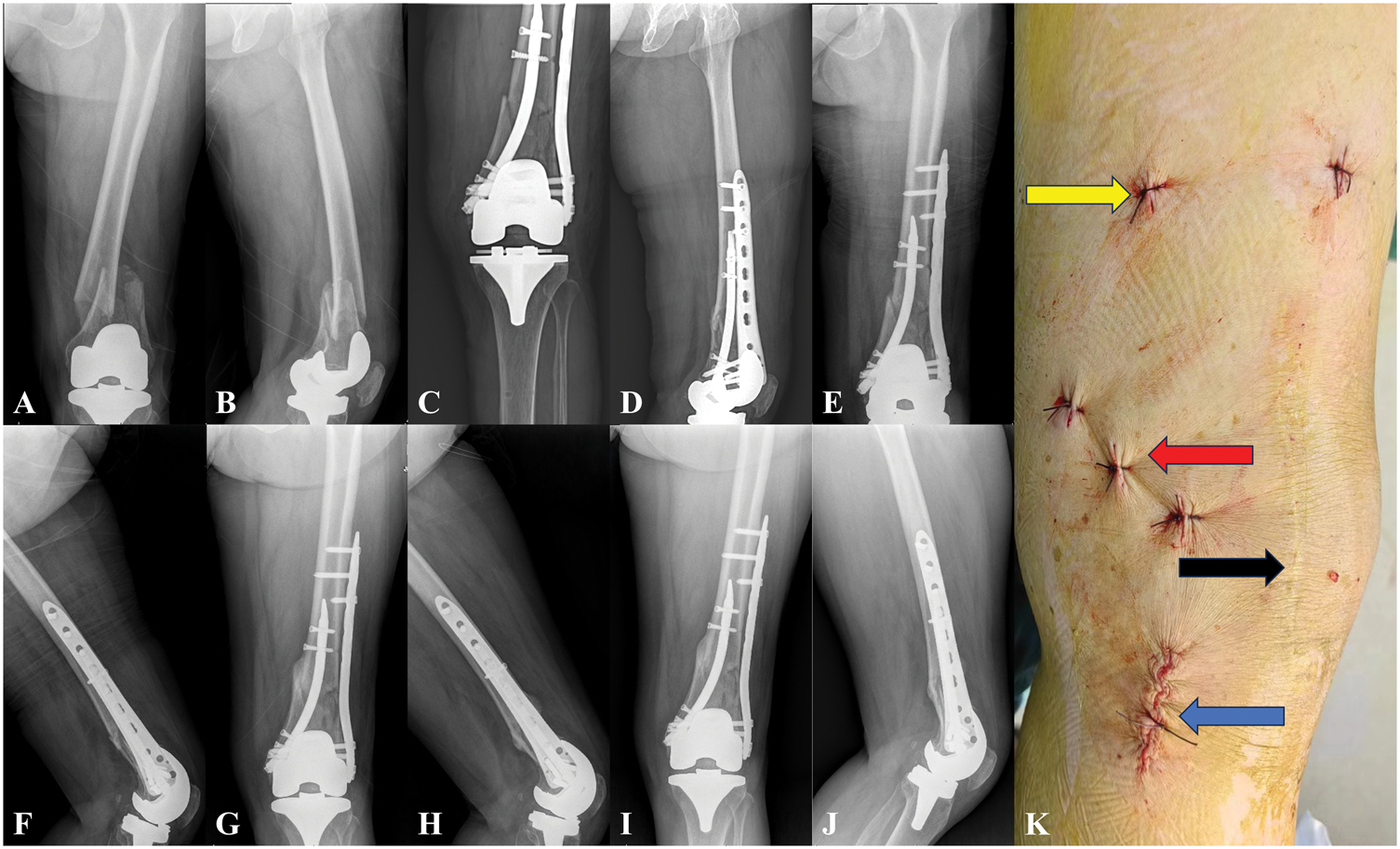
A 71-year-old female patient presented with a periprosthetic femoral fracture (Rorabeck Type II) following left TKA. (a, b) Preoperative anteroposterior and lateral radiographs revealed a distal femoral fracture; (c, d) the patient underwent combined RTN and LISS plate fixation. X-ray at 3 days postoperatively; (e, f) radiographs taken 1 month postoperatively; (g, h) radiographs taken at postoperative 3 months showed partial callus formation; (i, j) radiographs at 6 months confirmed successful bone union and (k) the black arrow indicates the previous knee arthroplasty incision, the blue arrow shows the RTN entry point, the red arrow highlights the three distal locking screws, and the yellow arrow marks the two proximal locking screws.

An 80-year-old female patient presented with a fracture of the right distal femur (AO/OTA 33A3). (a–c) Preoperative radiographs and CT revealed a low trans-condylar bicondylar fracture; (d, e) the patient underwent RTN and LISS plate fixation and allograft bone grafting; (f, g) radiographs taken 3 months post-surgery indicated mild medial cortical resorption in the distal femur; (h, i) radiography at postoperative 6 months. Fracture union was observed. AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.

A 52-year-old female patient presented with a fracture of the right distal femur (AO/OTA 33C2). (a–c) Preoperative radiographs and CT identified the fracture; (d–f) the patient underwent an operation with combined RTN and LISS plate fixation. Postoperative radiographs and CT confirmed proper fracture reduction, alignment, and implant placement, despite medial cortical deficiency post-reduction; (g, h) radiographs at postoperative 2 months; (i, j) radiographs at 6 months postoperatively confirmed bone union. AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.

A 76-year-old female patient presented with a fracture of the right distal femur (AO/OTA 33A2). (a–d) Preoperative radiographs and CT identified the fracture; (e, f) the patient underwent an operation with combined RTN and LISS plate fixation and allograft bone grafting. Fracture union was observed at 6 months. AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.
Discussion
Distal femoral fractures pose significant challenges in orthopedic trauma due to factors such as patient age, soft tissue injury, fracture extension, articular involvement, comminution, and fragment size, all of which complicate the prognosis. 20 The surgical options include plating, retrograde intramedullary nailing (locking and nonlocking), 21 and joint replacement. 22 Previous studies have shown good subjective and objective results, which could be provided by plating as well as locking and nonlocking retrograde intramedullary nailing. 23 Locking lateral plates, such as LISS, are widely used due to their minimally invasive application, angular stability, resistance to multi-planar forces, and enhanced fixation in osteoporotic bone. However, they are associated with high rates of nonunion, varus collapse, and implant failure. 24 Retrograde femoral intramedullary nails reduce soft tissue damage and promote bone healing through canal reaming but exhibit nonunion rates similar to LISS, particularly in older patients with poor bone quality. 25 For patients with severe bone loss, pre-existing osteoarthritis, or joint contractures, joint replacement serves as an alternative. 26 However, internal fixation remains the preferred approach due to its lower infection rates, reduced revision surgeries, and lower mortality compared with joint replacement. Given the limitations of single-method fixation, combined techniques have gained traction in the management of complex distal femoral fractures, 27 particularly in cases involving medial supracondylar or cortical bone defects, low-level bicondylar fractures, medial Hoffa fractures, periprosthetic fractures post-TKA, nonunion following LISS, and osteoporotic comminuted fractures (AO/OTA C3). Combined fixation provides superior stability over LISS or retrograde nailing alone, enabling earlier weight-bearing, especially in patients with osteoporosis. 10 Biomechanical studies have demonstrated a 70% increase in the axial load stiffness when a medial plate is added to a single lateral plate in an AO/OTA 33 C fracture model. 28 The torsional stiffness of a dual-plate construct is 2.6 times that of a single lateral plate and 5.4% greater than a retrograde femoral nail. 29 In a series of nine patients with noncomminuted distal femoral fractures, combining retrograde nails with lateral locking plates facilitated early weight-bearing, with complete healing within an average duration of 20 weeks. 30 A retrospective study of 67 cases, including native and periprosthetic fractures, further demonstrated that nail-plate fixation significantly improved the rates of union and allowed earlier weight-bearing compared with single-plate fixation. 31
Despite the advantages of combined fixation, several limitations remain. The limitations of dual-plate fixation are as follows: 1. A medial incision increases soft tissue disruption and heightens the risk of neurovascular injury. 32 2. Although anatomically designed plates exist for lateral femoral condyle fixation, no specific implants are available for medial distal femur fractures. 12 The current medial plates include proximal humeral locking plates, medial proximal tibial locking plates, limited-contact dynamic compression plates, and endosteal substitution plates.14,33 The limitations of nail-plate fixation are as follows: 1. Retrograde femoral intramedullary nailing is challenging in patients with closed-box TKA. 2. Extremely distal fractures may not be amenable to retrograde nailing, even with advanced implants. 3. In cases of ipsilateral total hip arthroplasty, shorter nails and lateral plating are necessary to bridge stress risers. 4. Retrograde nailing requires a longitudinal incision through the patellar tendon and joint capsule, along with intercondylar drilling, increasing the risk of postoperative adhesions, knee pain, and functional impairment. These challenges limit the widespread use of dual-plate and nail-plate fixation in distal femoral fractures, highlighting the need for improved fixation strategies.
RTN, a minimally invasive technique for distal tibial fractures, was first introduced by Hofmann et al. in the late 1990s. 34 Its banana-shaped distal curvature aligns closely with the tibial anatomy. In this study, RTN was innovatively applied as medial supplemental fixation for distal femoral fractures. Our previous biomechanical research demonstrated that RTN combined with an LISS construct provides superior biomechanical stability compared with dual-plate and nail-plate fixation for comminuted distal femoral fractures. 35 RTN offers several advantages: 1. Minimally invasive approach. A 2-cm incision at the medial femoral epicondyle enabled RTN insertion, with five locking screws placed using a targeting device, minimizing soft tissue trauma. 2. Central stabilization. Positioned within the femoral medullary canal, RTN provides stability comparable to retrograde intramedullary nails without affecting the neurovascular structures along the medial femur. 3. Preserved knee joint integrity. Unlike retrograde nails, RTN is inserted through the medial epicondyle, avoiding knee joint disruption. Patients exhibited favorable knee function, with a mean VAS score of 1.5 ± 1.1, knee ROM of 129.5° ± 4.7°, and HSS score of 86.8 ±6.9, achieving a 90.9% excellent-to-good outcome, comparable to dual-plate fixation. 36 4. Precise screw placement. The shorter length of RTN and targeting device improve the locking screw accuracy, reducing intraoperative fluoroscopy and surgical duration. In this study, the mean operation time was 98.3 ± 9.0 min, with an average blood loss of 167.8 ± 24.3 mL, surpassing the outcomes reported for nail-plate fixation. 37 5. Early functional recovery. RTN provides stable fixation, facilitating early knee mobilization and weight-bearing. Bone union was achieved within a mean duration of 5.3 ± 0.8 months, with full weight-bearing initiated at 55.7 ± 6.5 days. The mean femoral–tibial angle was 171.2° ± 1.8°. A previous study showed that distal femoral fractures using nail-plate fixation enabled early weight-bearing compared with single-plate fixation. 31 RTN enabled even faster healing and earlier weight-bearing than dual-plate or nail-plate constructs. 38 6. Low complication rate. The minimally invasive insertion of both LISS and RTN resulted in fewer complications than dual-plate fixation. Only one patient, who had uremia, developed a superficial infection, which was resolved with debridement. No cases of delayed union, nonunion, or fixation failure were observed. These findings highlight RTN as a promising adjunct for distal femoral fracture fixation, offering biomechanical advantages, reduced surgical trauma, and enhanced clinical outcomes.
The preliminary results demonstrated that RTN offers effective central stabilization, supports early functional recovery, and has a low complication rate, making it a promising alternative to conventional fixation methods for distal femoral fractures. As a medial supplemental fixation for comminuted fractures, RTN enhances medial support, improves alignment, and adheres to key biomechanical principles, facilitating bone healing and enabling early weight-bearing. Moreover, it is minimally invasive, technically straightforward, and preserves the medial neurovascular structures and knee joint function.
However, this primary study has certain limitations: 1. Retrospective design. The study design may introduce selection and information biases. 2. Small sample size. The limited cohort and short follow-up (mean: 11.0 ± 1.9 months) hinder the assessment of long-term outcomes and complications. The initial objective of including 30 patients within 1 year was not achieved. We extended the enrollment period by 6 months; however, only 13 people were registered, and 11 cases were followed up. 3. Lack of a control group. The absence of a comparative cohort limits the strength of the conclusions. Due to the small number of cases and the study design, it was not possible to compare the treatment results with those of a control group. Thus, we compared and examined the clinical results by conducting a literature review.
Future research should prioritize the following: 1. Biomechanical and clinical trials. Comparative studies, including randomized controlled trials, are needed to assess the biomechanical performance and clinical efficacy of RTN relative to LISS plates, dual-plate constructs, and nail-plate fixation. 2. Implant optimization. The development of specialized retrograde intramedullary nails for medial femoral condyle fixation could enhance the clinical outcomes.
Conclusion
The combined use of RTN and LISS plating could provide a minimally invasive and effective strategy for managing distal femoral fractures. This innovative technique may enhance stability, accelerate recovery, and minimize postoperative complications, resulting in favorable clinical outcomes. Future large-scale prospective comparative studies should be conducted to confirm the aforementioned findings.
Footnotes
Acknowledgements
We would like to thank the participants included in the current study and all physicians and nurses involved in the management of the patients.
Authors’ contributions
Huiyun Deng: Writing the paper, data analysis and collection.
Tianlai Chen: Data collection.
Hui Liu: Writing the paper, data analysis and collection.
Weibin Lin and Weizhen Xu: Searching the related articles, data analysis.
Jin Wu: Data collection, surgeries, research team manager.
All authors have contributed significantly and are in agreement with the content of the manuscript.
Authorship declaration
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors are in agreement with the manuscript.
Consent for publication
All patients or their families signed the informed consent before surgery and provided the consent to publish and report individual clinical data.
Data availability
All data supporting the findings of this study are available within the paper.
Declaration of conflicting interests
The authors declare no competing interests.
Disclosure statement
The corresponding author declares, on behalf of all the authors, that there are no conflicts of interest. The paper is NOT based on a previous communication to a society or meeting.
Ethics approval and consent to participate
This study was performed in accordance with the Helsinki Declaration of 1975, as revised in 2024 and was exempted by the Ethics and research committee at The Affiliated Dongnan Hospital of Xiamen University. Informed consent was obtained from all participants to participate in the study after full explanation of the study procedures.
Funding
No Funding.