
Abstract
Objective
To evaluate the effectiveness of retrograde tibial intramedullary nail (RTN) in addressing nonunion in the distal one-fourth of the tibia.
Methods
This retrospective study included consecutive patients who were treated with RTN for nonunion in the distal one-fourth of the tibia between December 2020 and August 2023. Data regarding age, sex, injury mechanism, fracture type, initial fixation method, nonunion duration and type, risk factors, surgical duration, hospital stay, time to bone union, ankle function at final follow-up, and any complications were extracted from hospital records and analysed.
Results
Five patients in total were included, with previous treatments comprising locking plates and/or external fixation. The mean duration of RTN surgery was 94.0 ± 13.7 min, and mean duration of hospital stay was 9.8 ± 1.9 days. Patients were monitored for 10–18 months post RTN, achieving complete bone healing within a mean of 4.8 months. At the latest follow-up, the mean American Orthopedic Foot and Ankle Society (AOFAS) score was 84.4 ± 6.8 (range, 77–95). No complications, such as infection, reoperation, implant issues, rotational deformity, or shortening were reported.
Conclusion
RTN emerges as a dependable, minimally invasive, and safe treatment modality for managing nonunion in the distal one-fourth of the tibia.
Keywords
Introduction
Fracture healing is a complex process influenced by various factors, with the blood supply and mechanical stability at the fracture site being essential. 1 Distal tibial fractures are the most common long bone fractures, 2 however nonunion in the distal tibia is uncommon, with occurrence rates reported between 1% and 17% in the literature. 3 This rarity is partly due to the rapid healing of periarticular cancellous bone compared with compact cortical bone, as it uses existing trabecular surfaces for new bone growth. 4 Additionally, a robust blood supply from metaphyseal vessels and nutrient arteries aids healing in the distal tibia. 5
However, nonunion in the distal tibia can still occur, presenting treatment challenges due to the short, osteopenic bone segment, proximity to the ankle joint, and delicate soft-tissue envelope from previous surgeries. 6 Treatment options include surgical and non-surgical methods. Non-surgical approaches typically involve early weight-bearing, electromagnetic field stimulation, low-intensity pulsed ultrasound, percutaneous bone marrow aspirate injection, and extracorporeal shock wave therapy. 7 Surgical options often include intramedullary nailing, fine wire/ring external fixation, and plate reconstruction.8,9 Each technique has its specific applications and potential complications; for example, plate reconstruction in compromised soft tissue may lead to wound complications and infections. 10 Moreover, the unique shape and widening of the distal tibial canal may result in poorly fitting intramedullary nails, causing instability and persistent nonunion or malunion. 11
Effective treatment of distal tibial nonunion requires careful planning, considering the soft tissue condition, vascular challenges, and mechanical stability. The aim of the present retrospective study was to analyse cases of distal tibial nonunion successfully treated with retrograde tibial intramedullary nail (RTN).
Patients and methods
Study population and study parameters
This retrospective study included consecutive patients who were treated by RTN between December 2020 and August 2023 for nonunion of the distal one-fourth of the tibia.
All patients who met the following inclusion criteria were enrolled: a nonunion in the distal one-fourth of the tibia without the fracture line penetrating the articular platform, skeletal maturity, and a follow-up period of at least 10 months. Patients who met the following criteria were excluded: aged <18 years, underwent surgery for nonunion or malunion in the proximal or middle tibia, and/or received <10 months of follow-up. Nonunion was defined as an unhealed fracture after 9 months with no healing progress during the previous 3 months.
Clinical case data regarding patient age, sex, injury mechanism, fracture type, initial fixation method, nonunion duration and type, risk factors, surgical duration, hospital stay, time to bone union, ankle function at final follow-up, and any complications were extracted from hospital records and reviewed.
This retrospective clinical study was approved by the Xiamen University Institutional Review Board and written informed consent for treatment and study inclusion was obtained from each patient preoperatively. All patient details were deidentified and the study adhered to the ethical standards outlined in the Helsinki Declaration of 1975 as revised in 2013 and the protocols of the institutional research committee. The reporting of this study conforms to STROBE guidelines. 12
Surgical techniques
Under general or epidural anaesthesia, patients were positioned supine on a fluoroscopic surgical bed. Depending on the condition of the soft tissue, a 3–4 cm incision was made to access the nonunited fracture site, and necrotic bone and scar tissue were excised manually. A second incision, 2–3 cm long, was made at the medial malleolus for dissection. A guide wire was inserted at the midpoint of the medial malleolus, with its position confirmed using C-arm fluoroscopy in both anteroposterior and lateral views. The guide wire was aligned parallel to the medial cortex in the anteroposterior view and with the distal tibia's axis in the lateral view. Access to the medullary canal was achieved with a cannulated awl and reamer following the guide wire. Prosthesis trials determined the correct diameter and length for the RTN (Double Medical Technology Inc., Xiamen City, China). The RTN was connected to the aiming device and gently inserted into the medullary canal with a twisting motion until it was flush with the medial malleolus cortex. C-arm fluoroscopy confirmed correct reduction and nail placement (RTN illustrated in Figure 1). Distal and proximal locking screws were inserted using the target device and trocar, and an end cap was attached at the nail's end. An iliac crest bone graft was utilized for one patient with atrophic nonunion.

Illustration of retrograde tibial intramedullary nail application in the distal tibia.
Postoperative management
Following the procedure, patients routinely received antibiotic treatment for 24 h (intravenous infusion of 0.75 g cefuroxime, twice daily) and began active and passive exercises for the knee and ankle, along with toe flexion. Non-weight-bearing walking was recommended for 3–4 weeks, followed by a gradual transition to weight-bearing. Regular follow-up visits were conducted to assess bone union and functional outcomes.
Statistical analyses
Data are presented as n prevalence, mean ± SD or range, and were analysed as simple descriptive statistics using IBM SPSS Statistics software, version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Between December 2020 and August 2023, five patients were treated for nonunion of the distal one-fourth of the tibia and were included in the study, comprising four male patients and one female, with a mean age of 42.0 ± 12.9 years (range, 29–63 years). Causes of injury included road traffic accidents (three patients), fall from height (one patient), and crush injury (one patient). Fractures were classified using the AO Foundation/Orthopaedic Trauma Association (AO/OTA) system 2018: one as type 43A1, two as type 43A2, and two as type 43A3. Of these cases, three were closed fractures, while two were open fractures (one Gustilo type II and one Gustilo type IIIA).
In terms of prior surgeries, three patients with closed fractures had been treated with plates; one patient with a Gustilo type II open fracture had an external fixator; and one patient with a Gustilo type IIIA open fracture had a plate followed by an external fixator. The cohort included one patient with atrophic nonunion, three with hypertrophic nonunion, and one with infected nonunion, with a mean nonunion duration of 14.8 ± 2.3 months (range, 12–18 months). Clinical parameters are summarised in Table 1, while Table 2 shows nonunion risk factors for the study cohort, including body mass index, tobacco use, nonsteroidal anti-inflammatory drug use, opioid use, infection history, and diabetes. 13 The patient with a history of infection had been free of symptoms for at least 6 months before revision surgery. Clinical and blood tests were performed in all patients to rule out active infection before RTN treatment.
Demographic and clinical parameters of the study population.

AO/OTA, AO Foundation/Orthopaedic Trauma Association system 2018; Gustilo, Gustilo open fracture classification system.
Related risk factors for nonunion in the study population.

BMI, body mass index (using diagnostic criteria for obesity in BMI for Asian populations recommended by the World Health Organisation, BMI was grouped into four categories: underweight [<18.5 kg/m2], normal weight [18.5–23.0 kg/m2], overweight [23.0–27.5 kg/m2], and obese [≥27.5 kg/m2]); NSAID, nonsteroidal anti-inflammatory drugs.
The mean duration of surgery was 94.0 ± 13.7 min (range, 75–110 min), with hospital stays ranging 7–12 days (mean, 9.8 ± 1.9 days). Patients were followed for 10–18 months, with a mean follow-up of 12.8 ± 3.1 months. Complete bone healing occurred within a mean of 4.8 months. The latest follow-up showed a mean American Orthopedic Foot and Ankle Society (AOFAS) score of 84.4 ± 6.8 (range, 77–95), indicating positive outcomes. No complications, such as infection, reoperation, implant issues, rotational deformity, or shortening, were observed. Surgical data and outcomes are summarised in Table 3, with a representative case illustrated in Figures 2, 3 and 4 (Case 5).
Outcomes following retrograde tibial intramedullary nail to treat distal tibial nonunion in the study population.

AOFAS, American Orthopedic Foot and Ankle Society.

Representative radiography images from a 36-year-old female with a Gustilo type IIIA open distal tibial fracture (Case 5), showing: (a and b) preoperative images; (c and d) immediate debridement, suturing, temporary external fixation and K wires, applied on the day of admission; (e and f) at 11 days after the first operation, gastrocnemius flap was performed for wound coverage and plate was used as a substitute for external fixation; and (g and h) no obvious callus formation at 3 months after the plate fixation.

Representative images from a 36-year-old female with a Gustilo type IIIA open distal tibial fracture (Case 5), with nonunion in the distal tibia at 1 year after the plate fixation, showing: (a and b) preoperative radiography before the revision surgery; (c and d) preoperative computed tomography image indicating hypertrophic nonunion and apex posterior angle in the distal one-fourth of the tibia; and (e and f) anterolateral and medial appearance of the surgical area before revision surgery.
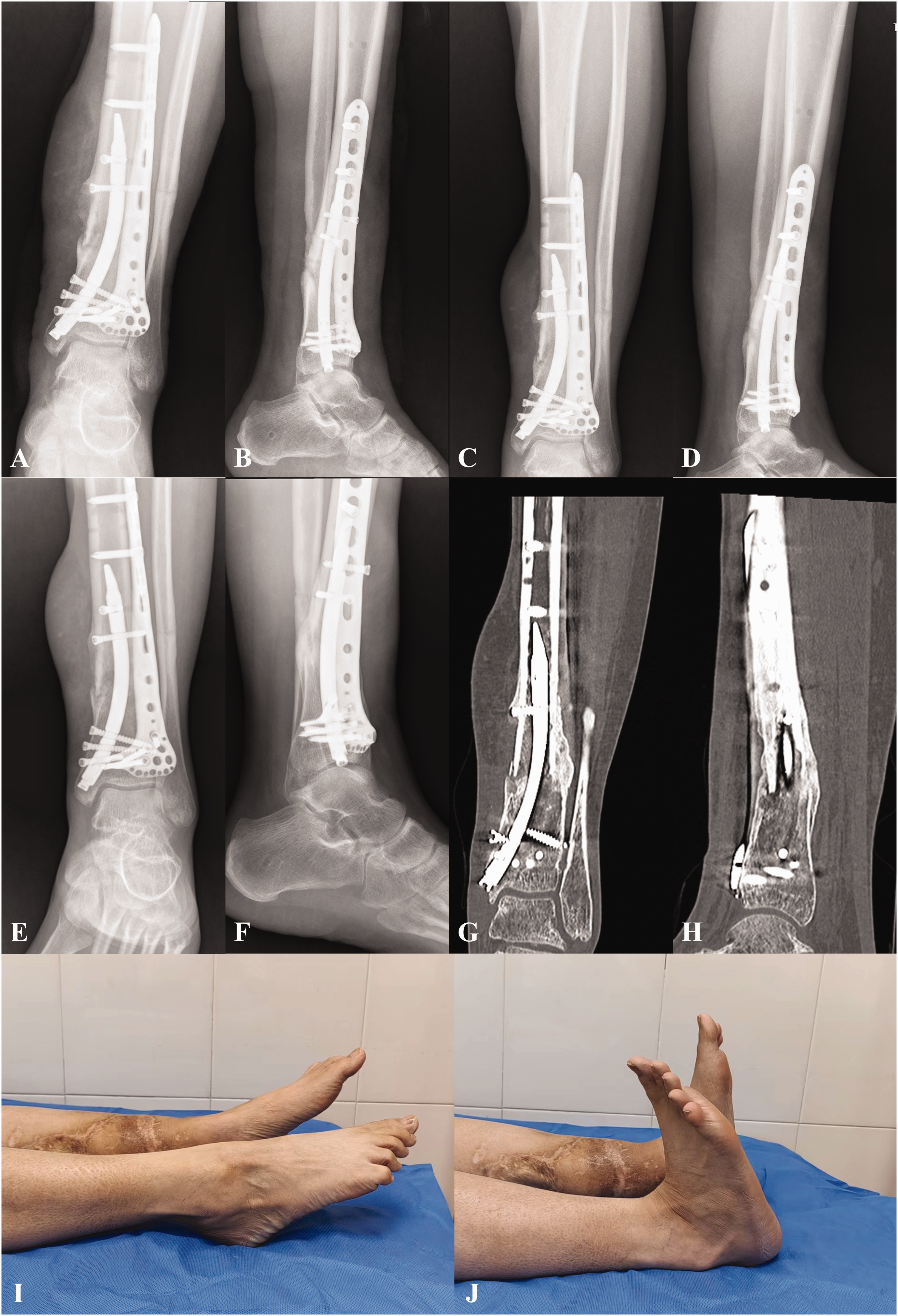
Representative images from a 36-year-old female with a Gustilo type IIIA open distal tibial fracture (Case 5), at 5 months after the RTN treatment, showing bone union: (a and b) radiography image obtained at 3 days after revision surgery; (c and d) radiography image obtained at 3 months after revision surgery; (e–h) X-ray and computed tomography images obtained at 5 months after revision surgery, showing fracture union but no postoperative change in the preoperative apex posterior angle; and (i and j) expected limitations in ankle motion, but no other observed symptoms or complications during follow-up.
Discussion
Nonunion is a rare complication following fractures of the distal one-fourth of the tibia; however, open fractures in this area with compromised soft tissues heighten the risk of infection and nonunion. 14 These complications may result in adverse clinical outcomes, such as persistent local infection, osteomyelitis, localized pain, joint stiffness, and limb deformity, presenting significant challenges in orthopaedic surgery.
High-energy injuries causing open fractures of the distal tibia often require temporary external fixation to stabilize the fracture site, maintain tibial length and alignment, and improve soft tissue conditions for subsequent procedures. 15 Unilateral external fixation, ring external fixation, or Illizarov external fixation have become popular for treating nonunion of the distal tibia, particularly in cases complicated by infection. 16 However, unilateral external fixation may lack sufficient stability, while ring or Illizarov systems might be cumbersome and uncomfortable for patients. Additionally, these methods are associated with prolonged application times and a high incidence of complications, such as pin tract infections, deep soft tissue infections, and even osteomyelitis, limiting their efficacy in managing distal tibial nonunion. 17
Plate fixation is commonly preferred for addressing nonunion in the distal tibia due to its ability to achieve anatomical reduction and maintain stable alignment. In one study involving 11 patients with nonunion of the distal tibial metaphysis, blade plates were applied to the medial tibia via a posteromedial approach, with some patients receiving autologous bone grafts to fill bone defects, resulting in high rates of bone union and low complication rates. 18 Another study, involving nine patients with distal tibial nonunion, utilized contralateral anterior L-shaped locking compression plates inserted through a posterior-lateral approach, achieving a mean AOFAS score of 90 at final follow-up with favourable clinical outcomes. 10 Nonetheless, achieving a balance between mechanical stability and preserving the delicate soft tissue envelope remains critical. Most cases of distal tibial fractures involve high-energy trauma, leading to compromised soft tissues that complicate exposure and adequate bone grafting. Consequently, wound-related complications and deep infections are common during plate fixation procedures for distal tibial nonunion. Furthermore, excessive bone manipulation during open surgeries can perpetuate nonunion. 11
Given the delicate nature of soft tissue in the distal tibia, intramedullary nail fixation emerges as the preferred method for managing distal tibial nonunion. 19 This approach offers several advantages. First, it minimizes soft tissue irritation due to its minimally invasive nature. Secondly, the reaming process not only clears fibrous tissue from the nonunion site but also stimulates new bone formation, reactivating the crucial inflammatory cascade necessary for bone healing. 20 However, intramedullary nail fixation may not be universally suitable for all cases of distal tibial nonunion, especially in cases involving the short, osteopenic, and spacious distal one-fourth segment. Challenges with alignment and instability at the nonunion site may persist, potentially leading to ongoing nonunion or malunion. Therefore, managing nonunion in the distal one-fourth of the tibia remains a significant challenge for orthopaedic surgeons. Bone callus accelerator and foot loading have been associated with a good outcome in cases of nonunion in the distal tibia,21–23 however, further research is needed to confirm these results.
Retrograde tibial intramedullary nail represents an innovative approach to minimally invasive treatment for distal tibial fractures. 24 Initial trials with a small cohort of nine patients reported a 100% success rate based on AOFAS scores, 25 indicating promising outcomes. Compared with plates and antegrade intramedullary nails, RTN demonstrates superior biomechanical characteristics.26,27 However, there are limited reports on its clinical application in managing nonunion of the distal one-fourth of the tibia. In the present study, five patients with nonunion in this area underwent RTN treatment. Early weightbearing and physical therapy were initiated, resulting in successful union in all cases without any instances of infection, reoperation, implant failure, or removal. Notably, case 5, which involved a patient with prior external fixation and plating, showed no change in the preoperative apex posterior angle postoperatively. Despite expected limitations in ankle motion, no other symptoms or complications were observed during follow-up.
Based on a review of literature and clinical experience, the RTN method offers substantial advantages; It is particularly effective for treating nonunion near the tibial plafond, reduces intraoperative fluoroscopy, and supports earlier full weight-bearing. These benefits stem from two key factors. First, RTN's medial ankle entry enhances stability by minimizing the working length and optimizing nail fit in the medullary canal, addressing potential instability and prolonged healing seen with antegrade intramedullary nails. 28 Biomechanically, RTN shows superior resistance to rotation and improved axial stability compared with both antegrade intramedullary nails and plate fixation. 25 Secondly, RTN requires fewer intraoperative fluoroscopy checks due to its precise nail targeting and shorter length, enabling precise initial placement and reducing radiation exposure and surgery time.
When assessing RTN for distal one-fourth tibial nonunion, several considerations arise: (1) length limitations of RTN may restrict its use for mid and lower tibial nonunion; (2) insertion at the medial malleolus with RTN may pose challenges in paediatric patients with open growth plates or conditions affecting the skin over the medial malleolus; and (3) careful handling during RTN insertion is crucial to safeguard the medial malleolus and triangular ligament from injury.
Conclusion
Treating nonunion in the distal one-fourth of the tibia requires a personalized approach, considering compromised soft tissue, impaired vascularity, and mechanical factors. The present findings indicate that RTN may effectively reduce complications, hasten union, and facilitate quicker recovery of functional abilities. However, the present retrospective study design introduces concerns regarding potential selection biases due to its limited sample size and short follow-up duration. Future research should aim to address these limitations through rigorous prospective comparative studies to validate and expand upon these results.
Footnotes
Acknowledgement
We thank all participants in this study for their enthusiasm, tireless work, and sustained support.
Author contributions
Wen-Liang Zhai: article writing, data collection and analysis; Yuan-Fei Xiong: data collection; Hui Liu: article writing, data collection and analysis; Jin-Hui Zhang and Wei-Zhen Xu: literature search and data analysis; Jin Wu: data collection, performed surgeries, research team manager. All authors contributed significantly to the study and manuscript, and have agreed to the final manuscript version.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.