
Abstract
Objective
Obesity can contribute to infertility, but the exact relationship between infertility risk and obesity-related measurements like waist-to-height ratio (WHtR), body roundness index (BRI), conicity index (CoI), and A body shape index (ABSI) in women is uncertain. We investigated the association between these indices and female infertility.
Methods
In this cross-sectional study, we used National Health and Nutrition Examination Survey data (2013–2018). We used weighted multivariable logistic regression analysis, receiver operating characteristic (ROC) curves, and subgroup analysis, as well as propensity score matching.
Results
Among 3373 participants, 344 (10.2%) reported infertility. A significant link between higher infertility risk and increased WHtR, BRI, CoI, ABSI, and body mass index (BMI) was found. Multivariable logistic regression analysis showed WHtR (odds ratio [OR] = 1.27, 95% confidence interval [CI]: 1.14–1.42), BRI (OR = 1.09, 95% CI: 1.05–1.14), CoI (OR = 1.36, 95% CI: 1.18–1.56), ABSI (OR = 1.22, 95% CI: 1.12–1.33), and BMI (OR = 1.03, 95% CI: 1.02–1.05) were significantly associated with female infertility. CoI had the best diagnostic performance (area under the ROC curve 0.628, 95% CI: 0.597–0.658).
Conclusions
Obesity-related indices were positively linked to infertility risk among women in the United States. These indices serve as valuable tools for assessing female infertility risk.
Keywords
Introduction
An infertility diagnosis indicates the inability to become pregnant after 12 months of regular and unprotected sexual activity. Approximately 12.7% of women in the United States (US) who are of childbearing age seek infertility treatment annually. 1 Female infertility is caused by several factors, such as disorders of the ovaries, endocrine system, and uterine and tubal systems. 2 Moreover, obesity is an important disruptor of fertility owing to its widespread systemic effects. Obesity has a detrimental impact on fertility mainly by disrupting the hypothalamic–pituitary–ovarian axis. 3 Women with obesity have higher insulin levels, which stimulate ovarian androgen production. Obesity seems to impact the oocyte, the granulosa cells surrounding it in the ovary, and the fluid that surrounds the oocyte. Additionally, overweight women may experience reduced fertility even without ovulation issues.4–6
Over the past 30 years, the prevalence of obesity has steadily increased worldwide. Prior research has used body mass index (BMI) as the most important indicator of obesity and excess weight. 7 A Mendelian randomization analysis including 28,341 women in Norway showed that women with a high BMI were more likely to be infertile. 8 According to research using the National Health and Nutrition Examination Survey (NHANES) database, in a group of 3624 women in the US, there was a 3% greater chance of infertility for each additional unit of BMI with a BMI of ≥19.5 kg/m2. 9 Nevertheless, BMI does not precisely indicate a person’s fat distribution or the difference between fat and muscle weight.
In recent years, researchers have suggested numerous new indicators related to obesity and lipids, with growing evidence indicating a potential link between these indices and female infertility. The waist-to-height ratio (WHtR) is considered the most accurate indicator of cardiovascular risk and mortality because it explicitly assesses abdominal fat in individuals with a low BMI. 10 Thomas introduced the body roundness index (BRI) in 2013 as a novel predictor that can accurately represent body and visceral fat. 11 Another widely used obesity-related index, the conicity index (CoI) indicates adiposity in terms of body weight (BW), body height (BH), and waist circumference (WC). 12 Furthermore, the A body shape index (ABSI) assesses body shape by considering WC, BW, and BH, offering a more comprehensive understanding of the central abdominal fat distribution.13,14
According to the use of these obesity-related indices for the measurement of obesity from different perspectives, few studies have been conducted on the association of these indices with the risk of female infertility. We used NHANES 2013–2018 data to compare the effectiveness of the WHtR, BRI, CoI, and ABSI with that of traditional anthropometric measures like BMI in predicting infertility risk in women.
Methods
Data source
NHANES is a series of studies aiming to evaluate the well-being and dietary habits of both adults and children in the US. The data are used to evaluate nutritional status and its correlation with health promotion and disease prevention according to results of the surveys. NHANES has a crucial role within the National Center for Health Statistics (NCHS), a part of the US Centers for Disease Control and Prevention, which is tasked with generating essential health data for the country. The general public can access NHANES data on a 2-year cycle at https://www.cdc.gov/nchs/nhanes/. Research conducted using NHANES is approved by the NCHS Research Ethics Review Committee. No ethics or administrative approval is required to access the NHANES database.
Study population
In this cross-sectional study, we focused on three NHANES cycles (2013–2014, 2015–2016, and 2017–2018) in which reproductive health surveys were conducted. The NCHS provided Institutional Review Board approval for NHANES 2013–2018 (Protocol #2011-17 and #2018-01; approval date for Protocol # 2018-01, 26 October 2017). Informed consent for the present study was not required as it comprised publicly available NHANES data. The present study was conducted according to the guidelines laid down in the Declaration of Helsinki of 1975, as revised in 2013. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15
Measurement of obesity-related indices
Trained Mobile Examination Center health technicians collected all physical measurements. Participants were asked to remove bulky clothing and shoes. BW, BH, and WC were measured with calibrated equipment according to established protocols (https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/BMX_J.htm). Obesity-related measures such as BMI, WHtR, BRI, CoI, and ABSI were determined using specified equations16–18 (Figure 1).

Calculation of obesity-related indices. BW, body weight; BH, body height; WC, waist circumference; WHtR, waist-to-height ratio; BRI, body roundness index; CoI, conicity index, ABSI, A body shape index; BMI, body mass index.
Demographic characteristics
Demographic characteristics included age, race and ethnicity, education, marital status, the ratio of family income to poverty (PIR), drinking habits, smoking habits, participation in vigorous and moderate physical activity, age at the first menstrual period, history of regular periods in the past year, history of pelvic infection (PID), history of pregnancy, hypertension, and diabetes. All these characteristics were obtained from NHANES demographic information, screening results, questionnaires, and lab tests. Comprehensive measurement protocols can be found at https://www.cdc.gov/nchs/nhanes/.
Statistical analysis
In this study, continuous variables are described using mean and standard deviation and categorical variables are reported using number and percentage. A t-test was used to analyze differences in the mean and standard deviation between groups with and without infertility. The chi-square test was used to compare categorical variables. We used three multifactor logistic regression models to investigate the associations between infertility and obesity-related indices (BMI, WHtR, BRI, CoI, and ABSI). No covariates were adjusted in Model I. Age, race and ethnicity, education, marital status, and PIR were adjusted in Model II. Model III was adjusted for age, race and ethnicity, education, marital status, PIR, drinking, smoking, vigorous physical activity, moderate physical activity, age at first menstrual period, regular periods in the past 12 months, history of PID, history of pregnancy, hypertension, and diabetes. Additionally, the ability of these obesity-related measurements to predict female infertility was evaluated using receiver operating characteristic (ROC) curves. We also performed subgroup analysis based on age, race and ethnicity, and hypertension. Tests for interaction were conducted to determine whether these covariates interacted with obesity-related indices (BMI, WHtR, BRI, CoI, and ABSI) to affect infertility.
To control for potential confounding variables and reduce bias, propensity score matching (PSM) was conducted in this research. A 1:2 PSM analysis with a 0.01 caliper value was performed.19,20 Additionally, similar methods were used to explore the association between obesity-related indices and infertility risk in the population after PSM.
The analysis was performed with R version 4.2 (www.r-project.org) and EmpowerStates 2.0 (X&Y Solutions, Inc. Boston, MA, USA). Statistical significance was considered with a P value of <0.05 in a two-sided analysis.
Results
In the present study, 29,400 participants were enrolled. Initially, 14,452 men and 190 pregnant women were excluded, as well as 5630 female participants younger than age 18 years and 4995 female participants older than age 45 years. Additionally, we excluded women with missing information on self-reported infertility (n = 629), BW (n = 40), BH (n = 3), and WC (n = 88). Finally, 3373 participants were included in the analysis (Figure 2).

Study flowchart. NHANES, National Health and Nutrition Examination Survey; BW, body weight; BH, body height; WC, waist circumference.
Population characteristics
Weighed characteristics of participants aged 18 to 45 years are presented in Table 1, according to their fertility status. In the sample of 3373 individuals, 344 (10.2%) women were infertile, and 3029 (89.8%) were not infertile. Women experiencing infertility typically were older (35.10 ± 7.13 vs. 30.86 ± 8.50 years), more likely to be married or in a relationship (71.80% vs. 48.37%), and had a higher PIR (2.52 ± 1.63 vs. 2.25 ± 1.60). Infertile women were more likely to drink alcohol (11.05% vs. 5.61%) and to smoke (36.05% vs. 25.72%), and were more likely to have hypertension (20.64% vs. 13.30%) or diabetes (8.14% vs. 3.57%). Additionally, our research revealed that women experiencing infertility engaged in less vigorous physical activity (24.13% vs. 32.82%) and a larger proportion had previous pregnancies (84.66% vs. 70.87%) and previous treatment for PID (10.47% vs. 4.13%) (all P < 0.05). There were no statistical differences in terms of race and ethnicity, moderate physical activity, age at first menstrual period, and regular periods in the past 12 months.
Characteristics of non-weighted study participants according to infertility.

Data are presented as mean ± standard deviation (continuous) or number and percent (categorical).
PIR, poverty-income ratio; PID, pelvic infection; BW, body weight; BH, body height; WC, waist circumference; BMI, body mass index; WHtR, waist–height ratio; BRI, body roundness index; CoI, conicity index; ABSI, A body shape index.
Overall, infertile women presented higher BW (84.66 ± 26.09 kg vs. 75.50 ± 22.58 kg), BH (162.38 ± 6.70 cm vs. 161.40 ± 6.85 cm), and WC (102.31 ± 20.30 cm vs. 93.88 ± 18.34 cm) (all P < 0.05). Additionally, obesity-related indices were higher among infertile women compared with fertile participants, including BMI (31.97 ± 9.10 kg/m2 vs. 28.91 ± 8.12 kg/m2), WHtR (0.63 ± 0.12 vs. 0.58 ± 0.11), BRI (6.41 ± 3.05 vs. 5.28 ± 2.69), CoI (1.31 ± 0.09 vs. 1.26 ± 0.09), and ABSI (0.08 ± 0.02 vs. 0.07 ± 0.01) (all P < 0.001).
Associations of infertility risk with WHtR, BRI, CoI, ABSI, and BMI
Table 2 shows the results of our analysis regarding the relationship of female infertility risk with WHtR, BRI, CoI, ABSI, and BMI using multivariate regression, adjusted progressively and in a comparison with the first quartile of obesity-related indices as a reference. A strong connection was found between the five indices and the likelihood of infertility, showing a clear pattern of a higher infertility risk with higher levels of obesity-related indices (P for trend <0.001). After fully adjusting for age, race and ethnicity, education, marital status, PIR, drinking, smoking, vigorous physical activity, moderate physical activity, age at first menstrual period, regular periods in the past 12 months, PID history, pregnancy history, hypertension, and diabetes (Model III), the indices WHtR, BRI, CoI, ABSI, and BMI all showed a significant associations with a higher infertility risk: WHtR (odds ratio [OR] Q4 vs. Q1: 2.16, 95% confidence interval [CI] 1.44–3.23, P = 0.0002, P for trend <0.0001), BRI (OR Q4 vs. Q1: 2.16, 95% CI 1.44–3.23, P = 0.0002, P for trend <0.0001), CoI (OR Q4 vs. Q1: 1.70, 95% CI 1.15–2.51, P = 0.0083, P for trend = 0.0006), ABSI (OR Q4 vs. Q1: 2.16, 95% CI 1.45–3.21, P = 0.0002, P for trend <0.0001), and BMI (OR Q4 vs. Q1: 2.13, 95% CI 1.44–3.13, P = 0.0001, P for trend <0.0001).
Association between obesity-related indices and female infertility.
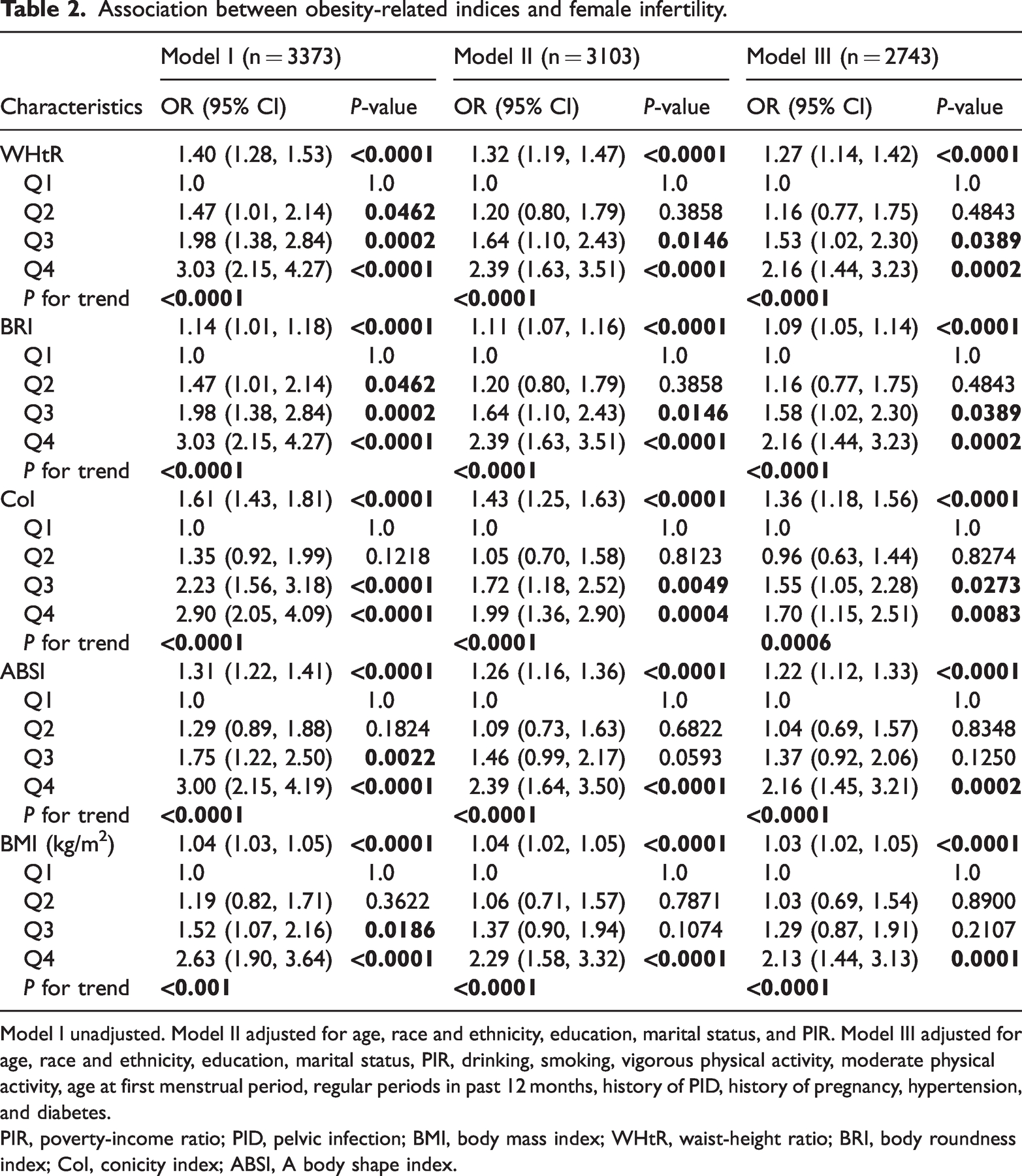
Model I unadjusted. Model II adjusted for age, race and ethnicity, education, marital status, and PIR. Model III adjusted for age, race and ethnicity, education, marital status, PIR, drinking, smoking, vigorous physical activity, moderate physical activity, age at first menstrual period, regular periods in past 12 months, history of PID, history of pregnancy, hypertension, and diabetes.
PIR, poverty-income ratio; PID, pelvic infection; BMI, body mass index; WHtR, waist-height ratio; BRI, body roundness index; CoI, conicity index; ABSI, A body shape index.
Discrimination ability of different obesity-related indices
Various obesity-related indices were evaluated using ROC curves and the area under the ROC curve (AUC) to assess their capacity to distinguish women with infertility (Figure 3). After analyzing the data, we determined that CoI outperformed other indices in terms of diagnostic accuracy, with an AUC of 0.628 (95% CI: 0.597–0.658). The other values were as follows: ABSI (AUC: 0.623, 95% CI: 0.592–0.654), WHtR (AUC: 0.619, 95% CI: 0.588–0.650), BRI (AUC: 0.619, 95% CI: 0.588–0.650), and BMI (AUC: 0.605, 95% CI: 0.573–0.637).

Receiver operating characteristic curve for infertility-related indicators in all participants. WHtR, waist-to-height ratio; BRI, body roundness index; CoI, conicity index, ABSI, A body shape index; BMI, body mass index; ROC, receiver operating characteristic; AUC, area under the ROC curve.
Results of subgroup analysis
Subgroup analysis was performed to examine potential variations in the relationship between the five obesity-related measures and infertility among the different groups, as shown in Table 3 and Supplementary Table S3. All stratifications were controlled for the covariates outlined in Table 1, excluding the variable used for stratification. The data demonstrated that the correlation between CoI and infertility was affected by age (P for interaction = 0.0005). The same result was also found for the four other measures (WHtR, ABSI, BRI, BMI: P for interaction = 0.0088, 0.0060, 0.0203, and 0.0331, respectively). In the subgroup analysis based on race and ethnicity, the correlation was stronger in non-Hispanic Whites among all measure groups (CoI: OR = 1.41, 95% CI: 1.13–1.77, P = 0.0025; WHtR: OR = 1.31, 95% CI: 1.10–1.56, P = 0.0026; ABSI: OR = 1.25, 95% CI: 1.09–1.43, P = 0.0013; BRI: OR = 1.11, 95% CI: 1.03–1.18, P = 0.0031; BMI: OR = 1.03, 95% CI: 1.01–1.06, P = 0.0033). Furthermore, there were no significant interactions, indicating that the relationship between these five measures and infertility depended on hypertension and diabetes. However, the association between these five measures and infertility was more significant in those who did not have hypertension and diabetes (P < 0.05).
Subgroup analysis for the association between obesity-related indices and female infertility.
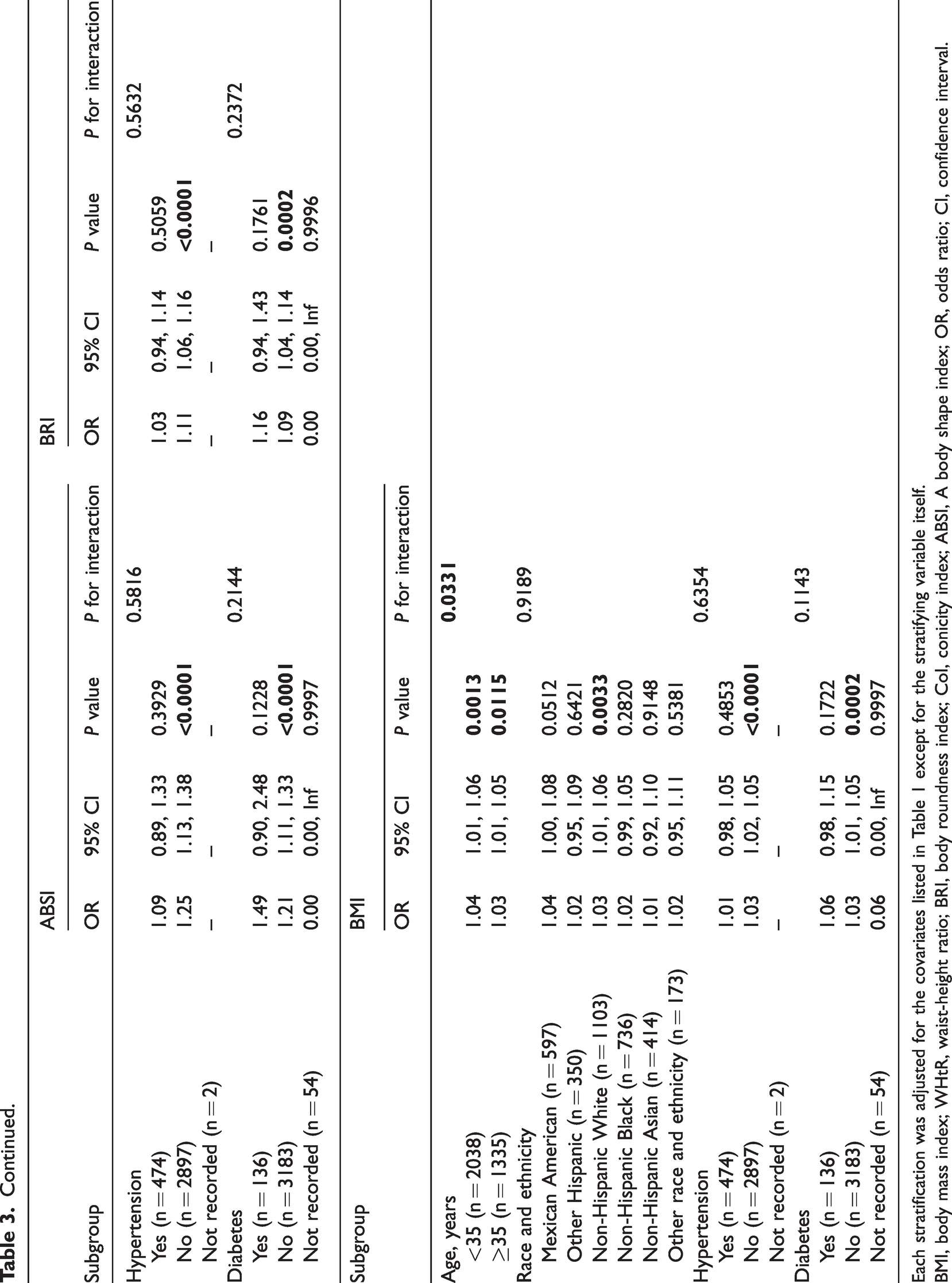
Each stratification was adjusted for the covariates listed in Table 1 except for the stratifying variable itself.
BMI, body mass index; WHtR, waist-height ratio; BRI, body roundness index; CoI, conicity index; ABSI, A body shape index; OR, odds ratio; CI, confidence interval.
PSM analysis
The analysis included 975 participants after PSM, comprising 325 women with infertility and 650 without infertility. As shown in Supplementary Table S1, there were no statistically significant differences between groups based on age, race and ethnicity, education, marital status, PIR, hypertension, diabetes, drinking, smoking, vigorous physical activity, moderate physical activity, age at first menstrual period, regular periods in the past 12 months, and PID history. Supplementary Table S2 demonstrates the results of weighted multivariable logistic regression analysis.
In Model III, WHtR, BRI, CoI, ABSI, and BMI were positively associated with infertility risk. Compared with the Q1 of WHtR, BRI, CoI, ABSI, and BMI, Q4 groups showed higher risks for the occurrence of infertility (all P for trend <0.05). Subgroup analysis showed that CoI and WHtR were significantly associated with the risk of infertility in the group aged ≥35 years. ABSI, BRI, and BMI were significantly associated with the risk of infertility in both age subgroups. In the subgroup of race and ethnicity, the five obesity-related measures were related to infertility risk in non-Hispanic Whites; these results were also observed in women without diabetes (Supplementary Table S3). The ROC curves and AUC are shown in Supplementary Figure S1.
Discussion
Approximately 186 million individuals and 48 million couples worldwide experience infertility, according to the World Health Organization. 21 The causes of infertility are a global public health issue that is poorly understood. The purpose of this study was to identify certain obesity-related factors that may affect infertility in American women of childbearing age between 2013 and 2018. Obesity is a prevalent issue among women of childbearing age. Research indicates that the risk of infertility is higher in women with obesity compared with their non-obese counterparts. Several studies have found that women with obesity often take longer to become pregnant.22,23 The pathophysiology of obesity involves low-grade systemic inflammation driven by pro-inflammatory elements like free fatty acids, lipopolysaccharides, adipokines (leptin, resistin, and visfatin), and cytokines (tumor necrosis factor alpha, interleukin [IL]-1β, IL-6), which are released by adipose tissue.24–26 Additionally, the impact of obesity includes a series of physiological disruptions such as hormonal imbalances, ovulation interference, compromised oocyte quality, embryonic development, and uterine environment alterations.27,28 In general, the adverse effects of obesity on fertility and fecundity are well established. 29
Several body indices have been used to measure obesity. As an important and common index, BMI is a measure of weight adjusted for height, which is associated with infertility status.5,30,31 However, BMI does not separate body fat from lean mass and it has limited sensitivity, making this measure problematic for clinical purposes. WC is a simple anthropometric measurement linked to fat mass and has been suggested as a method for identifying central obesity. 32 WC also has a positive association with infertility.33,34 Our previous studies have shown that the weight-adjusted waist index, which includes WC as a measure, is positively associated with infertility risk. 31 In this study, WC was also used in the calculation of the other four indicators (WHtR, BRI, CoI, and ABSI). The four indices showed greater sensitivity in predicting infertility risk than BMI alone. Our study is the first to discuss these five obesity indices and the risk of female infertility. Our results demonstrate the potential of obesity-related indices as predictors of infertility risk in women. Furthermore, the fully adjusted multivariate regression analysis demonstrated a trend of increasing infertility risk with increases in these five obesity-related indices.
Compared with other indices, CoI had the best diagnostic ability for female infertility based on ROC curve analysis. The CoI determines whether an individual has a double cone or a cylinder shape, depending on the amount of fat accumulated around the abdomen. 35 However, the ABSI showed the best diagnostic capability after PSM, possibly because PSM eliminated the effect of age. Similar to WC and the waist-to-hip ratio, WHtR is used to describe abdominal adiposity. This index has a strong positive association with cardiovascular disease risk among people with and without diabetes who have a normal BMI.36,37 In this study, we also found that the WHtR was positively related to infertility risk. In addition to predicting cardiovascular disease and all-cause mortality, another index, the ABSI, can also be used as a proxy for detecting sarcopenic obesity.13,38,39 This index can be used to estimate and stratify risk with BMI as a complement. The recently created BRI reduces the impact of BMI to some degree and offers a more precise representation of body fat than conventional indices like BMI and WC. A key aspect of the BRI is a focus on natural central obesity, which is not solely determined by body weight.40,41 The BRI emphasizes the importance of addressing visceral fat, which is not solely based on body mass. Using BRI as an indicator for assessing infertility risk in daily clinical practice is encouraged in this study.
The results of subgroup analysis showed that age may interact with the WHtR, CoI, ABSI, BRI, and BMI. According to our study, the connection between CoI and infertility disappeared in women who were aged 35 years or older. Previous studies have indicated that a decrease in the generation of robust and high-grade oocytes owing to aging leads to diminished fertility in women over age 35 years.42,43 However, when referring to the four other indices, the connection existed in all age groups. Consistent with our findings, non-Hispanic Whites are more sensitive to infertility because they are more susceptible to vitamin D deficiency, which leads to abdominal obesity.44,45 Furthermore, women with hypertension or diabetes show weaker links between infertility and these five indices compared with women without those conditions. These results may be owing to the fact that not all women with hypertension or diabetes are adequately treated, and some medications may affect ovulation.46,47
In addition to peripheral obesity, there has been increasing attention in recent years on the relationship between visceral obesity and infertility. A recently published article by Zhou et al. 47 presents an analysis focusing on the visceral adipose tissue area (VATA) and its association with female infertility, using the NHANES database. Zhou’s study expands our understanding of visceral obesity and provides new methods for predicting the risk of and finding treatments for female infertility in clinical settings. In the future, BMI, WHtR, BRI, CoI, ABSI, and VATA may be used together to assess women's infertility risk. Using these indicators, a scoring system can be developed to enhance the accuracy and comprehensiveness of prediction.
Strengths and limitations
In this study, we investigated indices related to obesity that may be used to predict female infertility. Our research showed that WHtR, BRI, CoI, and ABSI all had a positive relationship with the risk of infertility. Furthermore, compared with the classical BMI, these obesity-related indices showed greater sensitivity, suggesting that these may be used to measure infertility in future studies. However, it is crucial to acknowledge certain limitations in this research. First, the NHANES database records infertility as self-reported in a questionnaire but does not include concrete details about the reasons for infertility. Second, these indices were not combined in our study to determine their ability to screen infertility risk. In future clinical research, extensive multicenter prospective studies are needed to confirm our results.
Conclusion
The present study demonstrated a positive correlation between obesity-related indices and female infertility risk in the United States. Additional larger prospective studies are essential to substantiate these results.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251315019 - Supplemental material for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey
Supplemental material, sj-pdf-1-imr-10.1177_03000605251315019 for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey by Hong Zhang, Minmin Yu, Li Li, Chen Chen and Qinyuan He in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605251315019 - Supplemental material for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey
Supplemental material, sj-pdf-2-imr-10.1177_03000605251315019 for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey by Hong Zhang, Minmin Yu, Li Li, Chen Chen and Qinyuan He in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605251315019 - Supplemental material for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey
Supplemental material, sj-pdf-3-imr-10.1177_03000605251315019 for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey by Hong Zhang, Minmin Yu, Li Li, Chen Chen and Qinyuan He in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605251315019 - Supplemental material for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey
Supplemental material, sj-pdf-4-imr-10.1177_03000605251315019 for Obesity-related indices are associated with self-reported infertility in women: findings from the National Health and Nutrition Examination Survey by Hong Zhang, Minmin Yu, Li Li, Chen Chen and Qinyuan He in Journal of International Medical Research
Footnotes
Acknowledgements
We thank the National Health and Nutrition Examination Surveys for providing the data. We appreciate all participants who contributed to this study.
Author contributions
Hong Zhang and Qinyuan He conducted the analyses and wrote the draft of the article. Minmin Yu, Li Li, and Chen Chen conceived the study design. All authors contributed to the collection of clinical data, writing or revising of the manuscript, and approved the final manuscript version.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.