
Abstract
Cytomegalovirus (CMV) infection typically affects immunocompromised individuals. However, CMV-associated enteritis involving the entire small intestine is rare in immunocompetent patients. We report a case of a 60-year-old immunocompetent woman with a history of diabetes mellitus who presented with diarrhea for 3 weeks. Abdominal computed tomography and stool tests revealed panenteritis accompanied by protein-losing enteropathy. Enteroscopy revealed ulcerative mucosa throughout the small intestine, and subsequent biopsies confirmed CMV-associated enteritis. Initial treatment with intravenous ganciclovir was complicated by pancytopenia, leading to its discontinuation and a switch to oral valganciclovir. This adjustment led to significant clinical improvement and symptom resolution. This case highlights the importance of considering CMV-associated enteritis in immunocompetent patients presenting with unexplained gastrointestinal symptoms and demonstrates the effectiveness of oral valganciclovir following ganciclovir-induced pancytopenia.
Introduction
Cytomegalovirus (CMV), a member of the herpesvirus family, causes significant morbidity in individuals with immunocompromised states, such as those with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), those undergoing organ transplantation, those with hematologic malignancies, and those undergoing chemotherapy or long-term corticosteroid therapy. 1 CMV can affect any part of the gastrointestinal (GI) tract, leading to a wide range of symptoms, from mild, self-limiting illness to severe, life-threatening conditions. However, CMV infection involving the GI tract is uncommon in immunocompetent individuals. The exact incidence of CMV-related GI involvement in immunocompetent individuals is not well established. However, the condition remains rare, and it might be underdiagnosed because of its nonspecific presentation. When CMV infection does occur in immunocompetent individuals, the clinical presentation often includes diarrhea, abdominal pain, and occasional bleeding. 2 Diagnosing CMV enteritis in these patients can be challenging, as symptoms can overlap with those of other gastrointestinal disorders such as bacterial enteritis, inflammatory bowel disease, or ischemic colitis. Therefore, histopathological confirmation using hematoxylin and eosin staining and immunohistochemistry is essential for diagnosis. Treatment primarily involves antiviral therapy, typically with ganciclovir or valganciclovir, although the potential for adverse effects, such as myelosuppression, requires careful monitoring.3,4 In this study, we report a case of CMV-associated panenteritis in a 60-year-old immunocompetent woman that was successfully treated with oral valganciclovir, emphasizing the importance of considering CMV infection in the differential diagnosis of chronic diarrhea even in patients without apparent immunosuppression.
Case report
The reporting of this study conforms to CARE guidelines. 5 A woman in her 60s with well-controlled type 2 diabetes mellitus (HbA1c = 6.5%) on metformin presented to the emergency department with a 3-week history of watery diarrhea, low-grade fever, nausea, and vomiting. Her vital signs were as follows: blood pressure, 90/60 mmHg; heart rate, 100 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 37.8°C. Laboratory tests revealed a white blood cell (WBC) count of 10,780/μL, hemoglobin (Hb) level of 10.8 g/dL, platelet (PLT) count of 293,000/μL, C-reactive protein level of 3.67 mg/dL, serum albumin level of 2.14 g/dL, sodium level of 146 mmol/L, and potassium level of 3.3 mmol/L. The results of liver and kidney function tests were within normal limits. Stool tests identified fecal calprotectin >1000 μg/g, and Clostridioides difficile toxin testing was negative. Alpha-1-antitrypsin clearance was 180 mL/24 hours, indicating protein-losing enteropathy. Abdominal computed tomography (CT) revealed diffuse wall thickening and mucosal enhancement throughout the small intestine, consistent with panenteritis (Figure 1). Empirical antibiotic treatment with intravenous ciprofloxacin and metronidazole was initiated, covering potential bacterial infections such as enteropathogenic Escherichia coli or Clostridium species. Because of the persistent symptoms of watery diarrhea, nausea, and vomiting, the patient was initially limited to small amounts of fluids, and solid food intake was restricted. However, after 5 days of treatment, the patient’s symptoms persisted. Further investigation with enteroscopy revealed diffuse, hyperemic, and ulcerative mucosa in the jejunum and ileum (Figure 2). Biopsy samples were taken from both the jejunum and ileum, and histopathological examination revealed ulcerative changes with inflammatory cell infiltration in both areas, along with characteristic owl’s eye inclusions, indicating CMV infection. CMV immunohistochemistry further confirmed the diagnosis by highlighting CMV-infected cells, which appeared as dark brown-stained cells, consistent with CMV-associated enteritis in both the jejunum and ileum (Figure 3). Following the diagnosis, empirical antibiotics were administered for 7 days, after which intravenous ganciclovir 5 mg/kg (300 mg for a 60 kg patient) every 12 hours was initiated. After 3 days of treatment, the patient developed pancytopenia (WBCs, 3210/μL; Hb, 8.4 g/dL; PLTs, 62,000/μL). A 75% dose reduction of ganciclovir was attempted to mitigate the hematologic side effects, but the pancytopenia persisted. Because of this complication, the antiviral regimen was switched to oral valganciclovir 900 mg every 12 hours. Following this change, the patient’s pancytopenia gradually improved, and her symptoms resolved. The patient resumed oral intake on the 10th day of hospitalization following clinical improvement in abdominal symptoms and stabilization of laboratory markers, specifically the WBC count and serum albumin level. The patient was discharged after 1 week of oral therapy, and oral valganciclovir was continued for an additional 2 weeks as an outpatient, completing 3 weeks of treatment. One month after completing antiviral therapy, follow-up abdominal CT and enteroscopy revealed significant improvement with no evidence of active disease. The patient remained symptom-free at her 3-month follow-up, and she has not experienced a recurrence of symptoms.

Coronal views of the abdominal computed tomography image demonstrating diffuse wall thickening and mucosal enhancement throughout the entire small intestine, consistent with panenteritis.
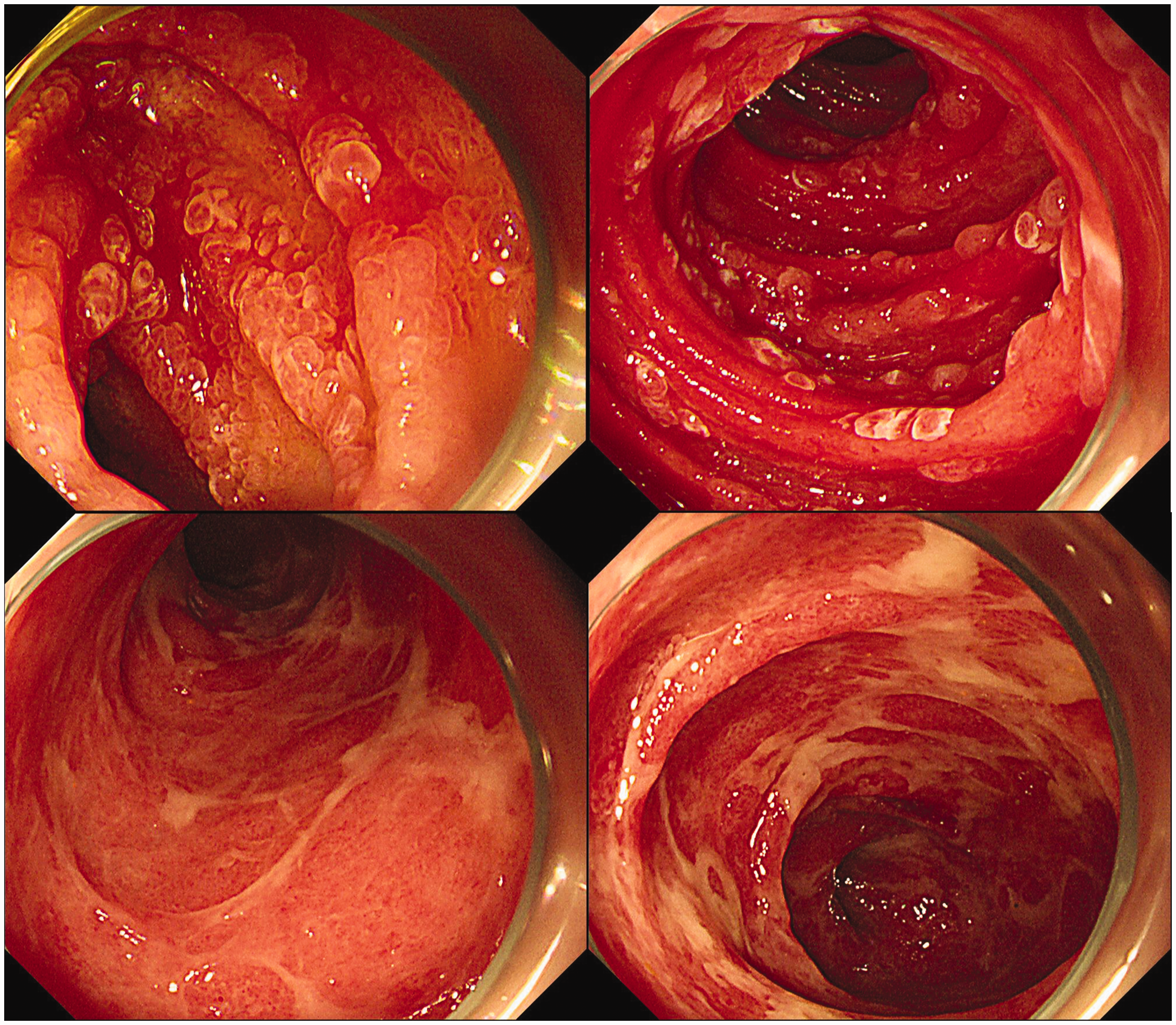
Enteroscopic images of the small intestine. The upper two images depict the jejunum, revealing diffuse hyperemic, edematous, and friable erosive mucosa with easy contact bleeding. The lower two images depict the ileum, revealing diffuse hyperemia and a significant amount of exudate. These findings are consistent with severe inflammatory changes throughout the small intestine.

The upper image at ×20 magnification presents hematoxylin and eosin staining of the mucosa, revealing ulcerative changes and infiltration of numerous inflammatory cells. The yellow arrows indicate owl’s eye inclusions, which are cytopathic changes characteristic of CMV infection. The lower image at ×10 magnification presents the results of immunohistochemistry for CMV, highlighting CMV-infected cells as dark brown as dark brown stained cells. CMV, cytomegalovirus.
The patient provided written informed consent and agreed to the use of her medical records and images for publication of this case report. The patient’s details were de-identified. Approval by an ethics committee was not required because all data used in this study were obtained from previous medical records.
Discussion
CMV infection primarily affects immunocompromised individuals, such as those with HIV/AIDS, transplant recipients, and patients undergoing chemotherapy or long-term corticosteroid therapy. 1 In immunocompetent individuals, CMV infections are uncommon, and they can pose significant diagnostic and therapeutic challenges because of their atypical presentation. 2
This case of CMV-associated panenteritis in a 60-year-old immunocompetent woman highlights several important aspects of the disease’s presentation, diagnosis, and management. The patient presented with chronic diarrhea, fever, and nausea, which are symptoms commonly associated with a wide range of gastrointestinal pathologies, making the diagnosis initially challenging. Given the patient’s nonspecific presentation and the high prevalence of enteric pathogens, empirical antibiotic treatment was initiated to cover potential bacterial infections, such as enteropathogenic E. coli or Clostridium species. However, the lack of response to antibiotics and the persistence of symptoms necessitated further investigation, leading to the diagnosis of CMV-associated enteritis. 2
Although gastrointestinal CMV infections can involve any part of the GI tract, small bowel involvement presenting as panenteritis is particularly unusual in immunocompetent patients. The presence of protein-losing enteropathy, as indicated by elevated alpha-1-antitrypsin clearance, further complicated the clinical scenario, and it is a rare but recognized complication of severe CMV enteritis. 6 Initial investigations, including comprehensive stool analysis and imaging studies, were essential in identifying the condition. Elevated fecal calprotectin levels indicated significant intestinal inflammation, whereas abdominal CT findings were suggestive of panenteritis. Enteroscopy permitted direct visualization of the intestinal mucosa, revealing diffuse, hyperemic, and friable ulcerative changes. Histopathological examination and immunohistochemical staining are critical for diagnosing CMV enteritis, as the endoscopic findings are often nonspecific. In this case, CMV-associated enteritis was confirmed through the identification of characteristic inclusion bodies and positive immunohistochemistry for CMV. This multi-modal diagnostic approach is crucial for ensuring accurate diagnosis, particularly in atypical presentations like such as the present case.
Antiviral therapy with ganciclovir is the first-line treatment for CMV infections, but it carries a significant risk of hematologic toxicity, as demonstrated by the development of pancytopenia in this patient.3,4 The 75% reduction of the ganciclovir dosage was a reasonable attempt to mitigate these hematologic side effects,7,8 but the persistence of pancytopenia necessitated a switch to oral valganciclovir. Valganciclovir, an oral prodrug of ganciclovir, has similar efficacy as intravenous ganciclovir, and it is often better tolerated, making it a suitable alternative in managing CMV infections. Studies illustrated that oral valganciclovir achieves comparable plasma concentrations as intravenous ganciclovir, ensuring effective viral suppression while offering greater convenience and potentially fewer side effects for patients.9–11 Additionally, the oral formulation reduces the need for prolonged intravenous access, thereby decreasing the risk of catheter-related complications and improving patient compliance. 12 The patient’s gradual improvement of pancytopenia and resolution of gastrointestinal symptoms following the switch to oral therapy underscore the importance of individualized treatment adjustments based on patient response and tolerance.
A review of the literature revealed that CMV enteritis in immunocompetent patients, although rare, is increasingly recognized.13–16 Previous case reports and studies highlighted the variability in clinical presentation and the need for high clinical suspicion and comprehensive diagnostic workup in such cases. The successful management of CMV enteritis with valganciclovir in this case is consistent with existing reports, 16 which advocate for the use of oral antiviral agents in cases in which intravenous administration is not feasible or is associated with significant side effects.
This case report illustrated the complexities of diagnosing and managing CMV-associated panenteritis in an immunocompetent patient. It highlighted the importance of considering CMV in the differential diagnosis of chronic diarrhea and the need for a thorough diagnostic approach, including endoscopic and histopathological evaluation. The effective use of oral valganciclovir following complications with intravenous ganciclovir demonstrates the adaptability required in treatment regimens to ensure patient safety and therapeutic efficacy. This case contributes to the growing body of literature on CMV infections in immunocompetent individuals and provides valuable insights for clinical practice.
Footnotes
Acknowledgements
We are grateful to the patient and all of the medical staff involved in the management of this case. Special thanks are given to the physicians and technicians who contributed to the diagnosis and treatment.
Author’s contributions
Kye Whon Kim and Min Cheol Kim conceptualized and designed the study. Kye Whon Kim prepared the initial draft, and Min Cheol Kim critically revised the manuscript. Both authors reviewed and approved the final version, and both authors take full responsibility for all aspects of the work.
Data availability statement
Data are available upon reasonable request from the corresponding author.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Yeungnam University Research Fund in 2021.