
Abstract
Brain abscesses caused by Mycobacterium tuberculosis are rarely reported and are typically found in immunocompromised patients. The challenges in identifying the pathogen and the frequent delays in initiating appropriate therapy often result in a poor prognosis for patients. We herein report a rare case of a brain abscess caused by M. tuberculosis in a 63-year-old patient with a history of hypertension but no history of pulmonary tuberculosis. The patient was hospitalized twice because of worsening right upper limb weakness and speech difficulties. Both a pus culture and cerebrospinal fluid culture were negative. Ultimately, the diagnosis of M. tuberculosis infection was confirmed through next-generation sequencing and the tuberculosis-specific T-cell test (T-SPOT). The patient’s symptoms improved following anti-tuberculosis treatment. This case highlights the importance of considering M. tuberculosis as a potential cause of brain abscesses, even in immunocompetent individuals, and underscores the need for early diagnosis for effective treatment.
Keywords
Introduction
Central nervous system (CNS) tuberculosis accounts for approximately 1% of all tuberculosis infections and is the most lethal form of the disease, leading to death or neurological complications in over 50% of cases. 1 China is among the 30 countries with a high tuberculosis burden, accounting for 8.4% of global tuberculosis cases and contributing significantly to mortality. 2 Risk factors for CNS tuberculosis include concomitant malignancy, malnutrition, human immunodeficiency virus (HIV) infection, and the use of immunosuppressive drugs. 3 CNS tuberculosis encompasses several forms, including meningeal tuberculosis, intracranial tuberculoma, tuberculous abscess, and spinal cord tuberculosis, with tuberculous meningitis and tuberculomas being the most common types. 4 However, brain abscesses caused by Mycobacterium tuberculosis are rarely reported.5,6 Timely identification of the pathogen is crucial for the effective treatment and prognosis of patients with brain abscesses.
In this report, we present a case of a brain abscess caused by M. tuberculosis in an immunocompetent patient with no history of pulmonary tuberculosis. The patient was hospitalized twice because of worsening right upper limb weakness and speech difficulties. This case underscores the importance of early diagnosis of tuberculous brain abscess in immunocompetent individuals without prior tuberculosis or a contact history.
Case presentation
A 63-year-old woman presented with a >1-month history of numbness and weakness in the right palm, which had worsened over the past week. The patient denied experiencing fever, dizziness, headache, slurred speech, facial asymmetry, or a history of trauma. Her medical history included hypertension, but she had no relevant travel or contact history. The patient did not smoke, consume alcohol, or use recreational drugs, and she reported no food or drug allergies.
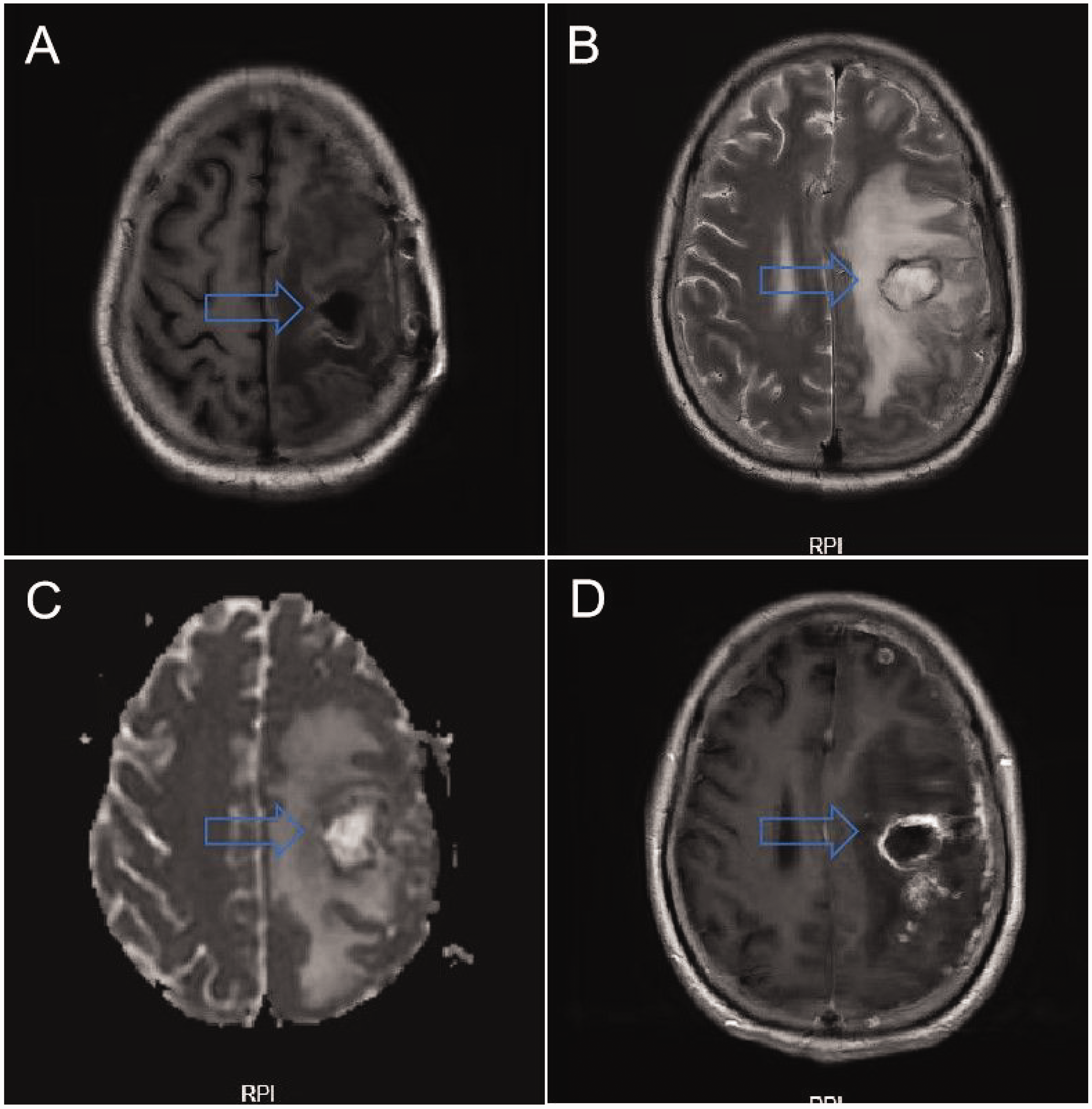
On admission (Day 0), her physical examination was unremarkable, with normal cardiac and pulmonary auscultation. Muscle strength was graded as follows: distal right upper extremity, 0/5; proximal right upper extremity, 2/5; right lower extremity, 5−/5; and left extremities, 5/5. She exhibited decreased sensation to pinprick and touch in the right palm. Reflexes in both upper and lower extremities were normal, and no neck stiffness was observed. Babinski’s reflex was positive on the right side and negative on the left. Laboratory test results were within normal limits. Chest computed tomography revealed scattered fibroproliferative foci in both lungs, which did not require specific treatment. Brain magnetic resonance imaging (MRI) indicated a lesion in the left frontal lobe with significant surrounding edema (Figure 1), leading to a diagnosis of brain abscess based on clinical history and imaging findings.

Magnetic resonance imaging (axial view) of the patient at the first admission. The post-contrast gadolinium (a) T2WI, (b) T1WI, (c) DWI, and (d) T2 post-contrast image revealed a nodule-like abnormal signal focus in the left frontal lobe, with mixed high and low signals on T2WI, an isointense signal on T1WI, a localized increased signal on DWI, and an isointense signal on the black water sequence. The lesion measured approximately 15 × 21 mm and showed extensive surrounding edema. T1WI, T1-weighted imaging; T2WI, T2-weighted imaging; DWI, diffusion-weighted imaging.
Mannitol (100 mL every 6 hours, intravenous infusion) was administered to reduce intracranial pressure, and sodium valproate and levetiracetam were prescribed to prevent seizures. A craniotomy was performed on day 5 to drain the left frontal lobe abscess. Postoperatively, methylprednisolone (40 mg once daily, intravenous infusion) was administered for 1 week for anti-inflammatory treatment. Upon drainage, the abscess cavity walls appeared tough, mechanized, and yellowish-white. Pathological analysis of the abscess walls indicated an accumulation of neutrophils near the brain tissue. The final pathology report confirmed inflammatory necrosis, neutrophil infiltration, and glial cell hyperplasia, consistent with a brain abscess (Figure 2). The pus culture was negative. Following surgery, the patient received intravenous vancomycin (1 g every 12 hours) for 1 week, followed by oral linezolid (0.6 g every 12 hours). At discharge (Day 21), her muscle strength was graded as follows: right upper extremity, 3/5 and right lower extremity, 4/5. There was no significant improvement in her right palm sensation.

Pathological findings from the abscess walls obtained during the first admission. The postoperative pathology report indicated inflammatory necrosis, neutrophil infiltration, and glial cell hyperplasia, consistent with a brain abscess.
The patient continued oral linezolid (0.6 g every 12 hours) for 1 month after discharge. However, her right upper extremity weakness worsened, accompanied by aphasia, recurrent headaches, nausea, and vomiting. A single episode of limb convulsions occurred on Day 153, and she was readmitted to the hospital on Day 164. Upon readmission, physical examination revealed hypophasia, with muscle strength as follows: distal right upper extremity, 0/5; proximal right upper extremity, 2/5; right lower extremity, 2/5; and left extremities, 5/5. Neck stiffness was mildly positive, and Babinski’s reflex remained positive on the right side. Brain MRI showed multiple abscesses in the left hemisphere, consistent with meningitis (Figure 3). Routine blood tests were normal. The tuberculosis-specific T-cell test (T-SPOT) revealed M. tuberculosis antigen (ESAT-6) of 9 spots and M. tuberculosis antigen (CFP-10) of 24 spots, indicating a positive result. Lumbar puncture revealed normal cerebrospinal fluid (CSF) pressure, with a protein content of 60.8 mg/dL. Tests for M. tuberculosis, rifampicin resistance gene, acid-fast stain, and tuberculosis DNA in the CSF were all negative. Next-generation sequencing (NGS) detected 53 copies of the M. tuberculosis complex in the CSF. The patient denied any history of tuberculosis infection or contact with patients who had tuberculosis. Repeat lung computed tomography showed no new changes, and sputum smears for tuberculosis were negative.
Magnetic resonance imaging (axial view) of the patient at the second admission. The post-contrast gadolinium (a) T2WI, (b) T1WI, (c) DWI, and (d) T2 post-contrast image revealed a nodule-like abnormal signal focus in the left frontal lobe following craniotomy for brain abscess drainage. Postoperative changes were observed in the left cranium, with a nodule-like abnormal signal focus seen in the left frontoparietal region. T2WI showed a mixed high and low signal, and T1WI displayed a mixed isointense and high signal with extensive surrounding edema. After contrast, the lesion showed ring-like enhancement, with significant enhancement of the adjacent meninges and multiple ring-like enhancements in the left cerebral hemisphere. Some lesions exhibited diffusion restriction and meningeal thickening with enhancement. The left lateral ventricle was compressed and deformed, with a shift of midline structures to the right. T1WI, T1-weighted imaging; T2WI, T2-weighted imaging; DWI, diffusion-weighted imaging.
The patient was treated with intravenous meropenem (1 g every 8 hours) for 10 days. A stereotactic brain biopsy of the left frontal lobe was performed on Day 172, and linezolid (0.6 g every 12 hours) was administered for 4 days, along with methylprednisolone (40 mg once daily) and levetiracetam (1 g twice daily) to prevent seizures. The M. tuberculosis smear and nucleic acid rapid test for the brain specimens were positive, confirming the diagnosis of a tuberculous brain abscess. The patient was discharged on Day 184 and prescribed standard anti-tuberculosis therapy (isoniazid, rifampicin, ethambutol, and pyrazinamide) for 12 months.
One year after discharge, the patient reported feeling better and expressed gratitude for the diagnosis. Muscle strength was assessed as follows: distal right upper extremity, 0/5; proximal right upper extremity, 1/5; right lower extremity, 5/5; and left extremities, 5/5. Although mixed aphasia and right palm weakness persisted, symptoms of the brain abscess, such as headaches and other meningeal irritation signs, did not recur.
Discussion
Since 2019, tuberculosis has remained the leading cause of death from a single infectious pathogen. 7 Extrapulmonary tuberculosis accounts for approximately 16% of all newly diagnosed tuberculosis cases worldwide. 4 Among these, the incidence of intracranial tuberculosis is particularly high, with significant mortality and disability rates. Literature reports indicate a fatality rate of approximately 25.4% to 33.3% for intracranial tuberculosis. 8 The most common form of intracranial parenchymal tuberculosis is intracranial tuberculoma, which constitutes approximately 20% of all intracranial lesions in developing countries. By contrast, tuberculous brain abscesses are rare. 9 High-risk factors for tuberculous brain abscesses include HIV infection, malnutrition in children, malignancy, and the use of immunosuppressive drugs. It is often secondary to hematogenous spread of M. tuberculosis, with the primary infection usually originating from the lungs. 10 In the present case, the patient had no history or clinical evidence of pulmonary tuberculosis, and the HIV test was negative, with no signs of immunodeficiency. This combination of findings makes the case particularly unusual. The final diagnosis of a tuberculous brain abscess was confirmed using NGS. 11
Tuberculous brain abscesses can present with clinical symptoms and MRI features similar to those of other bacterial brain abscesses, appearing as cystic lesions with circumferential enhancement. 12 The distinguishing feature is a thicker abscess wall than that of bacterial brain abscesses; however, other definitive characteristics are lacking, making imaging-based diagnosis challenging.13,14 Pathologically, tuberculous brain abscesses can vary significantly, with some cases showing caseous necrosis or granulation tissue15–17 and others lacking the typical tuberculosis-like granulomas.18,19 CSF findings in tuberculous brain abscesses often include high protein levels, low glucose levels, and lymphocytosis, whereas leukocytosis is more common in bacterial intracranial infections. Additionally, neurological symptoms tend to develop later in cranial tuberculous infections because of the gradual spread of inflammatory exudates to cranial nerves, compared with the more rapid progression seen in bacterial infections. 20 Clinically, intracranial tuberculous infections typically have a longer course (2–3 weeks) than bacterial infections, which often develop within 2 to 3 days. 21 In this case, the pathologic examination revealed inflammatory necrosis, neutrophil infiltration, glial cell hyperplasia, and a negative pus culture, complicating the differentiation from a bacterial brain abscess. Furthermore, CNS tuberculosis can mimic a wide range of other disease processes, adding to the diagnostic challenge, especially in an immunocompetent patient with no epidemiological history or lung signs of tuberculosis.
The unclear pathogenesis in this case may have been due to a combination of factors, including the patient’s age, sex, and immune status; the dose of infectious agents; and the immune response of the affected tissues. A limitation of this case was the absence of acid-fast staining of the pathological pus. However, NGS proved to be a valuable diagnostic tool, especially in this atypical case for which standard tests lacked specificity. This highlights the importance of considering tuberculous brain abscesses even in immunocompetent patients, with NGS playing a crucial role in diagnosis when conventional diagnostic methods are inconclusive.
Conclusion
Tuberculous brain abscess should be considered a possible diagnosis, even in immunocompetent patients. The widespread use of NGS technology in clinical settings is likely to facilitate earlier and more accurate diagnoses of tuberculous brain abscesses.
Footnotes
Authors’ contributions
K.C. and H. Z. collected the data and drafted the manuscript. X.L. and H.Z. revised the manuscript. All authors read and approved the final manuscript.
Consent for publication
The patient provided written informed consent for any identifiable photographs and/or clinical information to be used in this study. A copy of the written consent is available for review by the Editor of this journal. The reporting of this study conforms to the CARE guidelines. 22 The patient also consented to all the treatments described in this case report.
Data availability statement
Data will be made available on request. 22
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Ethics approval
This work was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University School of Medicine (ethics approval no. (2023)No.(0454)).
Funding
This work was supported by the National Natural Science Foundation of China (No. 82200052).