
Abstract
The primary etiology of pyomyositis is predominantly Staphylococcus aureus, although Gram-negative bacteria may also be involved on rare occasions. The prognosis for pyomyositis caused by Gram-negative bacteria is more unfavorable than that of infections caused by Staphylococcus aureus. Among Gram-negative bacteria, members of the Enterobacteriaceae family, including Escherichia coli, Klebsiella species, and Salmonella species, have the capacity to produce gas. Gas-forming myositis is a rare phenomenon that primarily affects immunocompromised patients and is associated with a poor prognosis. To the best of our knowledge, no previous reports of gas-forming pyomyositis in an immunocompetent patient exist. We herein present the first documented case of Salmonella-induced gas-forming pyomyositis of the iliacus muscle in a healthy young man with no underlying diseases or comorbidities. Additionally, we reviewed cases of gas-forming pyomyositis in the literature and cases of pyomyositis caused by Gram-negative bacteria in immunocompetent patients.
Introduction
Primary pyomyositis is mainly caused by Staphylococcus aureus and only rarely by Gram-negative bacteria. 1 Pyomyositis caused by Gram-negative bacteria, such as Escherichia coli, Klebsiella species, or Salmonella species, occurs mostly in immunocompromised patients and is associated with a high mortality rate despite surgical intervention and the use of broad-spectrum antibiotics.1–3 Gas-forming pyomyositis is very rare, with most reports involving patients with underlying diseases 4 ; there are no previous reports of gas-forming pyomyositis in immunocompetent patients. We herein report a case of gas-forming pyomyositis caused by Salmonella species in a healthy young man that improved with surgical treatment and antibiotics. We also review prior cases of gas-forming pyomyositis caused by Salmonella species.
Case report
A man in his early 20s was admitted via the emergency room with a 2-day history of increasing left pelvic pain, which made it difficult for him to walk. The patient also reported a fever on the second day of pain. He had no history of trauma, intravenous drug use, or previous comorbidities such as diabetes or autoimmune disease. The patient had experienced diarrhea 3 weeks earlier but had recovered quickly without medication. Physical examination revealed no limitations of motion or tenderness in the hip joint. On admission, the patient’s leukocyte count was 14.9 × 109/L, with 80% neutrophils, 9% lymphocytes, and 8% monocytes. His hemoglobin level was 12.7 g/dL, and his platelet count was 190 × 109/L. His total serum bilirubin, alkaline phosphatase, and liver transaminase levels were normal. The patient’s C-reactive protein level was 16.72 mg/dL, and his erythrocyte sedimentation rate was 59 mm/hour. A serum test for HIV was non-reactive. Computed tomography (CT) showed no abnormalities, but a T2-weighted magnetic resonance imaging scan revealed low signal intensity in the left iliacus muscle (Figure 1(a), (b)).

Imaging findings of gas-forming pyomyositis in the left iliacus muscle. (a) Computed tomography scan showed no abnormalities. (b) T2-weighted magnetic resonance imaging revealed high signal intensity in the left iliacus muscle (white arrow) and (c) follow-up computed tomography scan of the abdomen showed air behind the iliacus muscle (black arrow).
Pyomyositis was diagnosed, and empirical intravenous antibiotic therapy with teicoplanin and piperacillin/tazobactam was initiated. On day 3 of hospitalization, blood culture confirmed Salmonella group D, and the patient was switched to ceftriaxone based on the susceptibility results. His pelvic pain gradually decreased, and his fever subsided. However, on the night of the third hospital day, acute abdominal pain in the left lower quadrant and pelvic pain became severe. A follow-up CT scan of the abdomen and pelvis revealed air behind the iliacus muscle (Figure 1(c)). Incision and drainage were performed, but no definite abscess or muscle necrosis was observed at the surgical site. Wound cultures were consistent with Salmonella group D. The patient’s pain improved dramatically after surgery. After 2 weeks of intravenous ceftriaxone, the patient was discharged in stable condition with oral antibiotics (cefpodoxime 200 mg, twice daily) for 2 weeks. The patient was asymptomatic and had a normal white blood cell count and C-reactive protein level at his clinic visit 2 months later. All patient details were de-identified, and written consent to treatment was obtained from the patient. Because all patient details were de-identified, written informed consent for publication was not necessary. Additionally, because of the nature of this study (case report), the requirement for formal ethics committee approval was waived. The reporting of this study conforms to the CARE guidelines. 5
Discussion
Primary pyomyositis caused by Salmonella
Pyomyositis is a purulent infection of skeletal muscle that can be classified into secondary pyomyositis, caused by penetrating trauma or contiguous spread from an adjacent infection, and primary pyomyositis (formerly known as tropical pyomyositis), caused by hematogenous spread following prior transient or concurrent bacteremia. 1 The clinical course of primary pyomyositis is typically described in three stages. In the first stage, muscle necrosis or pus is not visible on imaging. In the second stage, necrosis or pus becomes visible on imaging, accompanied by severe symptoms. If treatment, including appropriate surgical intervention, is not carried out at this stage, the infection can progress to the third stage, which is characterized by sepsis and poor outcomes. 6
Primary pyomyositis is mainly caused by Staphylococcus aureus, but can, on rare occasions, be caused by Gram-negative bacteria,1,7 including E. coli and Klebsiella species. Most such cases occur in immunocompromised patients and are associated with high mortality and poor outcomes. 8 One important factor influencing mortality in Salmonella pyomyositis is likely the presence of underlying medical conditions. In a review of cases of muscle infection caused by Salmonella species, 10 (41.7%) of 24 cases with underlying medical conditions resulted in death. In comparison, only one (16%) of six cases without underlying medical conditions resulted in death, and the affected patient was 88 years old. 9
Salmonella-induced pyomyositis is not mentioned in textbooks but has been reported in more than 50 cases in the English-language literature.7,9–11
DNA homology studies have shown that most clinically important isolates belong to the Salmonella enterica species. More than 2500 distinct serotypes, based on somatic (O) and flagellar (H) antigens, have been described for this single species, with the most common O-antigen serogroups being A, B, C1, C2, D, and E. Strains from these serogroups are responsible for nearly all Salmonella infections in humans. 12
Although Salmonella typhi was once the primary cause of pyomyositis, its prevalence has recently declined. Non-typhoidal Salmonella infections, particularly Salmonella enteritidis serotype D, have now become more common causes. 13 While non-typhoidal Salmonella typically causes enterocolitis, few pyomyositis cases report prior enterocolitis symptoms. This is likely because most enterocolitis symptoms are mild, self-limiting, and go unrecognized, with pyomyositis often developing 3 to 6 weeks later. Bacteremia occurs in about 5% of Salmonella enteritis cases, forming a focal lesion, and is predominantly seen in immunocompromised patients. 13
Gas-forming pyomyositis
Gas-forming muscle infections are primarily caused by Clostridium and group A Streptococcus species, which lead to muscle necrosis and progress rapidly, often requiring extensive emergency excision. 14 Staphylococcus aureus, the most common cause of primary pyomyositis, does not produce gas and is often treated with antibiotics alone. 15
Gas-forming pyomyositis caused by Gram-negative bacteria is uncommon. However, among reported cases, most have been caused by Enterobacteriaceae, such as K. pneumoniae and Salmonella species, which cause a significant proportion of focal gas formation in soft tissue and muscle infections. 16
Nine of 10 reported patients with gas-forming myositis due to K. pneumoniae died despite aggressive treatment, with diabetes being the most common underlying medical condition.2,17–21 By contrast, gas-forming pyomyositis caused by Salmonella has been reported in nine cases, including our case, most of which involved underlying disease, with only three resulting in death. Cases of gas-forming pyomyositis caused by Salmonella species are summarized in Table 1.
Gas-forming pyomyositis caused by Salmonella species.
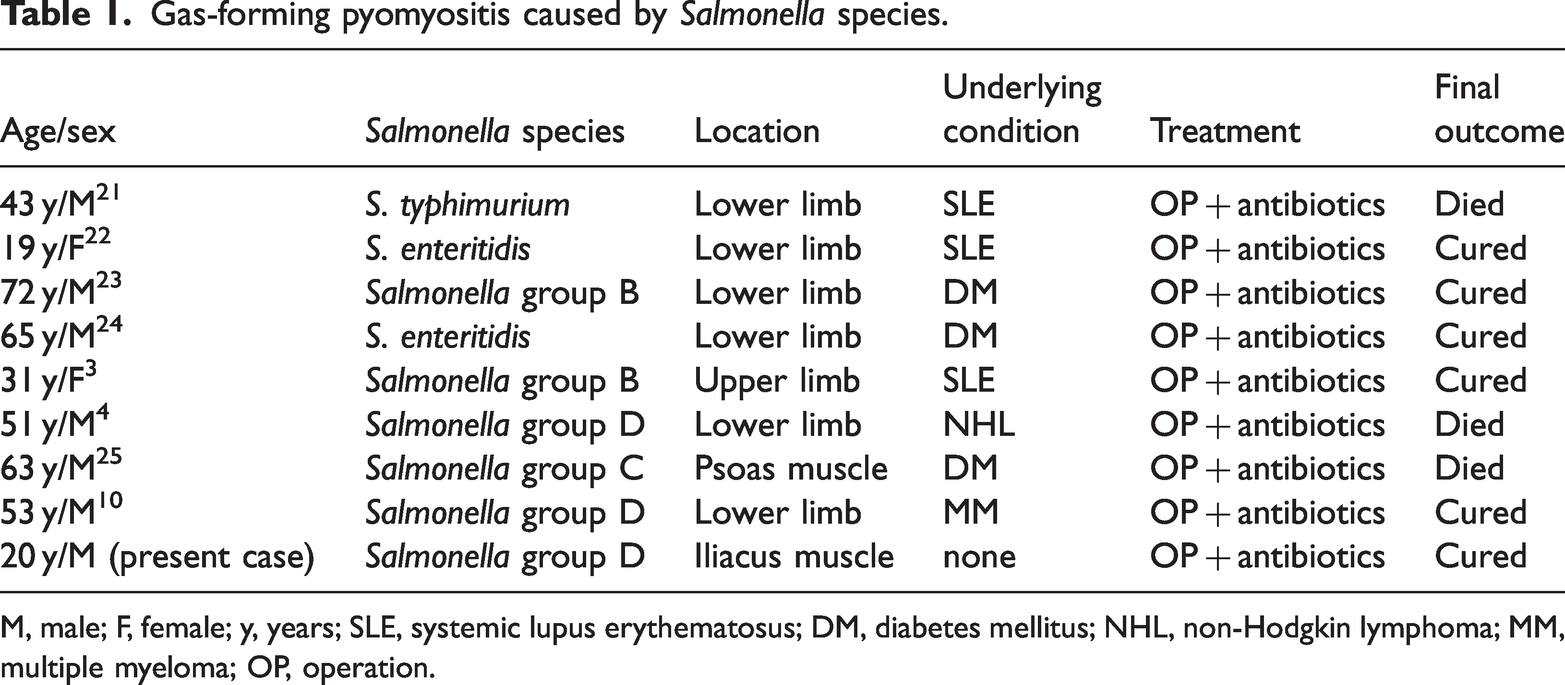
M, male; F, female; y, years; SLE, systemic lupus erythematosus; DM, diabetes mellitus; NHL, non-Hodgkin lymphoma; MM, multiple myeloma; OP, operation.
Gas-forming myositis does not appear to be associated with increased mortality in Salmonella infections. While gas-forming lesions require attention, gas formation itself is not believed to increase mortality. Gas-forming pyomyositis caused by Klebsiella infection has a higher mortality rate than those caused by Salmonella, but the underlying reason for this difference remains unclear.
Pyomyositis in immunocompetent patients
Underlying diseases are thought to have the greatest influence on the course of pyomyositis, making it rare for primary pyomyositis to occur in immunocompetent patients without a history of trauma, as seen in this case.
The predominant bacterium causing pyomyositis in immunocompetent patients is Staphylococcus aureus. Muscle infections caused by Staphylococcus aureus are more common in young men and are often treated with antibiotics alone. Although antibiotic resistance may pose challenges with methicillin-resistant Staphylococcus aureus, there have been no reports of death from pyomyositis caused by Staphylococcus aureus in an immunocompetent patient.15,26–28 Most cases of pyomyositis without underlying disease are caused by Gram-positive bacteria such as Staphylococcus aureus or by polymicrobial infections associated with trauma. Primary pyomyositis caused by Gram-negative bacteria in immunocompetent patients is extremely rare. 29 We identified cases of pyomyositis caused by Gram-negative bacteria in immunocompetent patients from the English-language literature, which are summarized in Table 2.
Pyomyositis caused by Gram-negative bacteria in immunocompetent patients.

M, male; F, female; y, years; mo, months; I & D, incision and drainage.
The patients ranged in age from 23 months to 59 years, and all infections occurred in the lower extremities or the iliopsoas muscles associated with the lower extremities. Three of the four patients were male, and Salmonella species caused three of the infections. In contrast to Gram-negative pyomyositis associated with underlying diseases, which has a high mortality rate, all four patients recovered without complications following aspiration or surgical intervention and appropriate antibiotic therapy.
In our case, there was no underlying disease, and the lesion was located at a relatively deep site near the pelvic brim. Incision and drainage would have required a large skin incision and deep dissection, so the initial approach was to monitor the patient with antibiotics effective against Gram-negative bacteria, without surgery. During the first 3 days of antibiotic treatment, the patient’s pain and fever decreased. However, the pain subsequently worsened, and a follow-up CT scan revealed new-onset gas, prompting surgical intervention. No pus was observed in the surgical field, and no muscle necrosis was noted. The patient recovered after the operation, with rapid improvement in symptoms. Based on this experience, it is recommended that even when lesions are in inaccessible locations, surgical intervention should be considered to resolve pyomyositis, even if only for decompression. In reported cases of pyomyositis caused by Gram-negative bacteria, most patients underwent surgical intervention, which is a critical factor for treatment and prognosis.
Conclusions
In immunocompetent patients, primary pyomyositis is predominantly caused by Staphylococcus aureus and is usually resolved with appropriate antibiotic treatment. However, the possibility of Gram-negative bacteria as the causative agent should be considered, particularly in patients with immunosuppression or chronic conditions such as diabetes. Surgical intervention should not be delayed if severe pain or fever persists during appropriate antibiotic therapy.
Footnotes
Acknowledgement
We thank Dr. Tae Hoon Noh from the Department of Infectious Diseases for his assistance in treating this patient.
Author contributions
Gyu Min Kong participated in the data collection and analysis and drafted the article. Jee Young Lee supervised the study and reviewed and revised the manuscript. Both authors have read and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.