
Abstract
Nontyphoidal Salmonella (NTS) infection can lead to gastroenteritis, enteric fever, and bacteremia. However, bone and joint infections due to NTS are rarely encountered, accounting for only 0.8% of all Salmonella infections and 0.45% of all types of osteomyelitis. We herein report an extremely rare case of acute multifocal osteomyelitis (bilateral femurs and left tibia) with septic arthritis of the bilateral hips caused by Salmonella Dublin in an immunocompetent adult. We performed thorough debridement of the bilateral hips and surgical decompression of the involved bones. At 1 year of follow-up, the patient’s inflammatory biomarkers were within normal limits, and clinical and radiologic examinations showed no signs of infection. We emphasize that invasive NTS can lead to multifocal bone and joint infections in immunocompetent adults. The manifestations of Salmonella osteomyelitis may be insidious; thus, we recommend performing a simultaneous magnetic resonance imaging examination of the bone adjacent to the infected joint to avoid missed or delayed diagnosis. Thorough surgical debridement combined with a long course of sensitive antibiotic therapy is essential to eradicate the infection.
Keywords
Introduction
Nontyphoidal Salmonella (NTS) is a common causative agent of foodborne infections in humans. Bone and joint infection is a rare complication of NTS infection and is usually unifocal and asymmetric. 1 Such infections usually occur in patients with predisposing conditions such as sickle cell disease, systemic lupus erythematosus, use of immunosuppressive drugs, diabetes, and previous surgery or trauma involving the bone.2–4 We herein report an extremely rare case of acute osteomyelitis of the bilateral femurs and left tibia with septic arthritis of the bilateral hips due to Salmonella Dublin in an immunocompetent adult.
The current report aims to provide a clear description of the diagnosis and management of this case, highlighting that invasive NTS can lead to systemic multifocal bone and joint infections in immunocompetent adults.
Case report
A 28-year-old man was admitted to our emergency department with a 1-month history of pain in the bilateral hips and left lower extremity with fever. He reported a history of trauma in his left knee and calf 10 days before the onset of symptoms. No open wound or fracture was present. The patient went to a local clinic for intra-articular steroid injections to reduce the pain and swelling. He had no history of underlying diseases or immunodeficiency. Before admission to our hospital, he had received intravenous ceftriaxone infusion (2 g/day) for 2 weeks, but intermittent fever persisted during the infusion of antibiotics.
Laboratory evaluation on presentation to our emergency department showed a C-reactive protein (CRP) level of 78.4 mg/L (reference range, <5 mg/L), an erythrocyte sedimentation rate (ESR) of 80 mm/1st hour (reference range, 0–21 mm/1st hour), and a white blood cell (WBC) count of 9.82 × 109/L (reference range, 3.5–9.5 × 109/L) (neutrophils, 70.2%; lymphocytes, 19.2%; monocytes, 9.3%; eosinophils, 1.0%; and basophils, 0.3%). A purified protein derivative skin test was strongly positive. Although the patient denied a history of tuberculosis, a tuberculosis antibody test and tuberculosis interferon-gamma release test were positive. No mycobacteria were found on a sputum smear, and chest computed tomography (CT) showed no abnormalities. Hip CT showed uneven changes in the bone density of the bilateral femoral heads and hip joint capsule effusion. The patient was treated with intravenous levofloxacin (0.5 g once daily) combined with cefmetazole (1 g every 12 hours), and he had no fever except on the day of admission. He was then referred to the Tuberculosis Department because of concerns about tuberculosis of the hip. He developed an intermittent fever with a maximum body temperature of 39°C. The intravenous levofloxacin was continued, and piperacillin/tazobactam was added. However, both the blood culture and joint fluid culture were negative.
Despite treatment, the pain in the hips and sacrococcygeal region persisted. The patient’s inflammatory biomarkers remained high, with a CRP level of 79.4 mg/L, ESR of 97 mm/1st hour, and WBC of 8.43 × 109/L (neutrophils, 70.0%; lymphocytes, 17.6%; monocytes, 10.1%; eosinophils, 1.9%; and basophils, 0.4%). Our department actively excluded rheumatic immune diseases such as ankylosing spondylitis. HLA-B27 was positive, but CT of the sacroiliac joint and thoracolumbar spine showed no abnormalities. After consultation with the Department of Rheumatology and Immunology, oral sulfasalazine and imrecoxib were added to the treatment regimen. We performed bilateral hip joint aspirations for bacteriological culture on two consecutive days. The second aspiration produced turbid synovial fluid with a nucleated cell count of 10,000 × 106 (99% polymorphonuclear neutrophils). Salmonella Dublin was isolated from the synovial fluid of the bilateral hips, and Staphylococcus hominis was also cultured in the right hip. We further inquired about the patient’s medical history, and he added that he had eaten half-cooked beef, caught a cold, and drank heavily at the time of his left knee injury. However, he had no gastrointestinal symptoms, such as diarrhea. We used a Thomas stent with bilateral 3-kg skin traction to pull his lower limbs, preventing further narrowing of the joint space and alleviating the hip pain. At the same time, we administered an intravenous infusion of vancomycin (1 g every 12 hours) combined with piperacillin/tazobactam (4.5 g every 8 hours) according to the results of the bacterial culture and drug susceptibility tests.
After 10 days of conservative treatment, the patient’s fever recurred (maximum body temperature of 39°C). Salmonella Dublin was found in the blood culture. He complained of unbearable pain in the bilateral hips and left knee. Notably, X-ray and CT examinations showed hip joint space narrowing and destruction of the femoral head, peri-acetabular bone, and left upper tibia (Figure 1(a)–(d)), and magnetic resonance imaging (MRI) of the hip showed multiple abnormal signals and joint capsule effusion (Figure 2(a)–(c)). This indicated that the disease was rapidly progressing, and septic arthritis of the bilateral hips and acute osteomyelitis of the left tibial plateau were confirmed. We actively performed debridement of the bilateral hip lesions, drilling for decompression, and drainage of the left tibial osteomyelitis. Both the intraoperative findings and postoperative pathology confirmed the previous diagnosis.

Radiograph and computed tomography scans of the patient 1 month after onset of symptoms. (a) Anteroposterior radiograph of the hip revealed joint space narrowing and (b)–(d) Computed tomography of the hip and knee joint showed bone destruction in the femoral head and neck and an irregular shadow in the posterior part of the left upper tibia. Images were taken 1 month after the onset of symptoms.
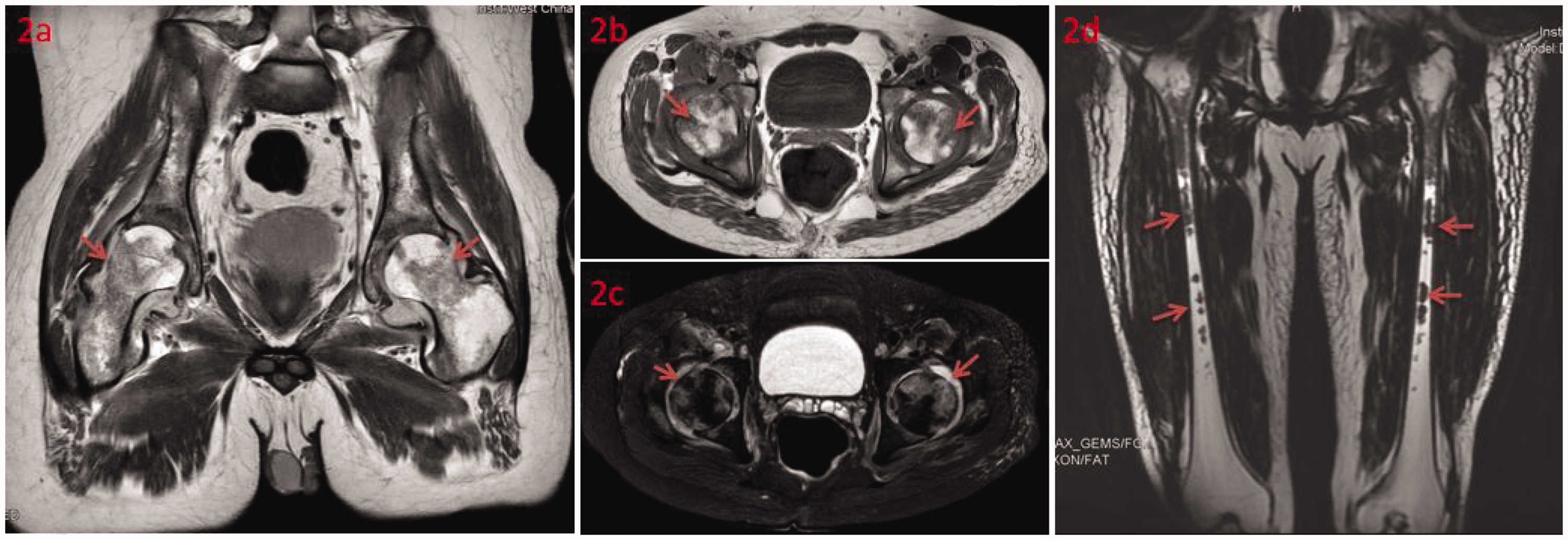
Magnetic resonance imaging of the patient. (a)–(c) Magnetic resonance imaging of the hip showed joint capsule effusion and multiple abnormal signals in the acetabulum and femoral head. Images were taken before the first surgery and (d) Magnetic resonance imaging of the bilateral thighs showed a patchy T2 signal in the bilateral femoral shafts and diffuse swelling of the bilateral thigh soft tissue. Images were taken after the onset of thigh pain and fever.
Although the pain in the hips and left knee was relieved, the patient developed fever again on the second postoperative day (maximum body temperature of 41°C). The antibiotic was immediately upgraded to meropenem (1 g every 8 hours) combined with vancomycin (0.5 g every 8 hours). The patient described throbbing pain of the bilateral thighs. Blood examination showed that the WBC count was 2.24 × 109/L (neutrophils, 62.1%; lymphocytes, 24.1%; monocytes, 10.7%; eosinophils, 2.7%; and basophils, 0.4%), the CRP level was 110 mg/L, and the ESR was 86 mm/1st hour. The decrease in WBCs was considered related to severe infection. Thigh MRI showed multiple abnormal signals in the bilateral femoral shafts (Figure 2(d)). The diagnosis of acute osteomyelitis of the bilateral femurs was confirmed, and we performed burr-hole and fenestration decompression of the bilateral femurs with catheter drainage. During the operation, obvious pus and necrotic granulation tissue were found in the femoral medullary cavity. The fever and thigh pain were relieved after the second operation. X-ray examination 10 days after the second surgery showed stable hip joints and lateral fenestration of the bilateral upper femurs (Figure 3(a), (b)).

Radiographs of the patient 1 year after discharge. (a), (b) Anteroposterior radiograph of the hip showed stable hip joints stable and lateral fenestration of the bilateral upper femurs. Images were taken 10 days after the second surgery and (c) Anteroposterior radiograph of the hip taken 1 year after discharge.
The patient’s treatment was changed from vancomycin to linezolid because of a high vancomycin blood concentration and drug eruption. After continuing intravenous infusion of meropenem and linezolid for 2 months followed by oral ciprofloxacin for 3 months, his CRP level decreased to 8.75 mg/L, ESR was 10 mm/h, and WBC count was 6.44 × 109/L (neutrophils, 64.1%; lymphocytes, 26.5%; monocytes, 6.8%; eosinophils, 1.9%; and basophils, 0.7%). During 12 months of outpatient visits, he reported that his symptoms were relieved and that there was no recurrence of infection. He was able to walk for a short distance of approximately 800 m. Physical examination revealed the following range of motion statistics of the bilateral hips: flexion/extension, 60/10 degrees; abduction/adduction, 20/20 degrees; and external rotation/internal rotation, 20/20 degrees. He preferred hip-preserving treatment, thus choosing to undergo follow-up and hip function rehabilitation training (Figure 3(c)), which he was undergoing at the time of this writing.
The patient provided written informed consent for treatment and publication of this report. The Ethics Committee on Biomedical Research of our hospital approved this study (approval no. 2022-1494). The reporting of this study conforms to the CARE guidelines. 5
Discussion
Bone and joint infections due to NTS infection account for only 0.8% of all Salmonella infections and 0.45% of all types of osteomyelitis. 6 NTS is more prone to causing single joint or bone infection and occurs more often in patients with underlying diseases or immune abnormalities. However, one study demonstrated that Salmonella osteomyelitis and septic arthritis also occur in immunocompetent adults, mainly through bloodstream transmission, and the common risk factors for Salmonella infection are often absent in these patients. 7
Bacterial invasiveness and disease severity vary widely between different NTS serotypes. Salmonella Dublin is a bovine-adapted serotype, but human infection may still occur by the consumption of raw milk, milk products, or beef. 8 Salmonella Dublin is aggressive and more likely to cause serious illnesses such as bloodstream infections than other NTS serotypes, and most infected patients have no apparent immunodeficiency.8,9 We believe the cause of the infection in the present rare case is traceable. First, the patient had eaten half-cooked beef before the symptoms appeared. Although he had no obvious gastrointestinal symptoms, it is likely that Salmonella Dublin had invaded his gastrointestinal tract and remained dormant in the reticuloendothelial system or the bowel, later becoming activated by a reduction in the immune response. 6 Second, the patient drank heavily and caught a cold during this period, which may have compromised his immune function, leading to a bloodstream infection. Finally, he had a history of trauma in the left lower extremity and underwent intra-articular injections of steroids. Although there was no evidence of fracture, microvascular damage to the periosteum or tissue may have been present locally, and Salmonella isolates may have seeded the injured site during hematogenous transmission, leading to osteomyelitis.
Additionally, our patient complained of sacrococcygeal pain and tested positive for HLA-B27. Therefore, the differential diagnoses included ankylosing spondylitis and reactive arthritis. However, the patient had no family history of spondyloarthritis and did not report any previous spinal or joint symptoms. Furthermore, CT of both the sacroiliac joint and thoracolumbar spine showed no abnormalities; thus, we had insufficient evidence to diagnose ankylosing spondylitis. With respect to reactive arthritis, the patient had no symptoms of enteritis or other evidence of a preceding symptomatic infection. Moreover, the affected regions did not meet the major criteria of asymmetric monoarthritis or oligoarthritis in the guidelines. 10 Finally, the patient did not undergo immunohistology or polymerase chain reaction of the sacroiliac joint. Thus, the diagnosis of reactive arthritis remains questionable.
Salmonella osteomyelitis usually affects the diaphysis of long bones, especially the femur and humerus. 6 This may be ascribed to increased bone marrow activity and blood degradation products.6,11 Most of the previously reported cases involved unilateral femoral osteomyelitis (see Appendix 1). Our patient developed simultaneous acute osteomyelitis of the left tibia and bilateral femurs. Common clinical symptoms of Salmonella osteomyelitis include fever, bone pain, tenderness, and soft tissue swelling. However, its manifestations can also be nonspecific and insidious, 7 leading to a delayed or missed diagnosis. In this case, the symptoms and X-ray/CT imaging features did not show obvious evidence of femoral osteomyelitis in the early stage. The reappearance of high fever, subsequent throbbing pain in the thighs, and additional thigh MRI helped us finally establish the diagnosis of bilateral femoral osteomyelitis. This case suggests that X-ray or CT may have insufficient sensitivity, whereas MRI is sensitive to fluid and soft tissue signals and is more accurate and effective for the early diagnosis of acute Salmonella osteomyelitis. 12 MRI can be used to identify bone marrow edema (BME) in the affected bone, which is a crucial factor in diagnosing osteomyelitis. In acute osteomyelitis, the bone marrow becomes congested with fluid and pus, resulting in low signal intensity on T1-weighted images and high signal intensity on fluid-sensitive and post-contrast sequences. 13 Thus, marrow and soft tissue edema will be more diffuse and extensive in acute osteomyelitis. Another characteristic finding highly suggestive of acute osteomyelitis is the presence of intramedullary and extramedullary fat globules, which appear as foci of high T1 signals. 14 However, BME is a more equivocal feature that is often seen in other pathologies, such as ankylosing spondylitis. In ankylosing spondylitis, the areas of affected bone marrow observed on MRI are typically located periarticularly or in another typical anatomical area (e.g., subchondral bone marrow). 15 Additionally, other MRI findings of structural damage co-existing with BME, such as erosion, fat metaplasia, and sclerosis, may further support the diagnosis. 15
Various antibiotic options are available for Salmonella infection, including fluoroquinolones, third-generation cephalosporins, and cotrimoxazole.6,7,16 Fluoroquinolones are advocated as excellent choices because of their potent anti-Salmonella activity and good bone penetration. 17 Once septic arthritis or acute osteomyelitis is suspected, administration of broad-spectrum intravenous antibiotics should begin. The dosage must be modified based on the results of the antibiogram because the rate of antibiotic resistance is constantly increasing.3,7,8 The Salmonella Dublin isolated in the present case was resistant to first-generation cephalosporins, aminoglycosides, penicillins, and nalidixic acid but sensitive to third-generation cephalosporins and ciprofloxacin. Intravenous antibiotics should be continued for at least 4 to 6 weeks.3,18 Our patient received intravenous levofloxacin after admission, and the antibiotic therapy was then adjusted to intravenous linezolid combined with meropenem according to the blood culture and severity of infection. Infusion continued for 2 months after discharge and was followed by oral ciprofloxacin for 3 months.
In addition to effective antibiotic therapy, surgical treatment is also critical for Salmonella septic arthritis and osteomyelitis. In patients with septic arthritis, surgical debridement is the first choice to eradicate the infection. 19 Routine open debridement includes removal of all accessible synovial tissue, capsulectomy, and drain placement. 20 For Salmonella osteomyelitis with bacteremia, debridement of the lesions and drilling or fenestration decompression are required. 12 In the present case, we actively prepared a surgical plan because the patient had multifocal infection with a frequently recurring high fever. We first performed bilateral hip debridement and decompression of the left upper tibia because of the delayed diagnosis of bilateral femoral osteomyelitis. After confirming that diagnosis, we performed burr-hole and fenestration decompression of the bilateral femurs with adequate drainage. After these two operations, his symptoms gradually resolved, and the infections were eradicated.
Conclusion
Although extremely rare, bone and joint infections in immunocompetent adults caused by invasive NTS, such as Salmonella Dublin, may be multifocal, and some lesions are insidious. Symptoms, signs, bacteriological cultures, and sensitive imaging methods (i.e., MRI) should be considered together to establish an early diagnosis and avoid missing possible coexisting insidious Salmonella osteomyelitis. We emphasize the need for early and thorough debridement of joint lesions, decompression and drainage of osteomyelitis, and susceptible and effective long-course antibiotic therapy to help eradicate the infection and reduce the pain and destruction of joints and bones.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231198382 - Supplemental material for Acute multifocal osteomyelitis with septic arthritis caused by nontyphoidal Salmonella in an immunocompetent young adult: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231198382 for Acute multifocal osteomyelitis with septic arthritis caused by nontyphoidal Salmonella in an immunocompetent young adult: a case report by Boyi Jiang, Hong Xu and Zongke Zhou in Journal of International Medical Research
Footnotes
Author contributions
Boyi Jiang: Study design and conception, drafting of the manuscript. Hong Xu: Study design and conception. Zongke Zhou: Critical review of the manuscript. All authors: Approval of the manuscript for publication.
Availability of data and materials
The datasets used and analyzed during the current study are available from the first or corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the “1•3•5 Project for Disciplines of Excellence” at West China Hospital, Sichuan University (ZYJC18039) and by the Regional Innovation & Cooperation Program of the Science & Technology Department of Sichuan Province (2021YFQ0028).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.