
Abstract
Objective
To investigate the correlations between multigene alterations and clinicopathological features in papillary thyroid carcinoma (PTC) samples.
Methods
In this retrospective study, 111 cytological specimens of thyroid nodules, including 74 PTC samples and 37 benign samples, were analyzed using a 22-gene mutation assay employing next-generation sequencing. Clinicopathological information was retrospectively collected and analyzed.
Results
Gene alterations were associated with a higher rate of lymph node metastasis (LNM) and thyroid capsular invasion, a lower rate of coexisting Hashimoto's thyroiditis, the classical PTC subtype, and younger age (<45 years). Among the 22 genes tested, the BRAF mutation rates showed a significant difference between the PTC and benign groups. In the subgroup analysis, younger age (odds ratio = 12.512, 95% confidence interval: 3.126–50.087) was an independent risk factor for LNM. In further analyses, BRAF mutation was significantly associated with LNM in the older subgroup (age ≥ 45 years), suggesting that the BRAF mutation test has greater value for determining PTC prognosis in the older age group.
Conclusions
Our findings will provide a more comprehensive understanding of the relationship between gene mutations and PTC and may contribute to improved PTC management.
Keywords
Introduction
Papillary thyroid carcinoma (PTC) accounts for the majority of thyroid cancer cases; 80% of thyroid cancer cases are papillary carcinoma. 1 In recent years, a considerable increase in the incidence of PTC has occurred in many parts of the world.2,3 Even after excluding factors such as the expanded use of ultrasonic technology and the more general acceptance of early cancer screening,4,5 the true PTC incidence rate has still increased in recent decades. 6 PTC is generally associated with a good prognosis and a high survival rate when diagnosed early, 7 with a 10-year survival rate of over 95%. 8 However, the risk of relapse or persistent disease is still approximately 30%.8–11 Currently, an increasing number of researchers are focusing on the possibility of selecting patient groups with different risks for unfavorable outcomes to match a particular therapeutic approach and improve PTC outcomes.12,13 Clinicopathologic factors correlated with unfavorable outcomes include male sex, older age, large tumor size, extrathyroid invasion, lymph node metastasis (LNM), and distant metastasis.9,14
Molecular characteristics are also potential prognostic factors for PTC patients. PTC and its molecular features have been widely researched in recent decades. The BRAFV600E mutation is the most frequent gene variation in PTC, accounting for approximately 90% of mutations in differentiated thyroid cancer. 15 This mutation is a point mutation at codon 600 of BRAF, resulting in the substitution of valine with glutamate (V600E). This leads to the constitutive activation of BRAF kinase and the mitogen-activated protein kinase (MAPK) signaling pathway, promoting uncontrolled proliferation and differentiation of PTC cells. Rearranged during transfection (RET) is a proto-oncogene implicated in PTC, with the second-highest frequency after BRAFV600E in PTC. 16 In addition, APC, RAS, and TERT are other important gene alterations in PTC.17,18 In general, most important mutant genes in PTC are included in the MAPK pathway.
Genetic alterations in PTC may be correlated with different clinicopathological features. The relationship between genetic alterations and clinicopathological factors can also indicate the relationship between genetic alterations and prognosis to some extent when prognosis-related information is unavailable. However, the correlations between gene mutations and clinicopathological features in PTC prognosis are still controversial. For example, BRAFV600E has been associated with adverse outcomes in PTC patients in some reports, while other studies have reached the opposite conclusion.19,20 RET/PTC3 has also been shown to be associated with a highly aggressive phenotype, while RET/PTC1 rearrangement is not associated with any clinicopathological features of PTC. 21 Therefore, further research is necessary to fully understand the impact of molecular alterations in PTC on the prognosis and even the diagnosis of PTC. In this study, cytological samples of thyroid nodules were collected for a 22-gene mutation sequencing assay. Furthermore, both molecular variation landscape examinations and thorough morphologic assessments were conducted to investigate the relationships between these genetic changes and the clinical and pathological aspects of PTC. Careful evaluation of clinicopathological features and gene mutations is considered helpful for predicting the clinical course of PTC. In addition, we evaluated the diagnostic performance of this multigene test in cytologically indeterminate nodules to explore its clinical application in auxiliary diagnosis.
Methods
Patients and specimens
Cytologic samples of thyroid nodules obtained by fine-needle aspiration biopsy (FNAB) were collected from the First People’s Hospital of Jiangxia District, Wuhan City, between June 2021 and October 2022. All data were collected and analyzed retrospectively. Our study was approved by the ethics committee of the First People’s Hospital of Jiangxia District, Wuhan on 5 March 2021 (No. 2021019) and was conducted in accordance with the declaration of Helsinki and the National Guidelines for Diagnosis and Treatment of Thyroid Cancer 2022 in China. 21 Written informed consent was obtained from all individual participants included in the study. All patients with thyroid nodules were diagnosed by ultrasonography and underwent FNAB or thyroidectomy to determine the final diagnosis. The reporting of this study conforms to the STROBE guidelines.22,23 The procedures used complied with the relevant guidelines and regulations. All patient details were de-identified.
Pathological review
Medical records, pathologic evaluations, and surgical pathology reports were reviewed to collect the demographic parameters and clinicopathologic characteristics of tumors. FNAB cytologic sample slides were examined and confirmed by two experienced pathologists, and if necessary, a third pathologist provided final confirmation of the different pathological tumors. Seven tumor pathological features were evaluated and recorded, including 1) tumor size (≤1 or >1 cm), 2) LNM, 3) thyroid capsular invasion, 4) multifocality, 5) presence or absence of Hashimoto's thyroiditis (HT), 6) presence or absence of nodular goiter, and 7) PTC subtype.
DNA extraction
Genomic DNA was extracted from cytological sample sections with at least 20% tumor cells using the QIAmp DNA Mini Kit (Qiagen, Hilden, Germany) following the manufacturer’s instructions. Then, 1% agarose gel electrophoresis was performed for DNA qualification. The concentrations of all samples were quantitated using a NanoDrop system (Invitrogen Life Technologies, Carlsbad, CA, USA) and a Qubit Fluorometer (Invitrogen Life Technologies).
Next-generation sequencing (NGS)
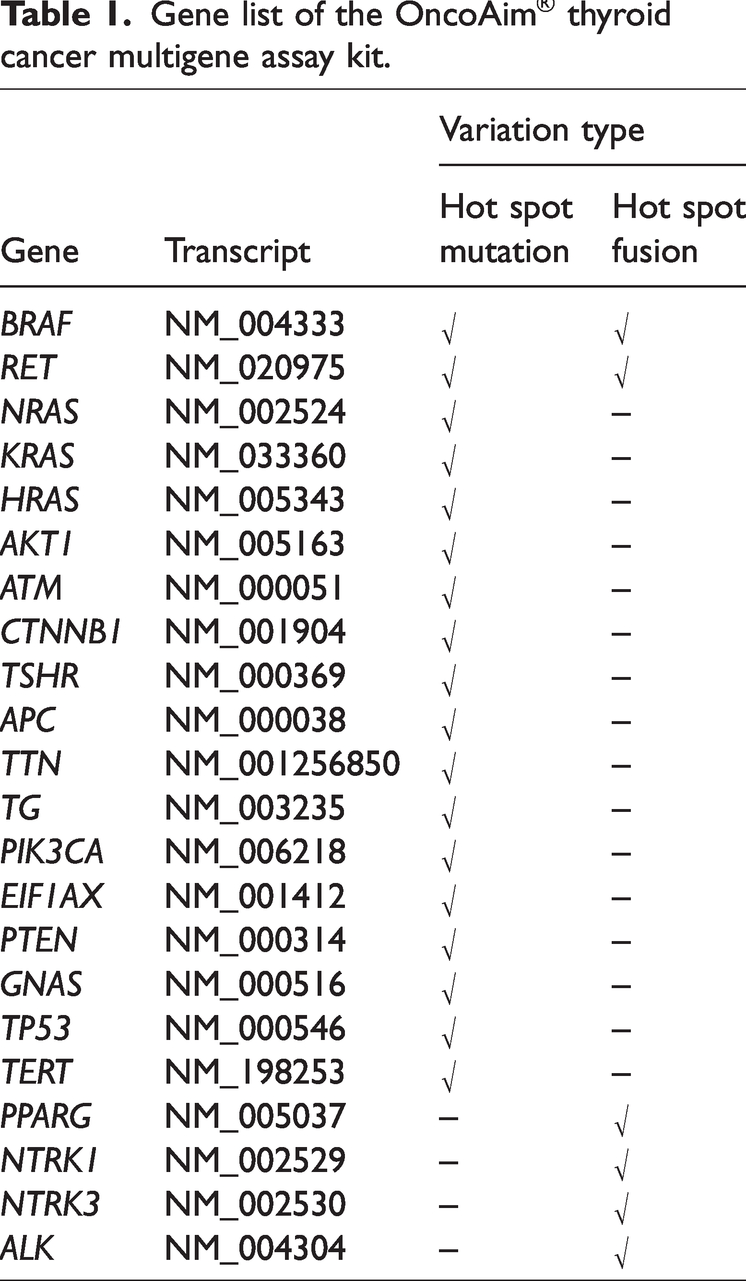
NGS was performed using the OncoAim® thyroid cancer multigene assay kit (Singlera Genomics, Inc., Shanghai, China). The OncoAim kit included 22 genes, as shown in Table 1, Supplementary Table 1, and Supplementary Table 2. The multigene assay kit was designed to simultaneously detect hot spot variations in these 22 genes, including single nucleotide variations, short insertions and deletions, and gene rearrangements. All 22 genes had been previously detected in tumor tissue of PTC patients and shown to include “pathogenic” or “likely pathogenic” variations, such as BRAF, RET, and TERT. The input DNA quantity for sequencing library preparation was 50 ng for each sample, and the DNA was fragmented using 5× WGS Fragmentation Mix (Qiagen, Beverly, MA, USA). After quality control and quantification, the library products were sequenced using 150-bp paired-end runs on a NextSeq 500 system (Illumina, Inc., San Diego, CA, USA), and the average sequencing depth was 10,000×.
Gene list of the OncoAim® thyroid cancer multigene assay kit.
Sequencing data were processed following the guidelines of the OncoAim® kit (Singlera). Sequencing reads were first quality-filtered using Trim-Glore software (version 0.4.0, https://www.babraham.ac.uk/science-facilities/bioinformatics) and then mapped to the reference human genome (hg19) using BWA software (version 0.7.12, http://sourceforge.net/projects/bio-bwa/files/bwakit/). After mapping, FreeBayes software (version 1.0.2, https://travis-ci.org/ekg/freebayes) was used to call single nucleotide variations and short insertions and deletions, and Blastall software (version 2.2.20, https://blast.ncbi.nlm.nih.gov/Blast.cgi) was used to call gene fusion. Hgvs annotation for single nucleotide variations and short insertions and deletions was performed using Ensembl Variant Effect Predictor (release-84, http://www.ensembl.org/info/docs/tools/vep/script/index.html). The minimum confidence threshold for variant calling was set to 2%. The gene variation result was classified as pathogenic, likely pathogenic, inconclusive, uncertain significance, likely benign, or benign according to the information from the ClinVar database. In this study, “pathogenic” or “likely pathogenic” results were considered positive.
Statistical analysis
SPSS statistical software (version 27.0, IBM Corp., Armonk, NY, USA) was used for all statistical analyses. R software (www.r-project.org) was used to create all figures. Continuous data are expressed as the mean ± standard deviation and were analyzed via an independent Student’s t-test or the Wilcoxon–Mann–Whitney test. Categorical data are expressed as quantities and percentages (n, %) and were analyzed via Pearson’s χ2 test or Fisher’s exact test. Univariate and multivariate logistic regression analyses were conducted to evaluate the risk factors of the dependent variable. A two-tailed P value of <0.05 was regarded as statistically significant. Patients with incomplete or missing pathological data were not included in the statistical analysis. The performance of the multigene test in diagnosing cytologically indeterminate nodules was evaluated by sensitivity and specificity analyses.
Results
Detection of mutations
In total, 142 thyroid nodule cytologic samples were collected from 135 enrolled patients at the First People’s Hospital of Jiangxia District, Wuhan City, between June 2021 and October 2022. Of the 142 samples, 111 were available for analysis (Figure 1), including 74 PTC nodule samples and 37 benign nodule samples. Seventy-four malignant thyroid nodule samples were obtained from 71 PTC patients, including 22 men and 49 women, with ages ranging from 21 to 71 years and an average age of 46 years. The remaining 37 benign samples were from 37 patients with benign thyroid disease, including 7 men and 30 women, with ages ranging from 21 to 77 years and an average age of 55 years. All malignant thyroid nodules were histologically diagnosed as PTC after initial surgeries. Of the patients with benign nodules, 21 underwent thyroidectomy and were diagnosed with benign results, while the other 16 patients underwent FNAB and received non-malignancy results based on the Bethesda class 24 [class I (n = 1); class II (n = 11); class III (n = 4)]. Information regarding the samples is shown in Table 2 and Supplementary Table 3.

Consort diagram.
Clinicopathologic characteristics and mutation information of PTC and benign nodules.

LNM, lymph node metastasis; HT, Hashimoto’s thyroiditis; PTC, papillary thyroid carcinoma; SD, standard deviation; NG, nodular goiter.
Age and sex calculations were based on patient information; other data calculations were based on nodule information.
Among the 74 PTC cytological samples, 79.7% (59/74) exhibited at least one mutation of the 22 genes tested. Specifically, 62.2% (46/74) showed the presence of a BRAFV600E point mutation, 8.1% (6/74) demonstrated RET/PTC1 mutations, and 6.8% (5/74) displayed RAS mutations. Notably, among all PTC cases, 55 had a single gene mutation, 4 had two gene mutations (all involving BRAF), and 15 did not exhibit any mutations. Among the 37 benign cases, 21.6% (8/37) showed gene mutations, with 7 mutations being RAS mutations, 6 of which were identified as located on codon 61 of the RAS gene. Details of all the mutant cases are shown in Figure 2.

Landscape of mutation profiles in the PTC and benign groups. The waterfall diagram shows the cases with gene mutation only. PTC: papillary thyroid carcinoma. BTN: benign thyroid nodules.
The mutation rates were significantly different between the PTC group and the benign group (79.7% vs. 21.6% P < 0.001) (Table 3 and Figure 3). Among all single gene mutations, only the BRAFV600E mutation rate exhibited a significant difference between the PTC group and the benign group (62.2% vs. 0%, P < 0.001) (Table 3 and Figure 3).
Comparison of gene mutation rates between benign thyroid nodule patients and papillary thyroid carcinoma patients.
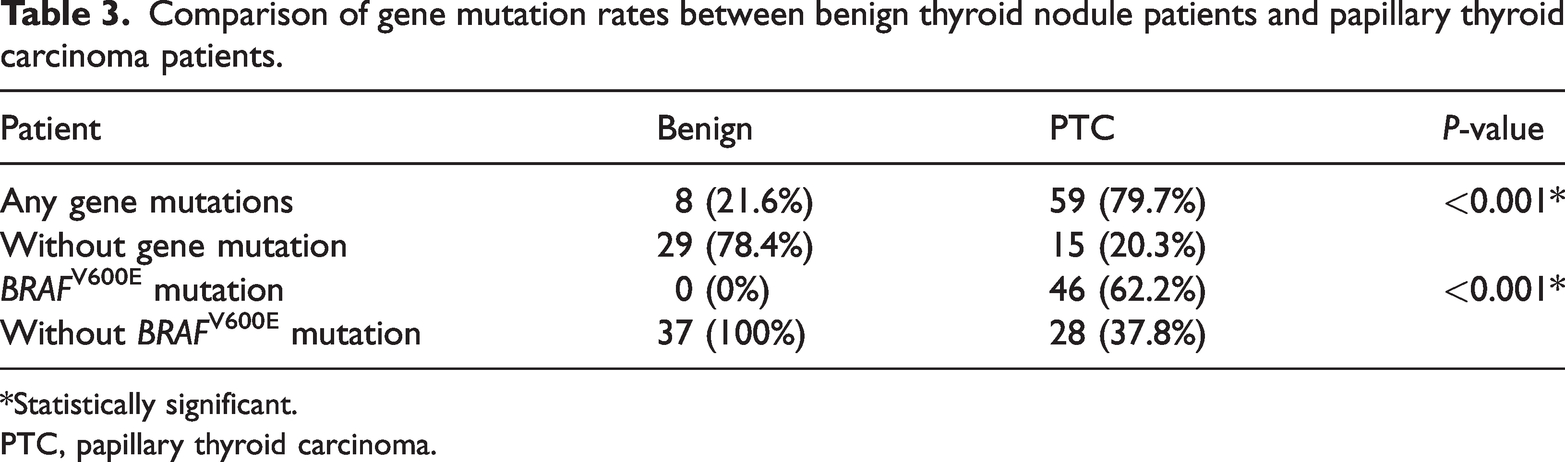
*Statistically significant.
PTC, papillary thyroid carcinoma.

Proportion of different gene alteration types in the PTC group and benign group (%). PTC: papillary thyroid carcinoma. BTN: benign thyroid nodules.
Correlation between gene mutations and clinicopathological features
Patient demographic characteristics, pathologic features of papillary carcinomas, and gene mutation information of the PTC group were analyzed and are summarized in Table 4. Gene mutations in tumors were associated with a higher rate of LNM (P = 0.020) and thyroid capsular invasion (P = 0.045), a lower rate of coexisting HT (P = 0.016), younger age (<45 years) (P = 0.042), and the classical PTC (CPTC) subtype (P = 0.049). BRAFV600E mutations in tumors were associated with a significantly lower rate of coexisting HT (P < 0.001), a higher rate of thyroid capsular invasion (P = 0.018), and the CPTC subtype (P = 0.002). A trend of association was observed between BRAF mutations and a higher rate of LNM. We also compared the clinicopathological features of BRAFV600E-mutated PTC and RAS-mutated PTC to explore their differences. As shown in Supplementary Table 4, compared with RAS mutations in PTC, BRAFV600E mutations in PTC were correlated with significantly lower HT occurrence (P = 0.002) and a higher thyroid capsular invasion rate (P = 0.031).
Comparison of clinicopathological characteristics between patients with or without gene mutation and between patients with or without BRAF mutation.

LNM, lymph node metastasis; HT, Hashimoto’s thyroiditis, PTC, papillary thyroid carcinoma.
Statistically significant.
Association between LNM and clinicopathological characteristics or gene mutations
We performed univariate and multivariate analyses to identify risk factors for LNM. In the univariate analysis, LNM was associated with having gene mutations [odds ratio (OR) = 4.185, 95% confidence interval (CI): 1.188–14.746, P = 0.026], younger age (OR = 8.000, 95% CI: 2.764–23.152, P < 0.001), tumor size (OR = 3.652, 95% CI: 1.153–11.565, P = 0.028), and thyroid capsular invasion (OR = 3.649, 95% CI: 1.189–11.202, P = 0.024) (Table 5). In the multivariate analysis, only age younger than 45 years emerged as an independent risk predictor for a high incidence of LNM. The age distribution of the LNM group significantly differed from that of the non-LNM group (Wilcoxon–Mann–Whitney-test, P < 0.001) (Figure 4). In the age-group analysis, the BRAF mutation rate showed a significant association with LNM in the older age group (age ≥ 45 years) (P = 0.012) (Supplementary Table 5).
The association between LNM and clinicopathological characteristics or gene mutations in PTC.

LNM, lymph node metastasis; HT, Hashimoto’s thyroiditis; PTC, papillary thyroid carcinoma; OR, odds ratio; CI, confidence interval; NA, not applicable.
*Statistically significant.

Box and scatter plot showing the median and quartiles of age distribution of the LNM and non-LNM groups with papillary thyroid carcinoma. The horizontal axis indicates the groups with or without LNM; the vertical axis indicates age. The orange spots represent LNM samples and blue spots represent non-LNM samples. LNM: lymph node metastasis. Non-LNM: non-lymph node metastasis. *** indicates P < 0.001 (Wilcoxon–Mann–Whitney test).
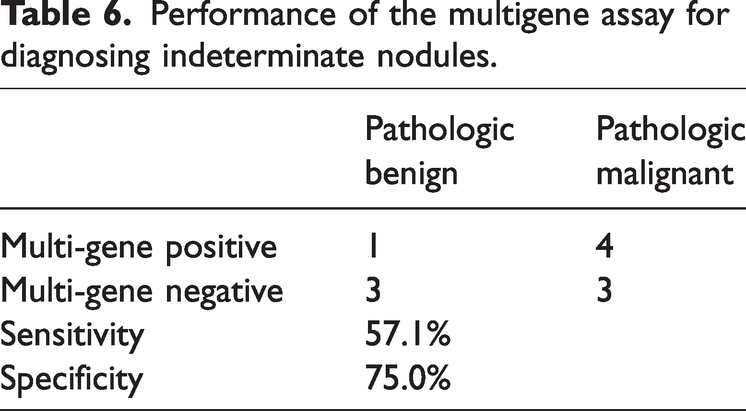
Performance of a multigene assay in diagnosing cytologically indeterminate nodules
Among all cytological diagnosis samples, we identified 15 nodules classified as Bethesda class III or class IV, indicating indeterminate nodules. Among these 15 nodules, 11 underwent diagnostic surgical procedures to obtain the final pathological diagnoses; 7 were identified as positive and 4 were identified as negative. The sensitivity and specificity of the multigene test for these 11 nodules were 57.1% and 75.0%, respectively (Table 6 and Supplementary Table 6).
Performance of the multigene assay for diagnosing indeterminate nodules.
Discussion
PTC has a relatively high mutation rate, particularly for genes in the MAPK pathway, such as RET/PTC rearrangement and point mutations of the BRAF and RAS genes. 25 In this study, we used a 22-gene assay including hot spot mutations, insertions and deletions, and gene rearrangements reported in PTC patients. Our findings revealed that the mutation rates detected in our cohort were consistent with those of previously published studies.26–28 Additionally, we observed a significant difference in the overall mutation rate between PTC and benign nodule patients, with rates of 79.7% and 21.6%, respectively. BRAF mutation was the most frequent mutation in the PTC group, and it was the only mutation that showed a significant difference between the PTC and benign groups. Multigene mutations were correlated with higher rates of LNM and thyroid capsular invasion, lower rates of coexisting HT, CPTC, and younger age in this study. BRAF mutation was associated with a lower HT incidence, a higher capsular invasion rate, and CPTC, a result that is generally consistent with previous reports. Recently, Liang et al. reported the genetic landscape of PTC in 355 Chinese individuals and found that kinase gene fusion was associated with younger age, larger tumor size, and LNM. 27 Tang et al. reported an analysis based on 117 PTC patients and found that mutations other than BRAFV600E were significantly related to poor prognosis. 29 Deng et al. found that BRAFV600E was associated with older age and was an independent risk factor for extrathyroidal extension (ETE) but not LNM, while RET/PTC rearrangement suggested increased LNM in young patients with PTC. Additionally, the combination of BRAFV600E with other gene mutations indicated a higher rate of ETE, which suggested greater aggressiveness of PTC. 30 Comparison of the clinicopathologic features of BRAFV600E-mutated PTC with those of RAS-mutated PTC showed that BRAFV600E mutation was significantly associated with a lower incidence of HT and a higher rate of thyroid capsular invasion, suggesting that PTC with BRAFV600E mutation tends to exhibit a more aggressive behavior, a finding that aligns with prior studies.31,32
There are also conflicting findings in previous studies regarding the relationship between mutations and clinicopathological factors; for example, some meta-analyses reported associations between BRAFV600E mutation and factors such as tumor multifocality, thyroid capsular invasion, ETE, LNM, and advanced stage,33,34 while another study found no association between BRAF mutations and any clinicopathological factors. 35 Alternatively, the same mutations, including BRAFV600E, may be associated with various clinicopathological factors in different studies. Similar controversies exist for other genes. These discrepant results may stem from differences in methodology, including group selection, group size, follow-up duration, and statistical analyses. The good prognosis of PTC patients makes it relatively challenging to gather sufficient information, such as overall survival rates, to study the relationship between mutations and prognosis. However, additional studies will provide valuable information to understand the relationship between mutations and PTC. Future research should prioritize large-scale studies with longer follow-up periods and standardized criteria for assessment to evaluate the relationship between mutations and PTC prognosis.
In this study, the correlation between mutation and younger age was a rare finding. In many tissue types, mutations accumulate steadily over time under normal circumstances, 36 and BRAF mutation, as the highest-rate mutation in PTC, has consistently shown a close correlation with older age.30,37 Although kinase gene fusion was reported to be correlated with younger age in PTC, 27 in the present study, RET fusion did not show any age trend, and the correlation between multigene mutations and younger age was interesting in this context. In addition, subgroup analyses revealed that younger age was an independent risk factor for LNM, which is also an interesting finding. Generally, older age is considered a negative factor for PTC prognosis, and patients younger than 45 years old are deemed to have low-risk disease and a favorable prognosis, even when faced with advanced locoregional thyroid cancer.38,39 These results suggest the relationship between PTC prognosis and age as a factor that should be reassessed through further research. In the subgroup aged ≥ 45 years, BRAF mutation had a significant association with LNM, and this tendency was not shown in the younger age group, which is similar to the results of a previous study. 40 This result suggests that a BRAF mutation test may be meaningful for PTC prognosis in older age groups, whereas other gene mutations may play a more meaningful role in younger populations.
FNAB is commonly used as a preoperative diagnostic tool for thyroid nodules. However, approximately 20% of nodules remain indeterminate even after FNAB diagnosis, with a malignant risk ranging from 10% to 40%.41,42 Enhancing the diagnostic accuracy of indeterminate nodules is crucial. Molecular testing has emerged as an important clinical tool, with approximately one-third of indeterminate thyroid nodule patients opting for molecular testing in the United States.43,44 Studies have shown that molecular tests, such as DNA-RNA tests (Thyroseq V3, multigene genomic classifier) and RNA tests (GSC, Afirma genomic sequencing classifier), can help a significant number of patients with indeterminate nodules avoid unnecessary diagnostic surgery. 41 However, these tests have limitations such as low specificity, high overdiagnosis rates, limited detection capabilities, and high costs. The diagnostic performance of the 22-gene test used in our study may require further verification, but it holds promise in providing useful information to improve subsequent management of indeterminate nodules. For example, the presence of BRAF mutations in a nodule sample may suggest the need for more aggressive clinical strategies, and RAS mutation is a low accuracy marker for PTC diagnosis.
Our study has some limitations. The sample size of the nodules analyzed was limited, which could impact the evaluation of the relationship between multigene alterations and clinicopathological features. Additionally, some benign nodules in our study only underwent FNAB cytological diagnosis and lacked tissue histopathologic confirmation, which may have reduced the accuracy of our findings to some extent.
In conclusion, the correlations between multigene alterations and clinicopathological features in PTC were investigated and the diagnostic potential of gene mutation detection in uncertain thyroid nodules was explored in this study, which may be very helpful for the investigation of driver genes in PTC and contribute to improved PTC management.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241233166 - Supplemental material for Correlation between genetic alterations and clinicopathological features of papillary thyroid carcinomas
Supplemental material, sj-pdf-1-imr-10.1177_03000605241233166 for Correlation between genetic alterations and clinicopathological features of papillary thyroid carcinomas by Shixuan Shang, Huimin Yang, Meixiang Chen, Jin Wu, Xianjun Shi, Xiangqin Li, Ningning Feng, Zhaoqing Zheng, Hongmei Liu and Yunzhi Zhang in Journal of International Medical Research
Footnotes
Acknowledgements
The authors are grateful to Shunlin Zhao, Qinfu Wang, Ling Wang, and Rong Zhou for their help with the enrollment of patients in this study.
Author contributions
Conception and design: S Shang, H Yang, M Chen Administrative support: S Shang Provision of study materials or patients: M Chen, J Wu, X Shi Collection and assembly of data: M Chen, J Wu, X Shi, X Li Data analysis and interpretation: S Shang, H Yang, N Feng, Z Zheng, H Liu, Y Zhang Manuscript writing: All authors Final approval of the manuscript: All authors
Declaration of conflicting interests
Huimin Yang, Ningning Feng, Zhaoqing Zheng, Hongmei Liu, and Yunzhi Zhang declare their employment relationship with the NGS company Shanghai Singlera Medical Laboratory, which performed the sequencing work for this study. The remaining authors have no potential conflicts of interest to declare.
Ethics approval and consent to participate
Approval for this study was obtained from the ethics committee of The First People’s Hospital of Jiangxia District (No. 2021019). Written informed consent was obtained from all individual participants included in the study.
Funding
This work was supported by the Research Program of Wuhan Municipal Health and Family Planning Commission [WH21Z40].
Supplementary Material
Supplementary Table 1. Hot spot gene mutations in the OncoAim® kit
Supplementary Table 2. Information on gene fusions in the OncoAim® kit
Supplementary Table 3. Information on mutations and clinicopathologic features in papillary thyroid carcinoma and benign nodules
Supplementary Table 4. Comparison of the clinicopathologic features of BRAFV600E-mutated papillary thyroid carcinoma with those of RAS-mutated papillary thyroid carcinoma
Supplementary Table 5. Correlation analysis of mutations and clinicopathological features in the older age (≥45 years) subgroup
Supplementary Table 6. Gene mutation list of indeterminate nodules
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.