
Abstract
Cervical lymph node metastasis in patients with differentiated thyroid cancer affects postoperative recurrence and survival. Hypoparathyroidism is caused by parathyroid gland injury during thyroidectomy. Carbon nanoparticles can trace stained lymph nodes, aiding in thorough dissection of lymph nodes in the operation area. To reduce postoperative occurrence of hypoparathyroidism, the parathyroid glands and their functions (identified by negative imaging induced by carbon nanoparticles) are retained in situ. However, the safety and adverse effects of nanocarbon suspension in thyroid surgery have rarely been evaluated. In this report, we describe a patient with thyroid cancer who had carbon secretions in the trachea caused by nanocarbon suspension when tracheal intubation was performed under general anesthesia, and the inflatable balloon surface of the tracheal tube was covered with these secretions. The patient recovered without fever, cough, phlegm production, chest pain, hoarseness, or hypocalcemia-induced convulsions. No consensus has yet been reached on the most appropriate injection site, depth, dose, or waiting time for nanocarbons in thyroid cancer surgery. We believe that nanocarbon suspension is safe for use in thyroid cancer surgery, but the most appropriate injection depth should be based on the thickness of the thyroid gland tissue to avoid deep injection into the trachea.
Keywords
Introduction
Thyroid cancer is the most common malignant endocrine tumor. The incidence of papillary thyroid carcinoma (PTC) accounts for more than 85% of all thyroid cancers, and its incidence is increasing. 1 Lymph node metastasis can occur in the early stages of PTC,2,3 and it has an impact on the prognosis and recurrence. 4 Therefore, thyroidectomy combined with regional lymph node dissection for PTC has gained recognition. 5 However, improvement in the detection rate of the suspected lymph nodes and a decrease in the incidence of postoperative hypoparathyroidism is challenging for thyroid surgeons.
Nanocarbons, through their identification and staining of lymph tissue, can improve the detection rate of lymph nodes and metastatic lymph nodes. The morphology and function of the parathyroid glands can be identified and retained in situ by negative parathyroid imaging, thus reducing the occurrence of hypoparathyroidism after the operation.4,5 However, a few adverse effects have been reported. 6 In clinical practice, we encountered a patient with thyroid cancer who developed carbon secretions in the trachea caused by infiltration of nanocarbon suspension during the operation.
Case report
A 56-year-old man was admitted to the hospital 1 week after a left thyroid nodule was discovered during a physical examination. Color Doppler ultrasonography revealed a hypoechoic area approximately 1.2 × 0.8 cm in size in the central portion of the left thyroid gland. The area had unclear boundaries with the surrounding tissues, an irregular shape, aspect ratio imbalance, and fine sand calcification, and its TI-RADS grade was 4B. Fine needle aspiration cytology of the left thyroid nodule suggested papillary thyroid cancer. Preoperative thyroid function and serum calcium and phosphorus levels were within the normal range.
Surgical treatment was performed under general anesthesia on 14 June 2019. The patient was placed in the supine position and intubated under general anesthesia. The intubation process was smooth, and no abnormal secretions were found in the mouth, pharynx, or larynx. Shoulder pads were used to fully expose the neck. A low neck arc incision was made to separate the skin flaps and expose the thyroid glands. Using a 1-mL skin test syringe, nanocarbon suspension (H20041829; Chongqing LUMMY Pharmaceutical Co., Ltd., Congqing, China) was injected with a perpendicular orientation into the two upper and lower poles of the left thyroid gland to about 4 mm in depth. A total of 0.2 mL was slowly injected at each point, confirming the site before injection and avoiding injection into the blood vessels. The syringe was retrieved, and the injection point was pressed with gauze to prevent nanocarbon spillage from affecting the operation. Left thyroid gland lobectomy and left central lymph node dissection were performed 10 minutes after injecting the nanocarbon suspension. The operation area was then rinsed with warm saline to check that the trachea was intact. No bubbles were found in the operation area after checking with an artificial tympanic lung. No obvious diverticulum was found in the exposed trachea after the radical operation for left thyroid cancer, and no thyroglossal cyst or fistula was found after anterior laryngeal lymph node dissection. A drainage tube was placed in the operation area, and the incision was sutured layer by layer. The procedure was smooth. When the tracheal tube was retrieved, a large amount of carbon-containing secretions was found in the patient’s mouth, and the inflatable balloon surface of the tracheal tube was covered with these secretions (Figures 1 and 2(a)). The secretions in the mouth were suctioned as much as possible with a sputum suction tube. The patient recovered smoothly and had no carbon-containing secretions after the operation. The drainage tube drained a small amount of reddish exudate and was removed on the second postoperative day. No fever, cough, sputum production, chest pain, hoarseness, or hypocalcemia-induced convulsions were noted after the operation. The serum calcium and parathormone levels were within the normal range. The patient was discharged on the third postoperative day. At the time of this writing, he was still undergoing follow-up without signs of discomfort.

The inflatable balloon surface of the patient’s tracheal tube was covered with carbon secretion.
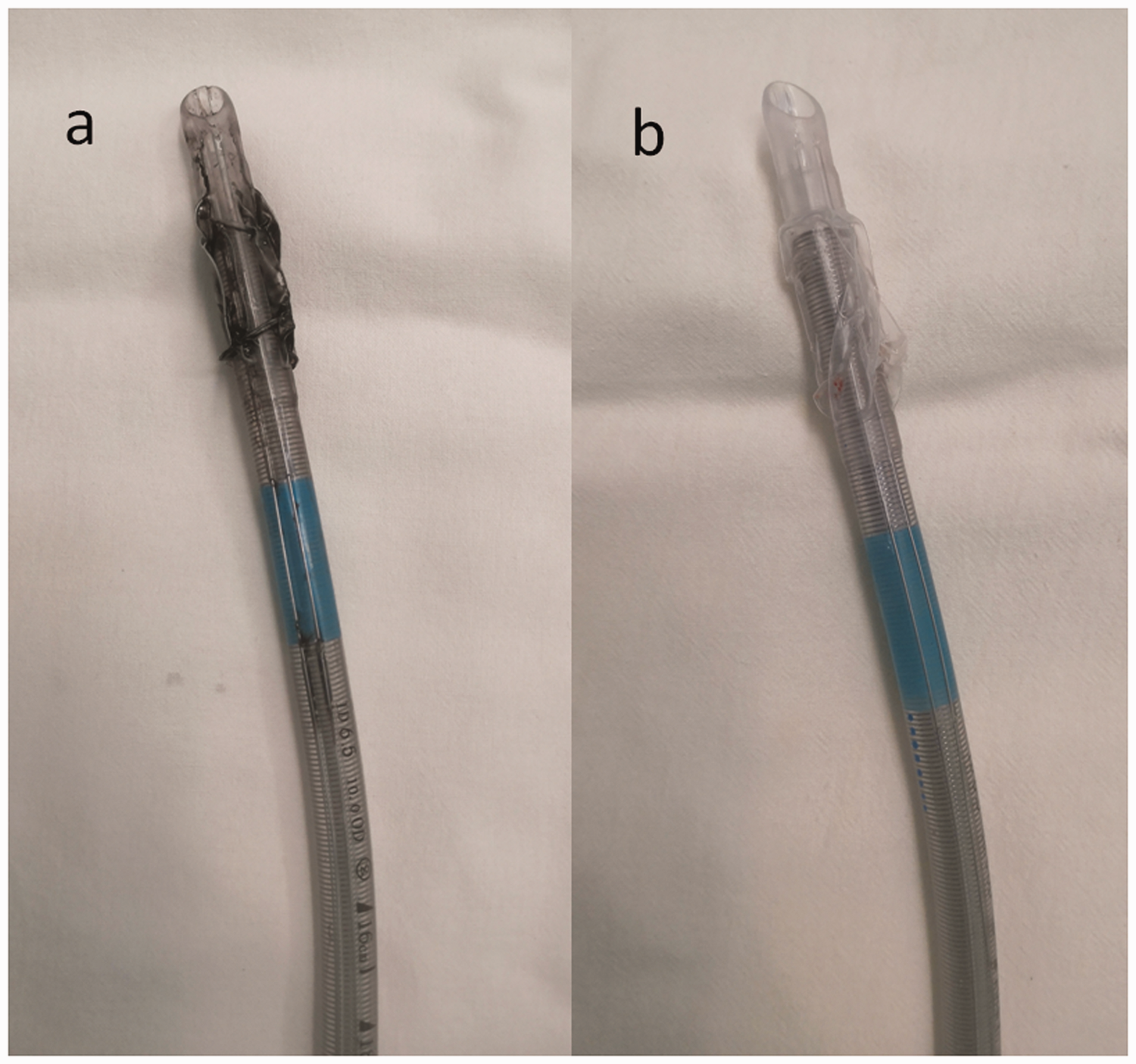
(a) The inflatable balloon surface of the patient’s tracheal tube was covered with carbon secretion. (b) Normal tracheal intubation for comparison.
Discussion
This report describes the case of a 56-year-old man with thyroid cancer who developed carbon secretions in the trachea caused by infiltration of nanocarbon suspension during the operation.
PTC accounts for more than 85% of all thyroid cancers, 1 and lymph node metastasis can be present in 20% to 90% of patients with PTC at the time of the initial diagnosis.2,3 Cervical lymph node metastasis in patients with thyroid cancer is an important factor that affects recurrence and survival 4 ; thus, pathological thyroidectomy combined with regional lymph node dissection is the main treatment of PTC. 5 The incidence of permanent hypoparathyroidism after total thyroidectomy combined with central lymph node dissection ranges from 1.4% to 14.3%. 7 The incidence of hypocalcemia caused by hypoparathyroidism can be as high as 9.9% to 20.8%8,9 and reduces the patient’s quality of life. Thus, it is particularly important to identify a method that can effectively remove lymph nodes and preserve the parathyroid glands.
As a new type of lymphatic tracer, carbon nanoparticles have been widely used in gastric cancer, colorectal cancer, and breast cancer surgeries and have achieved ideal results.10–12 In recent years, nanocarbon has been gradually applied in thyroid cancer surgery. 4 Carbon nanoparticles are 150 nm in diameter, smaller than the lymphatic endothelial cell gap (500 nm) and larger than the capillary endothelial cell gap (30–50 nm). Therefore, carbon nanoparticles can enter lymphatic vessels and lymph nodes after being swallowed by macrophages, facilitating identification of lymph nodes by black staining; however, these particles do not enter the parathyroid glands because of the absence of a lymphatic connection between the thyroid and parathyroid glands, so the parathyroid gland remains unstained and thus protected.4,5 Studies have shown that the use of nanocarbon can detect lymph nodes, aiding in thorough dissection of the lymph nodes in the operative area and increasing the detection rate of lymph nodes and metastatic lymph nodes. Moreover, by negative imaging of the parathyroid glands, their morphology and function can be well recognized and preserved in situ, thus reducing the occurrence of hypoparathyroidism after the operation.1,4,5,13 In addition, the use of carbon nanoparticles can significantly reduce the incidence of parathyroid gland injury during the second operation for thyroid cancer. 14
Nanocarbons are reportedly safe for use in gastric cancer surgery. 10 No allergies, toxic adverse effects, or safety concerns have been reported. To the best of our knowledge, there is no consensus on the most appropriate injection site, dosage, or waiting time of nanocarbons. Most clinicians inject the suspension in two to four points around the tumor, avoiding injection into the tumor. 4 The total injection volume ranges from 0.2 to 0.5 mL (0.1 to 0.2 mL per point), with a waiting time of 10 to 20 minutes after injection for surgery. 4 Although a few articles have mentioned the injection depth, this depth is not the same among different reports; some surgeons inject the suspension into the superficial thyroid gland to a depth of 2 to 3 mm, while others inject the suspension more deeply into the thyroid gland to no definite depth.15,16 In the present case, two injection points around the tumor were selected, the total injection volume was 0.4 mL, and the waiting time was 10 minutes; these parameters are consistent with those reported in the literature. 4 When the tracheal tube was retrieved after the operation, some carbon-containing secretions were present in the mouth, and the inflatable balloon surface of the tracheal tube was covered with these secretions. This has three possible explanations. First, thyroid neoplasms are located in the middle pole, and nanocarbon is injected into the upper pole of the thyroid. The gland was thin in our patient; his preoperative color Doppler ultrasound images showed that the thickness of the upper and lower poles of the left thyroid gland was about 0.5 cm. Therefore, the syringe needle with an injection depth of 0.4 cm might have penetrated the gland and trachea or the tracheal mucosa, causing direct entry or infiltration of nanocarbon into the tracheal cavity through the mucosa. However, the trachea was carefully examined during the operation. No surgical wounds were found on the surface, and no air bubbles were found in the operation area as checked using an artificial tympanic lung. The drainage tube was well sealed after the operation. However, we could not exclude the possibility of a pinhole in the trachea because such a hole is very difficult to identify. Second, the interaction between the thyroid lymphatic vessels and lymphatic capillary networks of the tracheal mucosal layers may have contributed to a small amount of carbon nanoparticle leakage. Theoretically, an abnormal lymphatic structure (which was difficult to confirm in this patient) might be one cause of such a large amount of carbon nanoparticle leakage. Third, inadvertent injection into a possible tracheal diverticulum, thyroglossal cyst, or fistula can also cause carbon-containing secretions. However, our patient had no obvious tracheal diverticulum, thyroglossal cyst, or fistula on his preoperative neck computed tomography scan, which was consistent with the intraoperative exploration. Actually, a thyroglossal cyst is located in the anterior central region of the neck, so the possibility of injecting carbon nanoparticles into a thyroglossal cyst was very small in this patient with left thyroid cancer.
The manufacturer’s manual for the nanocarbon suspension indicated that adverse reactions are rare and include an occasional low-grade fever after the injection; however, our patient did not develop a fever after the operation. He recovered smoothly after the operation with no respiratory symptoms, such as fever, cough, sputum production, chest pain, hoarseness, hypocalcemia-induced convulsions, or other discomforts.
In conclusion, this case suggests that nanocarbon suspension is safe for use in thyroid cancer surgery. However, the most appropriate injection depth should be selected according to the thickness of the thyroid gland to avoid deep injection into the trachea.
Footnotes
Authors’ contributions
L-BZ drafted this manuscript. FZ and P-BZ was involved in acquisition of the data and preparation of the figures. P-FL conceived of the study and revised the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
All data and materials are freely available upon request. For further information, please contact Dr. Peng-fei Li (nbblyy1288@sina.com), who is responsible for the dataset.
Consent for publication
Beilun District People’s Hospital obtained the patient’s consent for publication of his individual data.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The Ethics Committee of Beilun District People’s Hospital approved this study. The analysis was performed in accordance with the ethical standards of the hospital and the tenets of the Declaration of Helsinki/Declaration of Istanbul. The patient described in this study provided written informed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for profit sectors.