
Abstract
Nocardia pseudobrasiliensis is a new taxon constituting an emerging species of human pathogenic Nocardia, which shares morphological features with N. brasiliensis. However, N. pseudobrasiliensis is more invasive and more easily disseminated, and it exhibits distinctive antibiotic susceptibility. Few clinical cases related to N. pseudobrasiliensis infection have been reported, and N. pseudobrasiliensis hydrarthrosis has not been described. Here, we analyzed the case information, diagnostic process, treatment, and prognosis of a patient with N. pseudobrasiliensis hydrarthrosis who received treatment in Zhejiang Provincial People's Hospital. Magnetic resonance imaging showed joint cavity effusion and soft tissue swelling with high signal on proton density-fat saturated images and low signal on T1-weighted images. Oil microscopy revealed abundant acid-fast–positive filaments in hydrarthrosis puncture fluid. The pathogen was identified as N. pseudobrasiliensis by matrix-assisted laser desorption ionization–time of flight mass spectrometry. In contrast to the 100% ciprofloxacin resistance displayed by N. brasiliensis, this clinical isolate of N. pseudobrasiliensis was completely susceptible. In summary, this is the first report of N. pseudobrasiliensis in joint effusion from a patient with arthritis.
Keywords
Introduction
Nocardiosis, occurring primarily in immunocompromised patients, is a local or disseminated infection caused by obligate aerobic actinomycetes in the genus Nocardia. 1 This genus has undergone rapid taxonomic expansion, such that more than 100 subtypes and approximately 30 human pathogens have been identified thus far.2,3 Nocardia pseudobrasiliensis is a new taxon constituting an emerging species of human pathogenic Nocardia; it was genotypically characterized by Ruimy et al and previously considered a member of Nocardia brasiliensis based on its phenotype. 4 Although N. pseudobrasiliensis shares morphological features with N. brasiliensis, it has nitrate reductase and adenine decomposition activities, which enable greater invasiveness and dissemination, along with distinctive antibiotic susceptibility. 5 Thus far, fewer than 10 clinical cases related to N. pseudobrasiliensis infection have been reported; most reports have described Nocardia pneumonia, cutaneous nocardiosis, and disseminated nocardiosis. 6 To our knowledge, there have been no reports of N. pseudobrasiliensis hydrarthrosis. Here, we describe a man in his 70s who presented with N. pseudobrasiliensis-induced left hydrarthrosis and a 7-year history of systemic lupus erythematosus (SLE).
Case presentation
Clinical features
This report was written in accordance with the CARE guidelines. 7 A man in his early 70s experienced left hip pain without an apparent cause, numbness, or skin redness. Nearly 5 months later, he presented to a local hospital for redness and swelling in the left knee; he received injections of the antibiotics piperacillin sodium and tazobactam sodium, as well as oral treatment with the antiviral entecavir. One month later, the redness and pain in his knee had not improved. For further assessment, the patient was referred to Zhejiang Provincial People's Hospital. He reported a 7-year history of SLE characterized by abnormally low lymphocyte counts; he had taken prednisone 15 mg daily for more than 6 months, but he had not received other treatments. The patient's laboratory results suggested that he was a carrier of hepatitis B virus, and he had a history of recurrent oral ulcers. Otherwise, he had no other infectious diseases and no histories of surgery, trauma, allergies, or clinically significant family genetics. The patient had normal body temperature (37.1°C), normal respiration (18 breaths/minute), good mental status, soft abdomen, rough breath sounds in both lungs, no rales, no tenderness, and no rebound pain. Laboratory analysis showed increases in white blood cells (12.68 × 109/L) and neutrophils (95.6%), along with decreases in lymphocytes (2.0%), monocytes (2.2%), hemoglobin (105 g/L), red blood cells (3.43 × 1012/L), and C-reactive protein (52.4 mg/L). Biochemical function tests revealed an increased ratio of urea nitrogen to creatinine (31.52), and routine urinalysis indicated the presence of urine protein (Table 1). Magnetic resonance imaging showed joint cavity effusion and soft tissue swelling with low signal on T1-weighted images and high signal on proton density-fat saturated images (Figure 1).
Clinical assessments and laboratory results.
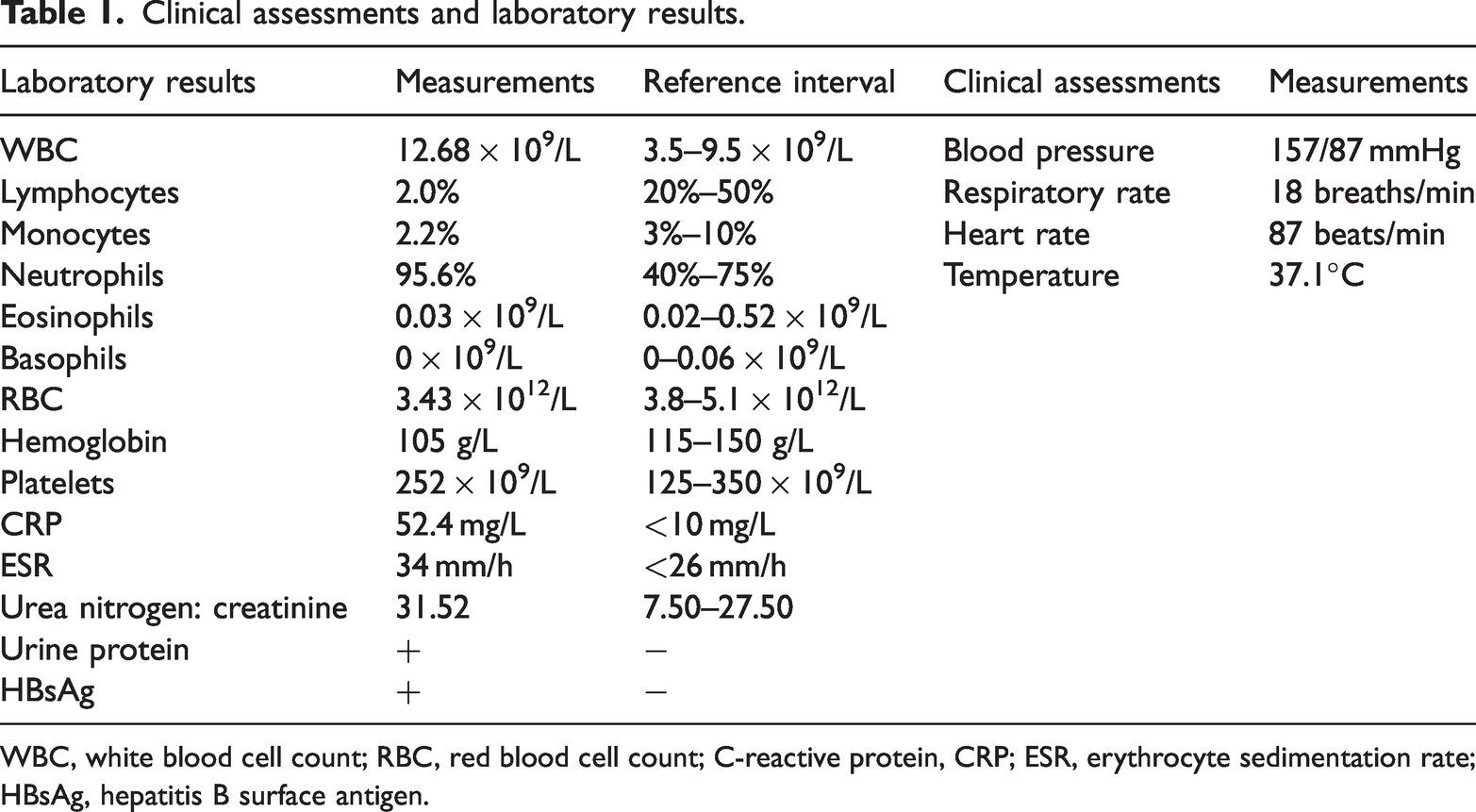
WBC, white blood cell count; RBC, red blood cell count; C-reactive protein, CRP; ESR, erythrocyte sedimentation rate; HBsAg, hepatitis B surface antigen.

Magnetic resonance imaging showed joint cavity effusion and soft tissue swelling with low signal on T1-weighted images and high signal on proton density-fat saturated images (arrows). LAI, left anterior inferior; LPI, left posterior inferior; RAI, right anterior inferior; RPS, right posterior superior.
Etiological investigation
Acid-fast staining of hydrarthrosis puncture fluid was performed, and oil microscopy revealed red acid-fast–positive filaments (Figure 2a). The pathogen was identified as N. pseudobrasiliensis via matrix-assisted laser desorption ionization–time of flight mass spectrometry (bioMérieux, France) (Figure 2b). The maximum zone of inhibition of the N. pseudobrasiliensis isolate, upon exposure to trimethoprim/sulfamethoxazole, was determined by the Kirby–Bauer method. The minimum inhibitory concentrations of amoxicillin/clavulanic acid, clindamycin, ciprofloxacin, imipenem, amikacin, linezolid, and levofloxacin against N. pseudobrasiliensis were determined by the Epsilometer test. The isolate was sensitive to all tested antibiotics, according to standard drug susceptibility assays. 8 (Table 2)

Pathology findings. (a) Oil microscopy revealed acid-fast–positive filaments in hydrarthrosis puncture fluid (×1000 magnification). (b) Matrix-assisted laser desorption ionization–time of fight mass spectrometry confirmed the presence of Nocardia pseudobrasiliensis. Da, Daltons; MV, megavolts.
Nocardia pseudobrasiliensis antimicrobial susceptibility according to Kirby–Bauer method and Epsilometer test.
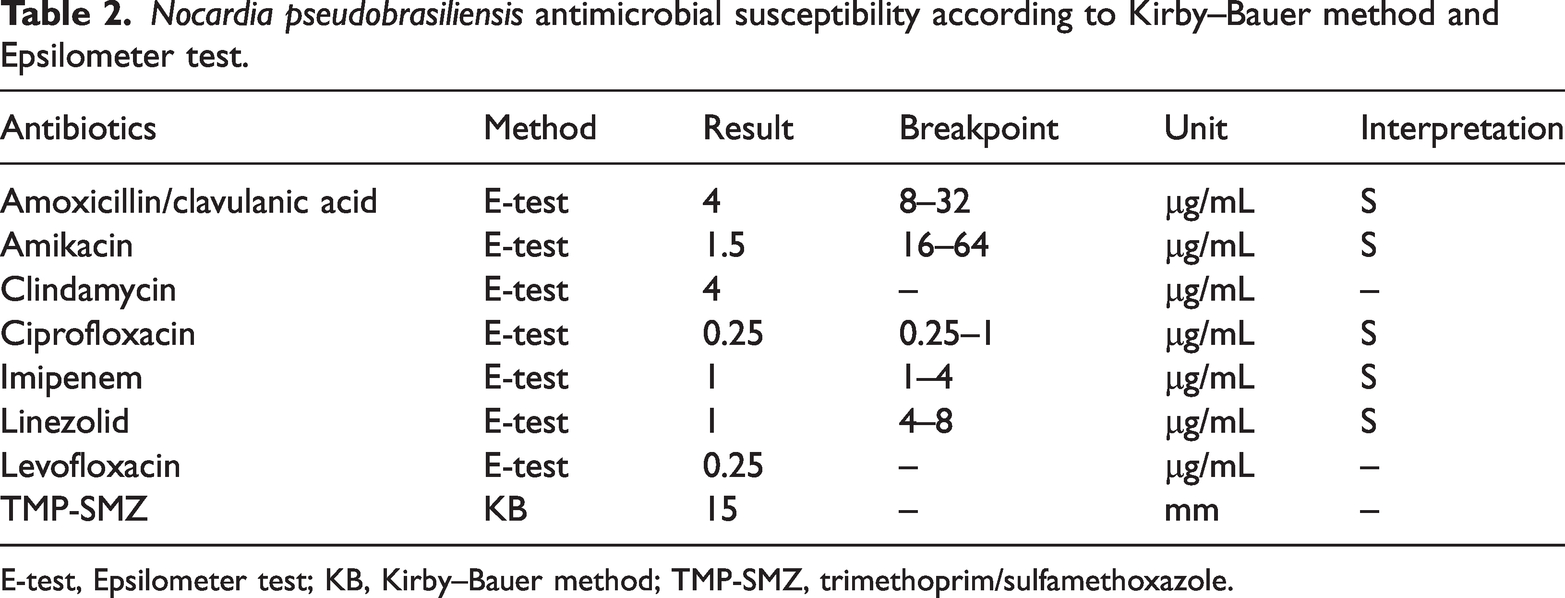
E-test, Epsilometer test; KB, Kirby–Bauer method; TMP-SMZ, trimethoprim/sulfamethoxazole.
Treatment and prognosis
The patient underwent debridement and drainage of the knee joint. A 1-cm incision was made at the front of the left knee. The inner side of the incision was repeatedly washed with normal saline using a 50-mL syringe; yellow pus was expelled, and two drainage tubes were placed. The wound was washed again with normal saline, the drainage tubes were sutured and fixed, and the wound was bandaged with compression. Antibiotic treatment was administered by intravenous infusion of amoxicillin sodium/clavulanate potassium (1.2 g, every 8 hours) and levofloxacin (100 mL, twice daily). The patient's symptoms were alleviated and he returned to the local hospital for subsequent treatment.
Discussion
Studies have shown that more than half of apparent N. brasiliensis isolates associated with pulmonary or disseminated infections belong to a new taxon known as N. pseudobrasiliensis4,9; however, cases of N. pseudobrasiliensis infection are rare. N. brasiliensis is a common cause of opportunistic infection in immunocompromised patients, and its clinical presentation typically comprises cutaneous nocardiosis.10–13 However, according to published reports,14–21 N. pseudobrasiliensis has nitrate reductase and adenine decomposition activities, which lead to greater invasiveness and dissemination, as well as distinctive antibiotic susceptibility, compared with N. brasiliensis. N. pseudobrasiliensis can be distinguished from N brasiliensis by 16S rRNA gene sequencing, adenine hydrolysis, and nitrate reductase analysis; however, these methods can be time-consuming, expensive, and inconvenient. Here, we obtained accurate results by conducting aseptic culture of the patient’s hydrarthrosis puncture fluid and subjecting colonies to matrix-assisted laser desorption ionization–time of flight mass spectrometry identification. Although this method has been used to identify N. brasiliensis, a more complete commercial database is needed for the identification of rare Nocardia spp. 22 The N. pseudobrasiliensis isolate obtained in this case was susceptible to trimethoprim/sulfamethoxazole, amikacin, ciprofloxacin, clindamycin, imipenem, amoxicillin/clavulanic acid, linezolid, and levofloxacin. N. brasiliensis is resistant to ciprofloxacin3,5; thus, ciprofloxacin can be used to control N. pseudobrasiliensis but not N. brasiliensis. Our patient had a 7-year history of SLE, and long-term use of the glucocorticoid prednisone presumably had increased the risk of Nocardia infection. Furthermore, the patient’s arthritis symptoms indicated immunosuppression. Therefore, opportunistic pathogen monitoring should be performed in patients with immune disorders.
Currently, there are strict criteria for the diagnosis of SLE. The patient in this case had been diagnosed with SLE 7 years prior to his visit to our hospital, but he did not show characteristic symptoms of SLE during the course of N. pseudobrasiliensis infection; his symptoms solely comprised immune dysfunction. Therefore, we inferred that the patient had previously met the criteria for a diagnosis of SLE. Nevertheless, Nocardia prevention and treatment efforts should be extended to all immunocompromised patients, rather than solely focusing on patients with SLE.
In conclusion, we have reported the first case of N. pseudobrasiliensis hydrarthrosis in a Chinese patient with arthritis. The N. pseudobrasiliensis isolate obtained in this case was susceptible to ciprofloxacin, whereas previous reports have shown that N. brasiliensis is resistant to ciprofloxacin. There is a need to emphasize awareness of N. pseudobrasiliensis as an emerging human pathogen in immunocompromised patients. Antibiotic use should be guided by drug sensitivity results to prevent further clinical deterioration.
Footnotes
Acknowledgements
We thank our colleagues and mentors for their support.
Author contributions
YJ, MC, XH, LP, and DC collected the patient’s clinical information and analyzed the data. YG wrote the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
All relevant data are provided in this article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
This study was approved by the Ethics Committee of Zhejiang People's Hospital (Approval No.: 2022JS008) and was conducted in accordance with the ethical standards of the Declaration of Helsinki. This case report and all images were published with written informed consent from the patient. All identifying information has been anonymized in the report.
Funding
This study was supported by the New Project of Zhejiang Provincial People's Hospital, entitled “Construction of Rapid Nucleic Acid Detection Platform for Invasive Fungi” (20211214).