
Abstract
Campylobacter fetus is a Gram-negative bacillus typically associated with bacteremia in immunocompromised patients. Prosthetic valve endocarditis (PVE) is a serious complication of prosthetic valve surgery, with a high mortality rate if not treated promptly. We present a rare case of PVE caused by C. fetus. A man in his mid-60s presented to the Emergency Department with a fever and showed elevated C-reactive protein concentrations. He had prosthetic mitral and aortic valve replacement surgery 15 years previously. Gram-negative rods were detected in a blood culture. These rods were identified as C. fetus using matrix-assisted laser desorption ionization time-of-flight mass spectrometry and confirmed by 16S rRNA sequencing. The patient was treated with gentamicin and imipenem, and underwent valve replacement surgery. C. fetus was isolated in a left atrial appendage swab obtained during the surgery. Follow-up blood cultures were negative after treatment. However, after a cardiac arrest event, the patient’s general condition deteriorated, and he died. To the best of our knowledge, this is the first case of PVE caused by C. fetus in Korea and the second fatality to date. This case highlights the importance of considering C. fetus as a potential cause of PVE, even in patients without known risk factors.
Keywords
Introduction
Campylobacter fetus is a Gram-negative bacillus that can cause infection in immunocompetent patients, but it is more common and more serious in immunocompromised patients. 1 Prosthetic valve endocarditis (PVE) is a potential complication following prosthetic valve surgery, and if left untreated, it can result in a high mortality rate. 2 However, PVE caused by C. fetus is extremely rare, with only seven cases reported worldwide and one case reported in Asia (Table 1), all of which occurred in immunocompetent patients.2–9 The purpose of this report is to present the first case of PVE caused by C. fetus in Korea.
Previously reported cases of prosthetic valve endocarditis caused by Campylobacter fetus.
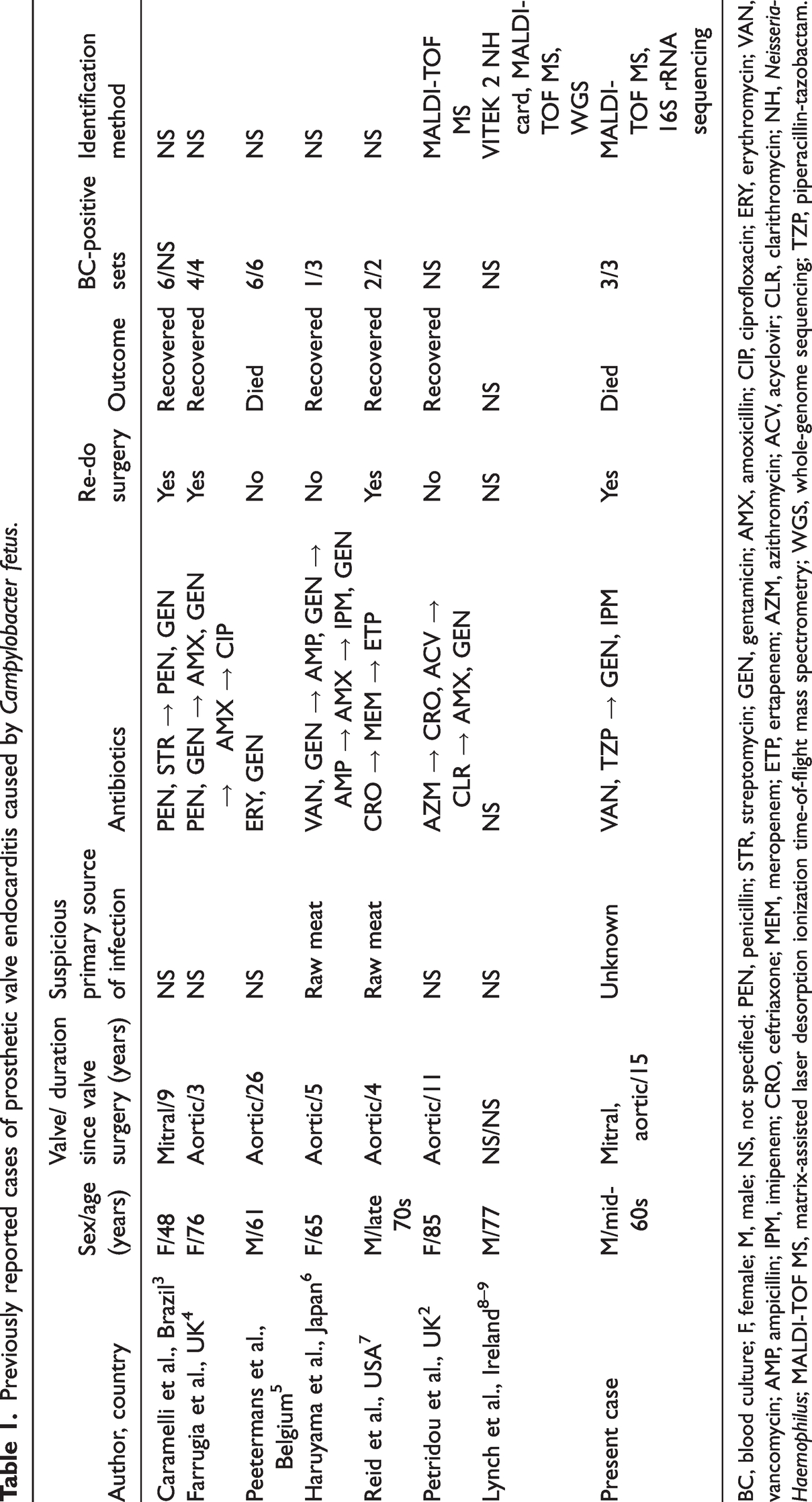
BC, blood culture; F, female; M, male; NS, not specified; PEN, penicillin; STR, streptomycin; GEN, gentamicin; AMX, amoxicillin; CIP, ciprofloxacin; ERY, erythromycin; VAN, vancomycin; AMP, ampicillin; IPM, imipenem; CRO, ceftriaxone; MEM, meropenem; ETP, ertapenem; AZM, azithromycin; ACV, acyclovir; CLR, clarithromycin; NH, Neisseria-Haemophilus; MALDI-TOF MS, matrix-assisted laser desorption ionization time-of-flight mass spectrometry; WGS, whole-genome sequencing; TZP, piperacillin-tazobactam.
Case presentation
A man in his mid-60s visited the Emergency Department of our hospital because of a persistent fever and elevated C-reactive protein concentrations that had continued for 3 weeks. Before this Emergency Department visit, the patient had visited another hospital when he developed a fever and took cefpodoxime, but there was no improvement in his condition. He was under follow-up at the Cardiothoracic Surgery Department after undergoing mechanical mitral and aortic valve replacement surgery 15 years previously for severe mitral valve stenosis and moderate aortic stenosis. His vital signs at admission were as follows: a blood pressure of 102/61 mm/Hg, heart rate of 73 beats/minute, respiratory rate of 20 breaths/minute, and body temperature of 36.7°C. Laboratory tests showed a hemoglobin concentration of 102 g/L, a white blood cell count of 15.18 × 109/L (neutrophils accounted for 84.4%), a platelet count of 249 × 106/L, and an elevated C-reactive protein concentration of 173.6 mg/L (reference range: 0–5 mg/L).
On Day 2 of Emergency Department admission, blood samples were taken from the peripheral veins and inoculated into BACTEC Plus Aerobic/F, Lytic/10, and Anaerobic/F (Becton Dickinson, Sparks, MD, USA) bottles, which were then cultured using the BACTEC FX system (Becton Dickinson). Three aerobic blood culture bottles showed positive results after 45, 48, and 49 hours, but no growth was observed on blood agar or MacConkey agar plates after aerobic culture at 35°C. However, 48 hours after anaerobic culture on Brucella agar plates under 10% H2, 10% CO2, and 80% N2 at 35°C, translucent round colonies formed. Identification using the VITEK 2 system (bioMérieux, Durham, NC, USA) with a Neisseria-Haemophilus card failed. The isolate was analyzed by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) using the microflex LT (Bruker Daltonics, Bremen, Germany). As a result of analysis with the MALDI Compass Library (DB9607, version 10.0) based on MALDI Biotyper Compass software 4.1 (Bruker Daltonics), the isolate was identified as C. fetus (score value: 2.460). To confirm this identification, 16S rRNA sequencing was performed using universal primers. To perform DNA amplification, 27F/1492R primers were used, and 785F/907R and 518F/800R primers were used for sequencing. The results were interpreted according to the Clinical and Laboratory Standards Institute guidelines. 10 As a result of searching the 16S rRNA base sequence in the GenBank database using the basic local alignment search tool algorithm, the isolate was 100% (1432/1432) identical to C. fetus (GenBank accession no.: MN661175.1) and 98.33% (1409/1433) concordant with C. hyointestinalis (GenBank accession no.: AF219235.1). Additionally, phylogenetic analysis using MEGA 11 software (https://www.megasoftware.net) showed a close relationship between the isolate and C. fetus (Figure 1a). Therefore, the isolate was conclusively identified as C. fetus.
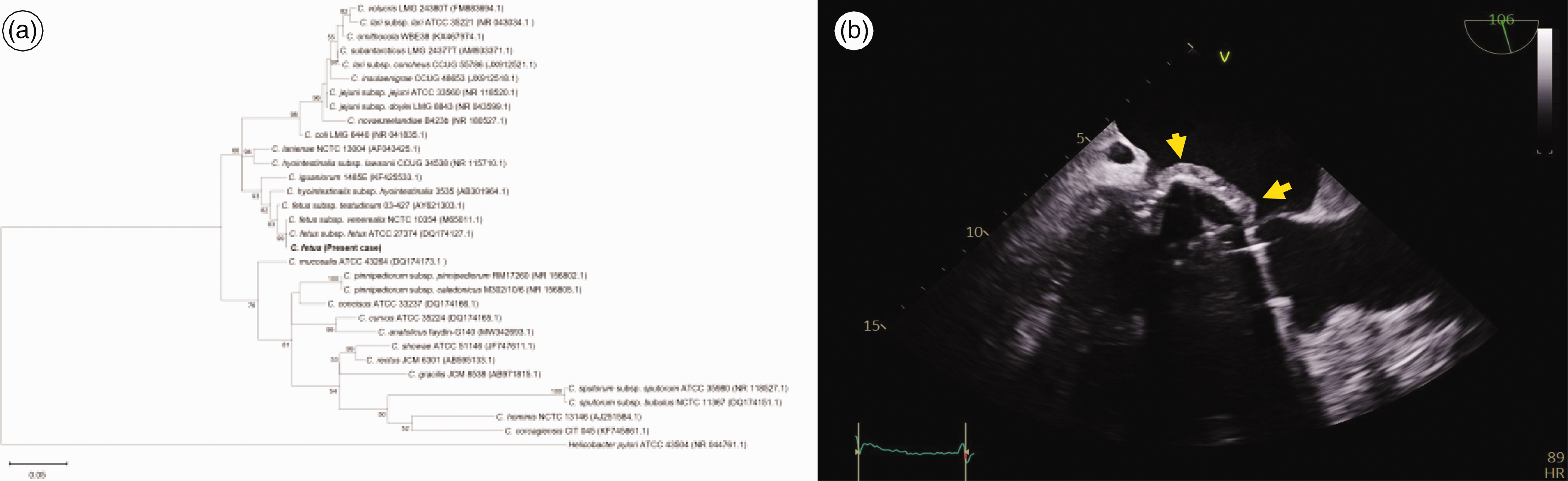
Phylogenetic analysis and transesophageal echocardiographic image of Campylobacter fetus. (a) Phylogenetic tree analysis of Campylobacter isolates (30 types and reference strains) based on 16S rRNA sequences (1507 nucleotide positions). The tree was constructed on the basis of the maximum likelihood method using the model GTR+I+G and Helicobacter pylori ATCC 43504 (NR 044761.1) as the outgroup. Bootstrap values are expressed as percentages of 1000 replications, and the scale bar indicates the estimated number of substitutions per base. GenBank database accession numbers are provided in parentheses. (b) Transesophageal echocardiography showing a suspicious vegetation around the mechanical mitral valve (arrows).
The minimum inhibitory concentrations (MICs) were determined by incubation under microaerobic conditions (5% O2, 10% CO2, and 85% N2) at 42°C for 48 hours on Brucella agar using Etest strips (bioMérieux, Marcy l’Etoile, France). Resistance or susceptibility could not be determined because there are no established breakpoints for interpreting antimicrobial susceptibility tests of C. fetus. However, vancomycin and piperacillin/tazobactam showed a high MIC of more than 256 μg/mL, while ceftriaxone, imipenem, meropenem, gentamicin, ciprofloxacin, and erythromycin showed low MICs (Table 2).
Antimicrobial susceptibility of the Campylobacter fetus clinical isolate from blood culture determined by the Etest.

MIC, minimal inhibitory concentration.
The patient was hospitalized on the day after his Emergency Department visit, and transesophageal echocardiography was performed on the same day. This technique showed suspicious vegetation around the mechanical mitral valve (Figure 1b). Vancomycin and piperacillin/tazobactam were started as empirical antibiotics for PVE. On Day 5 of hospitalization, the identification of C. fetus was confirmed, vancomycin and piperacillin/tazobactam were discontinued, and gentamicin and imipenem were administered. A prosthetic valve replacement operation was performed on Day 6 of hospitalization, and C-reactive protein concentrations decreased after the operation, but the white blood cell count continued to increase. On Day 11 of hospitalization, liver function tests showed elevated values, and gallbladder distention was observed on abdominal and pelvic computed tomography. Therefore, additional tests were planned to rule out acalculous cholecystitis. However, after cardiac arrest on Day 12 of hospitalization, the patient’s general condition deteriorated rapidly, and he died on Day 15.
Two peripheral venous blood cultures and two central venous blood cultures were performed on Day 4 of hospitalization. C. fetus was only found in the two central venous blood cultures. On Day 6 of hospitalization, preoperative blood cultures of peripheral and central venous blood cultures showed no growth. C. fetus was also observed in a smear culture of the left atrial appendage taken during the prosthetic valve replacement operation performed on the same day.
This case has been reported in accordance with the CARE guidelines. 11 All of the patient’s information has been anonymized.
Discussion and conclusions
The genus Campylobacter, consisting of Gram-negative rods that are small, slightly curved, or spiraled, is mostly found in animals. However, Campylobacter can also infect humans and cause several infectious diseases, such as gastrointestinal infections, bacteremia, abscesses, meningitis, osteomyelitis, and prosthetic joint infections, among others.1,12,13 Most of these diseases are self-limiting without antimicrobial treatment, and extraintestinal infections are uncommon in healthy individuals; however, they can occur in immunocompromised individuals, elderly individuals, and pregnant women. 1 While human infections caused by C. fetus are not common among the genus Campylobacter, C. fetus is one of the most common causes of Campylobacter bacteremia. 12 This finding is due to the affinity of C. fetus to the vascular endothelium, causing endovascular infections, such as mycotic aneurysms, thrombophlebitis, and infective endocarditis, including PVE. 5 C. fetus has three subspecies: C. fetus subsp. fetus, C. fetus subsp. testudinum, and C. fetus subsp. venerealis. The majority of human infections are caused by C. fetus subsp. fetus. 12 Untreated PVE caused by C. fetus is associated with a high mortality rate and can lead to various complications, such as septic emboli or perivalvular extension. 2
PVE occurring within 1 year of valve surgery is mainly caused by Staphylococcus aureus, while cases occurring 1 year or more after surgery are predominantly associated with viridans streptococci, HACEK bacteria (Haemophilus spp., Aggregatibacter spp., Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae), and rarely, fungal infections. 14 PVE can have various prognoses depending on the causative organism, but most infections cause complications, such as thrombosis, congestive heart failure, renal failure, arrhythmias, and conduction abnormalities. 14 Despite advancements in antimicrobial treatment and surgical techniques, the in-hospital mortality rate of PVE is still reported to be in the range of 22% to 29%.15,16
According to the Modified Duke criteria, 17 the patient met one major criterion with the presence of suspicious vegetation on transesophageal echocardiography. He had underlying heart disease and a fever of 38°C or higher. C. fetus is not a typical causative bacterium of endocarditis, but it was isolated in all three blood cultures of our patient. However, the patient met three minor criteria, leading to a clinical diagnosis of definite infective endocarditis. C. fetus was also identified in a swab specimen obtained from the left atrial appendage during prosthetic valve replacement surgery. However, the pathological criteria were not met because the tissue samples obtained during surgery were not cultured, and a histological examination for identifying microorganisms was not performed.
Because the genus Campylobacter has low metabolic activity and does not use carbohydrates, distinguishing it from other bacteria using phenotypic characteristics is challenging. 18 Although C. fetus is listed on the Neisseria-Haemophilus card of the VITEK 2 system, the instrument failed to identify this clinical isolate. MALDI-TOF MS is gaining attention as a potential replacement for the current microbial identification techniques used in clinical microbiology laboratories. 19 MALDI-TOF MS is used to quickly and accurately identify different species of Campylobacter. 18 A case of PVE in which C. fetus was identified by MALDI-TOF MS was previously reported, 2 which was the same in this case. Analyzing approximately 1060 base pairs is necessary for the species-level identification of Campylobacter spp. using 16S rRNA sequencing. 11 In our patient, the isolate was identified as C. fetus by sequencing, in accordance with reports that used the 16S rRNA sequencing technique. 20 The technique of 16S rRNA sequencing cannot distinguish between clinically important Campylobacter coli and Campylobacter jejuni. Therefore, the sequencing of rpoB, atpA, and cpn60 is required for accurately identifying the genus Campylobacter using molecular genetic techniques. 11
There are no established breakpoints for interpreting antimicrobial susceptibility tests of C. fetus. However, in this case, piperacillin/tazobactam and vancomycin showed high MICs, while ceftriaxone, imipenem, meropenem, gentamicin, ciprofloxacin, and erythromycin showed low MICs. Reports have shown that the antimicrobial susceptibility test of C. fetus isolated from fecal samples shows low MICs for ampicillin, gentamicin, and tetracycline. 21 Low MICs for imipenem, meropenem, gentamicin, and erythromycin were also observed in earlier cases of PVE caused by C. fetus.2,4,6,9
The cause and route of C. fetus infection are still unclear, but this infection is thought to occur after exposure to contaminated food from cattle and sheep, with predisposing factors such as immunosuppression and valve abnormalities. 12 Our patient was immunocompetent; therefore, how he became infected is unclear, and we assume that bacteremia caused by C. fetus contributed to his PVE and worsened systemic condition. His septic condition persisted irrespective of blood culture results, and the underlying atrial fibrillation worsened after surgery, leading to cardiac arrest occurring on Day 12 of hospitalization. We suspect that multiple organ failure due to deterioration in his overall physical function was the cause of death.
In this case, although no bacteria were detected in blood cultures after switching to the antimicrobial agents gentamicin and imipenem, the patient eventually died. Among previous cases of prosthetic valve endocarditis caused by C. fetus, only one patient, who visited the hospital 1 month after the onset of symptoms and did not seek treatment during that time, died (Table 1). 5 The similarities between these cases are the long duration since valve surgery and the delay between the onset of symptoms and the start of treatment. While our patient was evaluated at another hospital at the onset of fever, the use of inappropriate antimicrobial agents without identifying the organism at the time may have contributed to the poor prognosis. Even if a long duration since valve surgery contributes to a higher mortality rate, it is not a controllable factor. However, to obtain a better prognosis, presenting to the hospital early, identifying the organism, and receiving the appropriate antimicrobial therapy at the proper time may be particularly important.
To the best of our knowledge, this is the first case of PVE caused by C. fetus in Korea. C. fetus was identified using MALDI-TOF MS and 16S rRNA gene sequencing analysis. After gentamicin and imipenem administration and prosthetic valve replacement surgery, bacteremia was resolved, but the patient died. In this case, PVE, which occurred in a patient with no known medical history other than heart disease, was caused by C. fetus. Rapid identification of the pathogen is crucial for the appropriate management of PVE. The optimal antimicrobial to treat C. fetus infections is unclear, but based on previous reports and this case, antimicrobials, such as gentamicin, imipenem, and meropenem, can be considered.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 2211-111-1380). The IRB approved the request to waive the requirement for informed consent and approved publication.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231213264 - Supplemental material for Prosthetic valve endocarditis caused by Campylobacter fetus: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605231213264 for Prosthetic valve endocarditis caused by Campylobacter fetus: a case report and literature review by Ayeong Bak, Taek Soo Kim, Hyunwoong Park and Jae Hyeon Park in Journal of International Medical Research
Footnotes
Author contributions
AB, TSK, HP, and JHP contributed to data interpretation. AB prepared the figure. AB and JHP drafted the manuscript. All authors revised the manuscript and approved the final version.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
All authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.