
Abstract
Background:
Helicobacter pylori infection is very common worldwide, and about 10%–16% of these patients develop peptic ulcer disease. However, there is limited research on the impact of H. pylori eradication and peptic ulcer disease treatment sequencing.
Methods:
We conducted a retrospective study of adult patients diagnosed with H. pylori infection and peptic ulcer disease between October 2020 and April 2021 at our center. Data on primary treatment outcomes, including H. pylori eradication and peptic ulcer disease healing, were collected, and factors that may influence treatment outcomes were analyzed.
Results:
A total of 306 patients were included in this study. The sequence of H. pylori eradication and peptic ulcer disease treatment did not significantly affect the outcomes of H. pylori eradication and peptic ulcer disease healing. In addition, patient age, peptic ulcer disease type, clinic type and treatment regimen (including choice of proton pump inhibitor) had no significant impact on H. pylori eradication. However, patient gender and the choice of antibiotic combination proved to be key factors, as eradication rates were lower in female patients compared to males, and the combination of levofloxacin and clarithromycin was the least effective in eradicating H. pylori. Regarding peptic ulcer disease healing, the peptic ulcer disease type was an important influencing factor, since gastric ulcers being more likely to get cured completely compared to duodenal ulcers.
Conclusions:
The sequence of H. pylori eradication and peptic ulcer disease treatment does not significantly affect the primary outcomes. Patient gender and the choice of antibiotic combination are important factors in H. pylori eradication, whereas peptic ulcer disease type plays a key role in ulcer healing.
Introduction
Helicobacter pylori (Hp) infection is the most prevalent chronic bacterial infection worldwide, affecting about 50% of the population. 1 It is strongly associated with gastritis, peptic ulcer disease (PUD) and in some cases, even gastric cancer. 2 Hp has been classified as a group I human carcinogen for gastric adenocarcinoma and is also a risk factor for gastric mucosa-associated lymphoid tissue lymphomas. 3 Moreover, Hp sometimes shows antibiotics resistance.4,5 Therefore, it is crucial to eradicate Hp to prevent gastroduodenal pathologies.
Hp infection is the main cause of PUD by mechanism of acid hypersecretion and to mucosal barrier damage. Approximately 10%–16% of infected people develop PUD, including duodenal ulcer (DU) and gastric ulcer (GU). The global prevalence of PUD has decreased over time, in parallel with the declining prevalence of Hp infection. 6 Fundamentally, Hp eradication is essential to ulcer recurrence prevention, ulcer-related deaths reduction, and healthcare costs savings. 7
In China, the most widely used first-line therapy for Hp infection is bismuth quadruple therapy, 8 consisting of bismuth subsalicylate, two antibiotics and a proton pump inhibitor (PPI) taken for 14 consecutive days. In addition, patients with concomitant PUD will receive further therapy with a PPI and a mucosa protectant for 6–8 weeks to treat GUs, or 4–6 weeks to treat DUs. 9 It is well established that the differences in eradication efficacy are mainly caused by antibiotic resistance and inadequate acid suppression. 10 Interestingly, one study found an interaction between Hp infection and gastric cancer risk factors such as cigarette smoking, dietary salt, alcohol, and socioeconomic status.11,12 However, there has been limited research on the impact of sequencing Hp eradication therapy and PUD therapy.
In this study, we focused on the effect of the sequence of Hp eradication therapy and PUD therapy on Hp eradication rates and ulcer healing in patients with Hp infection and PUD.
Methods
Study design and population
This retrospective analysis consisted of adult patients diagnosed with Hp infection and PUD at the First Affiliated Hospital, Zhejiang University School of Medicine between October 2020 and April 2021. The study protocol was approved by Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (IRB No. 2023-0430) in accordance with the Declaration of Helsinki. An informed consent waiver was acquired from the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine as the study used anonymized data following previous standardized medical procedures.
Three different methods were used to test for Hp infection. They were urea breath test, Hp infection on endoscopic pathology or fecal antigen test.13,14 Inclusion criteria for the study were as follows: (1) patients received initial Hp eradication therapy (bismuth quadruple therapy) and PUD therapy, and (2) underwent a urea breath test with or without gastroscopy at the end of all treatments.
Exclusion criteria were as follows: (1) patients with severe liver or kidney insufficiency, malignancy, history of upper gastrointestinal surgery, or gastric infections other than Hp; (2) pregnant or breastfeeding; (3) taking other medications that may interfere with the use of anti-Hp drugs; (4) not taking medicines as prescribed; and (5) severe complications occurring during treatment.
The primary treatment outcomes of our study included Hp eradication and PUD healing. At the end of all treatments, Hp eradication was determined by urea breath test, and PUD healing was assessed by gastroscopy and categorized as “completely healed,” “partially healed” or “not healed.” Various potential influencing factors were analyzed. The focal factor was the sequence of treatment, that is, whether to eradicate Hp first before treating PUD or to treat PUD before eradicating Hp in patients with Hp infection and PUD. Other factors were patient gender, age, PUD type, clinic type, and treatment regimen, including the choice of PPI and antibiotic combination.
Statistical analysis
Based on a literature review, Hp eradication rates are expected to be 87% for those treated first for Hp eradication and approximately 77% for those treated first for PUD. 15 With a two-sided α of 0.05 and a power of 90%, a minimum of 305 study subjects is ultimately required. Statistical analyses were performed using SPSS 26.0 software (IBM Inc., Chicago, IL, USA). The data were expressed as mean ± SD or number (percentage) as appropriate. χ2 test or Fisher’s exact test was used for analyzing the significance of factors mentioned above. A p value < 0.05 was considered statistically significant.
Results
Patient characteristics
This study included 306 adult patients diagnosed with Hp infection and PUD at our center from October 2020 to April 2021. Table 1 shows the baseline characteristics of the patients. The majority (75.8%) of the patients were from the general outpatient clinic and 63.4% of the study cohort were male. The average age of the patients was 41.7 years with 18–59 years as the largest age group. DUs were the most common type of ulcer, followed by GUs and compound ulcers. Most patients received treatment to eradicate Hp followed by PUD therapy.
Baseline characteristics of patients with Hp infection and PUD.

DU: duodenal ulcer; GU: gastric ulcer; Hp: Helicobacter pylori; PUD: peptic ulcer disease.
Sequence of treatment does not affect the main treatment outcomes
Our study involved a total of 13 treatment regimens for Hp eradication, including six antibiotic combinations (amoxicillin & clarithromycin, amoxicillin & furazolidone, furazolidone & clarithromycin, metronidazole & clarithromycin, levofloxacin & clarithromycin, and levofloxacin & furazolidone) and four PPIs (omeprazole, pantoprazole, esomeprazole, and rabeprazole).
In terms of primary treatment outcomes (as presented in Table 2), treatments’ administration sequence had no significant effect on Hp eradication (p = 0.749). Moreover, among the 91 patients who underwent post-treatment gastroscopy review, the sequence of treatment did not make a difference on the outcome of PUD healing (p = 0.453). These findings suggested that whether Hp infection or PUD was treated first, the overall treatment effect remained consistent.
Effect of treatment sequence on Hp eradication and PUD healing.
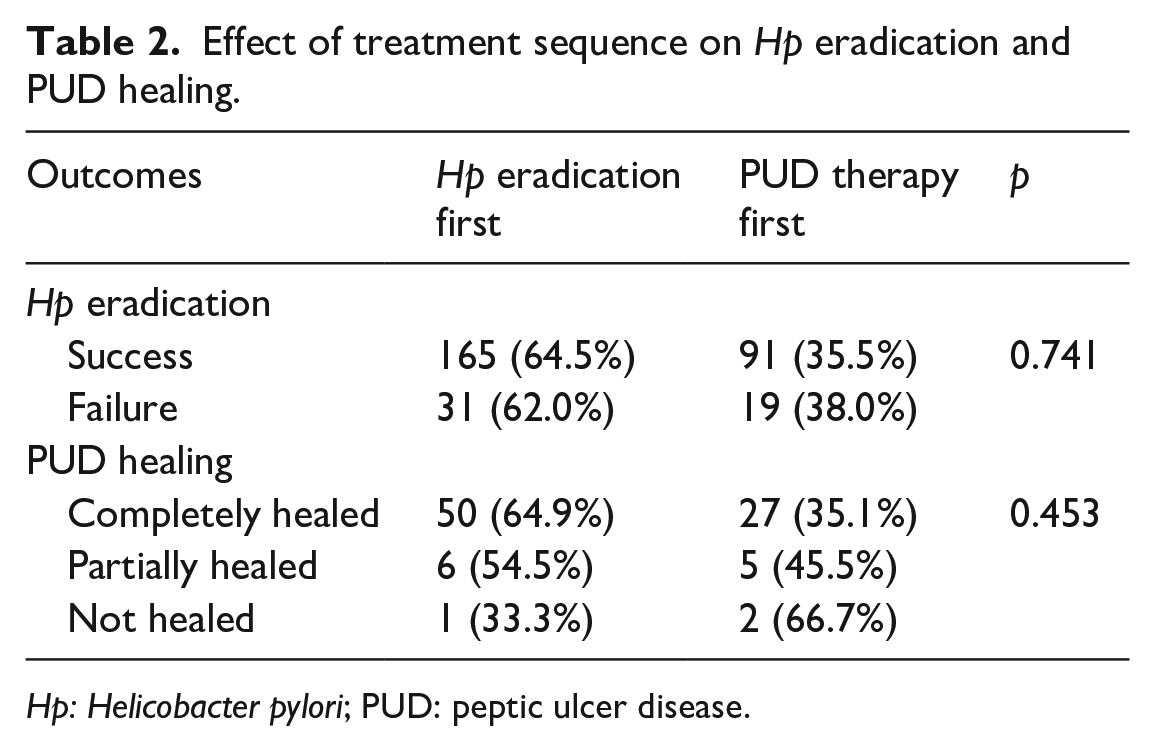
Hp: Helicobacter pylori; PUD: peptic ulcer disease.
Factors affecting Hp eradication
After further analyzing other factors that might affect Hp eradication in patients with Hp infection and PUD (Table 3), our findings indicated that patient age, PUD type, clinic type, and treatment regimen, including PPI choice, did not significantly influence the Hp eradication.
Factors that may affect Hp eradication.
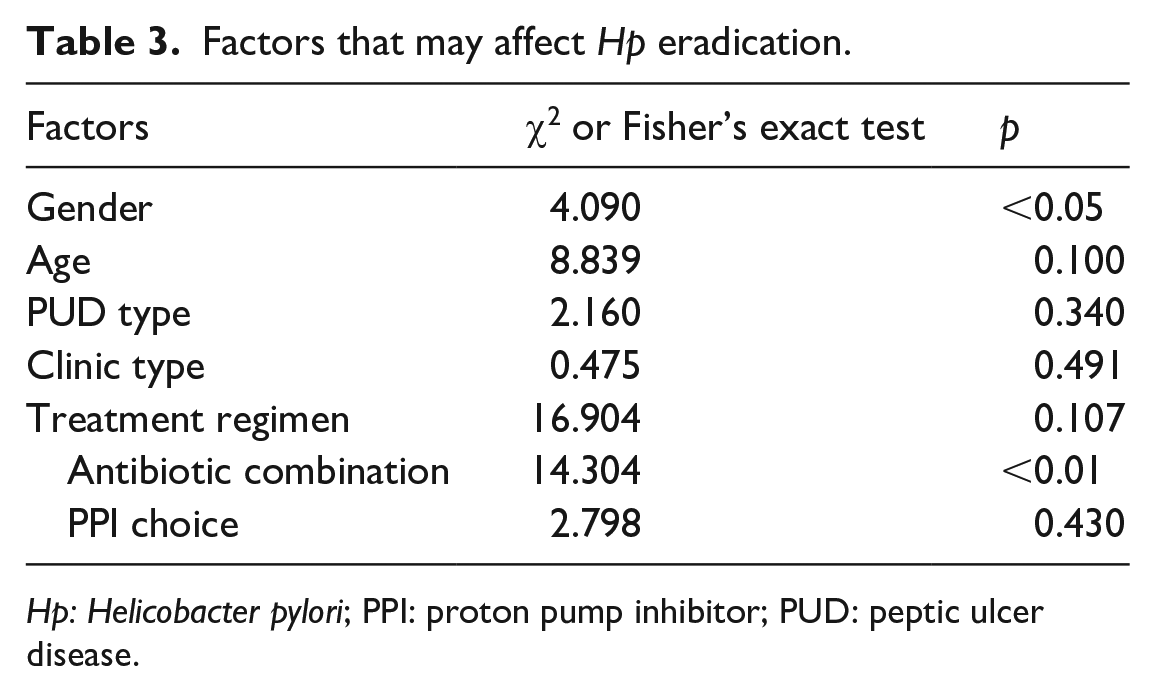
Hp: Helicobacter pylori; PPI: proton pump inhibitor; PUD: peptic ulcer disease.
However, the choice of antibiotic combination proved to be a critical factor, with the levofloxacin & clarithromycin combination showing the lowest efficacy for Hp eradication, as shown in Table 4. Interestingly, patient gender also had a significant impact on Hp eradication, as females exhibited lower eradication rates compared to males. In further multivariate logistic regression analysis, we observed a robust independent effect of patient gender and antibiotic combination on Hp eradication.
Effect of patient gender and antibiotic combination on Hp eradication.

Hp: Helicobacter pylori.
Factors affecting PUD healing
In addition, we conducted an analysis of factors that could potentially affect PUD healing (see Table 5). Patient gender, age, clinic type, and treatment regimen, including the choice of PPI and antibiotic combination, had no significant effect on PUD healing, whereas PUD type showed a notable impact on its healing.
Factors that may affect PUD healing.

PPI: proton pump inhibitor; PUD: peptic ulcer disease.
In detail, as shown in Table 6, GUs are more likely to heal completely compared to DUs. Moreover, compound ulcers should be analyzed separately: among five compound ulcers that failed to heal completely, there was only one GU versus four DUs. Similarly, we validated the effect of PUD type on PUD healing by multivariate logistic regression analysis.
Effect of PUD type on PUD healing.

DU: duodenal ulcer; GU: gastric ulcer; PUD: peptic ulcer disease.
Discussion
In our retrospective study on patients with Hp infection and PUD, we found that the sequence of treatment had no significant effect on main treatment outcomes, including Hp eradication and PUD healing. Furthermore, we analyzed factors that may affect Hp eradication and PUD healing. Patient gender and the choice of antibiotic combination played crucial roles in Hp eradication, while the type of PUD had a significant influence on PUD healing.
Over the past decade, Hp infection has received growing attention worldwide. The global prevalence of Hp infection in adults has declined from 50–55% to 43% due to improvements in socio-economic status, living standards and hygiene.16,17 Recently, the Maastricht VI/Florence Consensus Report has addressed various important aspects of Hp infection, such as treatment based on antibiotic susceptibility, and new insights into the Hp-gut microbiota relationship. 18 However, research and guidelines on the optimal treatment sequence for patients with both Hp infection and PUD is still rare. Our study specifically addressed this issue and showed that the treatment sequence, whether to eradicate Hp or treat PUD first, had no significant impact on the treatment outcome of Hp eradication and PUD healing.
However, we found that the choice of antibiotic combination played a crucial role in Hp eradication. The combination of levofloxacin and clarithromycin showed the lowest efficacy, possibly due to the relatively high level of antibiotic resistance. Other antibiotic combinations (amoxicillin & clarithromycin, amoxicillin & furazolidone, furazolidone & clarithromycin, metronidazole & clarithromycin, and levofloxacin & furazolidone) showed similarly higher Hp eradication rates. Interestingly, patient gender also emerged as an influencing factor for Hp eradication, with female patients having lower eradication rates than males. Several studies have suggested that this gender difference may be attributed to females being preferentially infected with Hp strains with the A2143G mutation and having higher rates of clarithromycin resistance compared to males.19,20 These factors can contribute to eradication failure in female patients.
On the other hand, PUD type was discovered as an important influencing factor in PUD healing. In our study, among the 91 patients who underwent post-treatment gastroscopy review, 21.6% (11/51) of DUs and 4.5% (3/67) of GUs remained unhealed, indicating that DUs were less likely to recover from treatments than GUs. A recent meta-analysis showed that Hp eradication therapy was superior to ulcer treatment drugs in DU healing, while no significant difference was observed in GU healing. 21 These imply that Hp eradication is particularly crucial for the healing of DUs compared to GUs. Therefore, treating Hp infection is an important step in curing DUs.
However, there are still some limitations in our study. This was a retrospective analysis with limited quality of evidence, as our original intention in conducting this study was to explore potential associations. Due to the limited sample size, our study did not cover all treatment options in clinical practice. In addition, the high variability of ulcer healing drugs in our study made it difficult to analyze their effect on treatment outcomes. Future prospective studies with large samples are needed. In recent years, there has been a variety of inspiring studies on Hp and PUD. A randomized controlled trial demonstrated the preventive effect of Hp eradication on aspirin-associated peptic ulcer bleeding. 22 In addition, metagenomic and single-cell RNA-Seq analysis revealed dramatic changes in the composition of gastric microbiome and immune cells in Hp-infected asymptomatic individuals. 23 Eradication of Hp also induced increased long-term resistant bacteria communities in the gut. 24 These imply an interplay between Hp and gastrointestinal microbiota. Moreover, some findings suggest a pathophysiological involvement of non-Hp Helicobacters in gastric diseases. 25 Therefore, more studies are needed to further explore these aspects in the future.
Conclusions
The treatment sequence, whether to eradicate Hp or treat PUD first, had no significant effect on the overall treatment outcome. However, patient gender and the choice of antibiotic combination were important factors influencing Hp eradication. In addition, compared to GUs, DUs have a higher risk of healing failure and Hp eradication is particularly crucial for healing. These findings provide valuable insights into the treatment of patients with Hp infection and PUD.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
Xinjue He was responsible for Investigation and Writing—Original Draft Preparation. Lan Li was responsible for Methodology and Formal Analysis. Chao Lu was responsible for Conceptualization and Writing—Review and Editing. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (No. 81970498, to Lan Li) and Natural Science Foundation of Zhejiang Province (No. LZ22H030002, to Lan Li).
Ethics approval and consent to participate
This retrospective study was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine (No. 2023-0430) in accordance with the ethical guidelines of the 1975 Declaration of Helsinki. The consent waiver was obtained from the Clinical Research Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine because the study used anonymized data obtained in previous standardized medical procedures.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.