
Abstract
Objective
To evaluate the application value of dual-energy computed tomography (DECT) in the differential diagnosis of acute intracranial hemorrhage and calcification.
Methods
This retrospective study involved patients who underwent non-contrast-enhanced cranial DECT in Anhui Wannan Rehabilitation Hospital from January 2015 to November 2022. The processed mixed images obtained after DECT were used as the conventional CT images. Each hyperdense lesion was analyzed based on virtual non-calcium and calcium overlay and classified as calcification or hemorrhage. The sensitivity, specificity, and accuracy of conventional CT and DECT were calculated by the chi-square test according to the unified reference standard.
Results
Sixty-six hyperdense intracranial lesions of 60 patients were analyzed; of these lesions, 41 (62.12%) were calcifications and 25 (37.88%) were hemorrhages. The sensitivity, specificity, and accuracy of DECT in identifying hemorrhage were 96.00%, 100%, and 98.48%, respectively, while those of conventional CT were 72.00%, 97.56%, and 87.88%, respectively. Of the 66 lesions, 4 (6.06%) could not be qualitatively identified and 3 (4.55%) were misdiagnosed by conventional CT but correctly identified by DECT.
Conclusions
DECT can accurately distinguish acute intracranial hemorrhage from calcification, especially in cases that are difficult to diagnose by conventional CT.
Keywords
Introduction
In the identification of acute intracranial hemorrhage and calcification, dual-energy computed tomography (DECT) can accurately distinguish calcifications from hemorrhages, especially in cases that are difficult to diagnose by conventional CT. 1 The principle of DECT is to achieve material separation based on the distinct X-ray attenuations of various materials when exposed to X-rays of different energy levels. The application of DECT in the nervous system has become a research hotspot; such DECT applications include identification of iodine extravasation and subarachnoid hemorrhage after intra-arterial interventions for stroke as well as identification of tumoral or nontumoral hemorrhage. However, few studies have focused on the identification of acute intracranial hemorrhage and calcification. This retrospective analysis involved patients in whom intracranial hemorrhage and calcification were difficult to identify by conventional CT. The purpose of the study was to investigate the application value of DECT in the identification of intracranial hemorrhage and calcification.
Patients and methods
Patient population
The cranial DECT data of patients admitted to the Stroke Center of Anhui Wannan Rehabilitation Hospital from January 2015 to August 2022 were retrospectively analyzed, and their conventional CT images were replaced by reconstructed mixed images (mixing ratio of 0.4). In total, 358 cranial DECT images were obtained during the study period. In 78 (21.79%) images, at least one intracranial hyperdense lesion was found by conventional CT. For 12 of these images, the reference standard could not be confirmed because of lack of comparison images, and these images were therefore excluded. Finally, 66 intracranial hyperdense lesions (and their reference standards) of 60 patients were analyzed. The inclusion criteria were at least one hyperdense lesion on conventional CT, a hyperdense lesion CT value of ≤100 HU, and complete clinical and imaging data. The exclusion criteria were subdural or epidural hematoma, ischemic stroke, and typical findings of cerebral hemorrhage on CT images.
Imaging parameters
The second-generation Siemens dual-source CT system (SOMATOM Definition Flash; Siemens Healthineers, Erlangen, Germany) was used for DECT. Tube A was 80 kV, and tube B was Sn140 kV. The CARE Dose4D CT Automatic Exposure Control System (Siemens Healthineers) was used. The tube rotation time was 0.5 seconds, and the pitch was 0.7. Two sets of images with slice thicknesses of 3.0 mm and 1.0 mm were reconstructed. Each group of images included the 80-kV series, the 140-kV series, and mixed images (mixing ratio of 0.4), and the reconstructed image convolution kernel was Q30f. Data were transferred to a workstation (syngo.via, VB10B; Siemens Healthineers) and analyzed by Brain Hemorrhage software (Siemens Healthineers) using a material separation algorithm based on water, hemorrhage, and calcium (iodine), with the iodine slope of 3.01 modified to the calcium slope of 1.45 and with a threshold of 1500 HU. The calcium overlay ratio was adjusted, and virtual non-calcium (VNCa) images and calcium overlay images were reconstructed. The slice thickness was 3 mm, the spacing was 3 mm, the window width was 80, and the window level was 40.
Image analysis
Two radiologists with more than 10 years of experience analyzed the cranial DECT images, and when disagreement occurred, a consensus was reached through consultation. First, the conventional CT images were analyzed, and each hyperdense intracranial lesion on conventional CT images was classified as calcification, hemorrhage, or unidentified. Multiple lesions of the same property were recorded as one lesion, such as bilateral basal ganglia calcification or multifocal hemorrhage. Multiple hyperdense lesions with different properties in the same patient were recorded as different lesions. Two months later, two radiologists reanalyzed each lesion based on the VNCa and calcium overlay images and classified each lesion as calcification or hemorrhage. Lesions that appeared hyperdense on the VNCa image and unstained on the calcium overlay image were classified as hemorrhage, and lesions that appeared hyperdense on the calcium overlay image but disappeared on the VNCa image were classified as calcification.
A follow-up CT scan or a ≥1-week-earlier CT scan showing stable hyperdense lesions could be used as the basis for diagnosis of calcification. Absence of edema around the lesion on magnetic resonance imaging (MRI) and characteristic changes on susceptibility-weighted images could each be used as a diagnostic criterion for calcification. If CT or MRI showed that the lesions had grown within a short time or the surrounding edema had markedly progressed, hemorrhage was diagnosed. The reporting of this study conforms to the STROBE guidelines. 2
Statistical analysis
IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA) was used for analysis. Measurement data conforming to a normal distribution are expressed as mean ± standard deviation, and count data are expressed as raw number or percentage. The sensitivity, specificity, and accuracy of DECT and conventional CT for the correct classification of hemorrhage were calculated. The chi-square test was used to compare variables between the two groups, and P < 0.05 was considered statistically significant.
Results
The patients’ mean age was 69.2 years (range, 55–83 years). Among the 60 patients, 24 (40%) were women (mean age, 70.0 ± 6.4 years) and 36 (60%) were men (mean age, 68.6 ± 11.5 years).
Twenty-nine lesions were confirmed by comparison with previous CT, 13 lesions were confirmed by follow-up CT, 14 lesions were confirmed by follow-up MRI, 9 lesions were confirmed by comparison with previous MRI, and 1 lesion grew and was diagnosed as hemorrhage. Of the 66 intraparenchymal lesions, calcification was diagnosed in 41 (62%) and hemorrhage was diagnosed in 25 (38%). Of the 25 hemorrhagic foci, 21 (84%) were intraparenchymal hematomas and 4 (16%) were hemorrhagic masses.
The reference standards for the classification and diagnosis of intracranial hemorrhage by conventional CT and DECT are shown in Table 1. The results of DECT and conventional CT for identification of intracranial hyperdense lesions are listed in Table 2. The sensitivity, specificity, and accuracy of the classification of hemorrhage are given in Table 3.
Criteria for classification of intracranial hemorrhage by conventional CT and DECT.

CT, computed tomography; DECT, dual-energy computed tomography; MRI, magnetic resonance imaging.
Diagnostic results of DECT and conventional CT for intracranial hyperdense lesions.

CT, computed tomography; DECT, dual-energy computed tomography.
Sensitivity, specificity, and accuracy of DECT and conventional CT for intracranial hemorrhage.
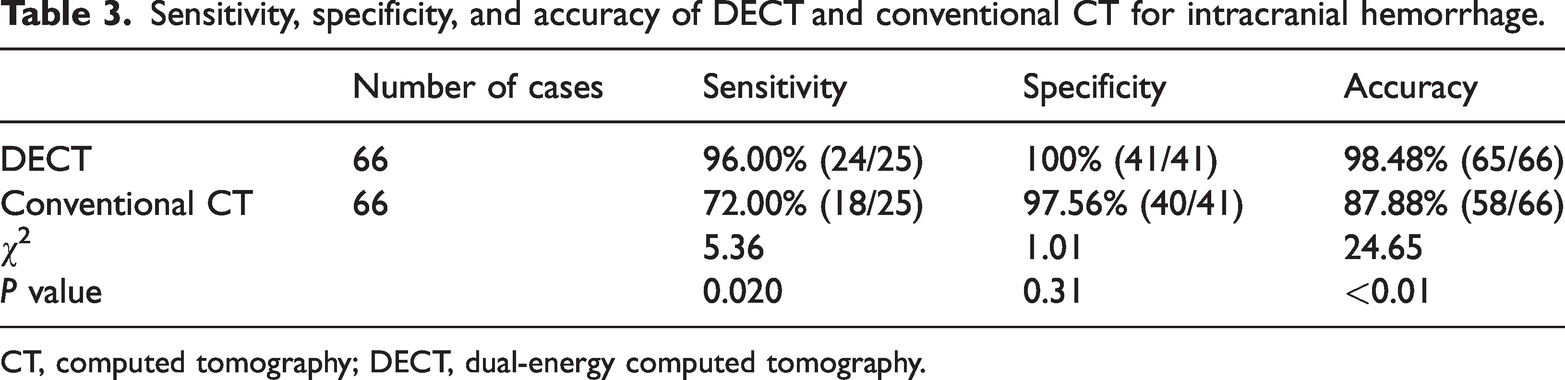
CT, computed tomography; DECT, dual-energy computed tomography.
On conventional CT images, 18 of 25 hemorrhagic lesions were correctly diagnosed as hemorrhage (sensitivity of 72.00%, specificity of 97.56%, and accuracy of 87.88%). On DECT images, however, 24 of the 25 hemorrhagic lesions were correctly diagnosed as hemorrhage (sensitivity of 96.00%, specificity of 100%, and accuracy of 98.48%). The accuracy of DECT was significantly higher than that of conventional CT (P = <0.01). Although DECT also had higher sensitivity (P = 0.020), the difference in specificity between DECT and conventional CT was not statistically significant. Of the eight lesions that were misdiagnosed or unidentified by conventional CT, seven were correctly diagnosed by DECT (Table 4).
DECT results of eight unidentified and misdiagnosed cases by conventional CT.

CT, computed tomography; DECT, dual-energy computed tomography; HU, Hounsfield units; MRI magnetic resonance imaging.
Discussion
Intracranial calcification and hemorrhage are the two most common hyperdense lesions on cranial CT, and their identification is important for diagnosis and treatment. Intracranial calcifications can be seen as sequelae of dystrophic changes in the basal ganglia and choroid plexus. They can also occur as part of the pathological process of other diseases, such as cysticercosis, Sturge–Weber syndrome, tuberous sclerosis, and slow-growing brain tumors including cavernous hemangioma, oligodendroglioma, meningioma, dermoid tumor, and craniopharyngioma. 1 Intracranial hemorrhage occurs more frequently in association with acute head trauma, stroke, and tumors such as metastatic melanoma and glioblastoma. Conventional CT can be used to diagnose most focal hyperdense lesions, such as dystrophic calcification of the basal ganglia and traumatic intracerebral hemorrhage. However, the X-ray attenuation of the lesions differs according to the presence of calcium, resulting in considerable overlap in the CT values of calcifications and hemorrhages and thus making it difficult to distinguish between the two. 3 This is especially problematic in some patients with acute trauma who have hemorrhage on top of calcification, making the differential diagnosis more difficult. The DECT-based material separation technique can facilitate correct diagnosis of such lesions.4–6
This study showed that in common hyperdense lesions, DECT using calcium overlay and VNCa imaging can effectively distinguish calcification from hemorrhage with significantly higher sensitivity and accuracy than conventional CT. This is an advantage of the DECT technique because it minimizes observer subjectivity by exploiting the inherent differences in the spectral signatures of blood and calcium at different energies. In the present study, there was no significant difference in the specificity of DECT and conventional CT for the diagnosis of calcification, indicating that the specificity of the two methods was high.
Of the eight lesions misdiagnosed and unidentified by conventional CT, seven were correctly diagnosed by DECT. Among these, one lesion was diagnosed as right cerebellar hemispheric hemorrhage on conventional CT images but was later diagnosed as calcification by DECT; after 1 week, conventional CT showed no significant changes in the lesion (Figure 1). Additionally, one lesion was diagnosed as right frontal lobe calcification on conventional CT images but was later diagnosed as hemorrhage by DECT. Routine follow-up CT 12 days later showed absorption of the hemorrhage (Figure 2). In another case, a hyperdense lesion in the right occipital region that could not be identified by conventional CT was diagnosed as calcification on DECT; later, however, slight hypointensity, slight hyperintensity, and homogeneous enhancement on T1-weighted imaging all indicated a meningioma (Figure 3). Another patient had a hyperdense lesion in the midbrain that could not be identified by conventional CT and was diagnosed as hemorrhage by DECT (Figure 4). The only false-negative identification by DECT was a mixed appearance of hemorrhage and post-angiographic contrast staining after calcium hydrolysis. In this case, both the iodinated contrast and the blood were subtracted on the VNCa image, showing hyperdensity on the calcium overlay image. This suggests that the presence of hyperdensity and virtual non-contrast enhancement on iodine overlay images are compatible with a mix of hemorrhage and iodine staining.
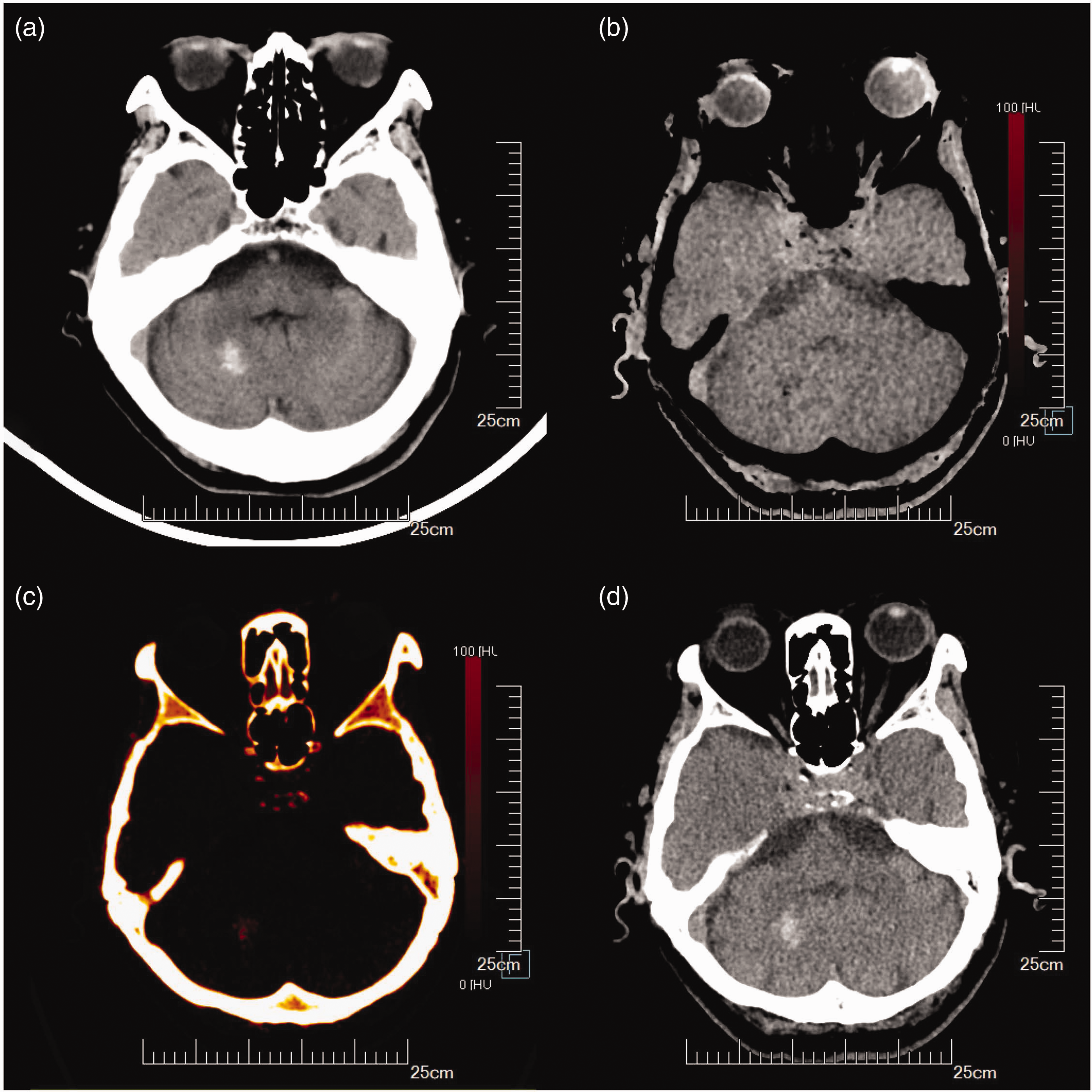
Conventional computed tomography shows hemorrhage, dual-energy computed tomography confirms calcification. (a) Conventional computed tomography shows hyperdense lesions in the right cerebellar hemisphere, suggesting hemorrhage. (b) Virtual non-calcium image shows hypodensity. (c) Positive calcium staining and (d) Computed tomography re-examination 1 week later shows no changes in the lesions.

Conventional computed tomography shows calcification, dual-energy computed tomography confirms hemorrhage. (a) Conventional computed tomography shows hyperdense lesions in the right frontal lobe, suggesting calcification. (b) Virtual non-calcium image shows hyperdensity. (c) Negative calcium staining and (d) Computed tomography re-examination after 12 days shows hemorrhage absorption.

Conventional computed tomography shows an unidentified lesion, dual-energy computed tomography confirms calcification. (a) Conventional computed tomography shows a hyperdense lesion in the right occipital region, which is unidentified. (b) Virtual non-calcium image shows hypodensity. (c) Positive calcium staining. (d) Slight hypointensity on T1-weighted imaging. (e) Slight hyperintensity on T1-weighted imaging and (f) Homogeneous enhancement on T1-weighted imaging.

Conventional computed tomography shows an unidentified lesion, dual-energy computed tomography confirms hemorrhage. (a) Conventional computed tomography shows a hyperdense lesion in the midbrain, which is unidentified. (b) Virtual non-calcium image shows slight hyperdensity. (c) Negative calcium staining. (d) Hyperintensity on T1-weighted imaging. (e) Mixed hyperintensity and hypointensity on T2-weighted imaging and (f) Slight hypointensity on fluid-attenuated inversion recovery.
The incidence of acute cerebral hemorrhage is relatively high, and the DECT-based material separation technique has become a simple and useful tool to distinguish hemorrhage from calcification in the clinical setting. 7 However, a diagnostic method based only on calcium overlay and VNCa images can only determine whether hyperdense lesions contain calcium. Noncalcified hyperdense lesions include soft tissue lesions other than hemorrhages, such as hyperdense tumors or metastases, which require reference to traditional imaging features and the patient’s clinical history. 8 A mix of iodinated contrast and hemorrhage may appear as a hyperdensity on the calcium overlay image and be subtracted after VNCa imaging, leading to misdiagnosis if mixing of iodinated contrast and hemorrhage occurs. 9 Generally, however, this situation does not cause diagnostic difficulties because clinicians usually know in advance that a contrast agent was used, which can be confirmed by virtual non-contrast-enhanced images and iodine overlay, calculated by changing the iodine slope.10,11
The limitations of this study are the small number of samples and retrospective design. Conventional CT can distinguish hemorrhage from calcification in most cases. In cases where conventional CT is ineffective, however, DECT can reliably diagnose the etiology of hyperdense lesions.
Conclusions
Mixed CT images generated by postprocessing of the data collected by DECT can be a good substitute for conventional CT images. When the calcium overlay and VNCa images are combined, hemorrhage and calcification can be better identified.
Footnotes
Acknowledgement
The authors would like to thank all individuals who participated in this study.
Author contributions
Fang Song and Faping Zhang designed the study. Fang Song collected the data. Fang Song and Faping Zhang analyzed the data and wrote and revised the manuscript.
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Ethics
We have de-identified all patient details in the study. Because this study was retrospective and patient data were de-identified, the requirements for institutional review board approval and patient informed consent were waived.
Funding
This work was supported by the Wuhu Science and Technology Program Project (2021cg39): Application of the dual-energy computed tomography (DECT)-based material separation technique in differential diagnosis and prognostic evaluation of cerebral hemorrhage.