
Abstract
Objectives:
Early surgical intervention within 48 h is critical for reducing mortality and morbidity in patients with hip fractures. However, occult hip fractures are often missed, leading to treatment delays. Dual-energy computed tomography allows visualization of bone marrow edema and bone contusions, which are challenging to detect using conventional computed tomography. This study aimed to evaluate the effectiveness of dual-energy computed tomography in diagnosing occult hip fractures.
Methods:
Eighteen dual-energy computed tomography scans obtained between May 2018 and March 2024 were analyzed. Magnetic resonance imaging was performed in all cases. A trained musculoskeletal radiologist interpreted the dual-energy computed tomography and magnetic resonance imaging scans, which were then reviewed by two senior orthopedic surgeons. The confirmed diagnoses included 14 femoral trochanteric fractures and 4 femoral neck fractures. Four junior orthopedic surgeons independently reviewed the dual-energy computed tomography scans only and conducted diagnostic examinations. Patients were subsequently categorized into two groups: those with unanimous diagnostic agreement (unanimity group) and those with discrepancies (objection group).
Results:
For femoral trochanteric fractures, sensitivity, specificity, accuracy, and Cohen’s kappa coefficient were 94%, 81%, 0.91, and 0.75, respectively. For femoral neck fractures, sensitivity, specificity, accuracy, and Cohen’s kappa coefficient were 68%, 96%, 0.90, and 0.69, respectively. A significant difference in diagnostic ease was noted (p = 0.04), with agreement achieved for 12 of the 14 femoral trochanteric fractures and one of the four femoral neck fractures. Logistic regression analysis yielded a regression coefficient for femoral trochanteric fractures of 3.05 (p = 0.03), indicating that these fractures were more easily diagnosed than femoral neck fractures.
Conclusions:
Dual-energy computed tomography demonstrated high sensitivity and specificity in detecting occult hip fractures, particularly those of the femoral trochanter. However, its sensitivity was lower for femoral neck fractures, indicating limited reliability in their diagnosis. Further investigation and magnetic resonance imaging scans are recommended for suspected femoral neck fractures.
Keywords
Introduction
Previous research indicates that to lower the rates of both mortality and morbidity, patients who fracture their hips should undergo surgical treatment within 48 h.1 –3 Delayed diagnosis of hip fractures is linked to an increased risk of complications, including displacement, the need for more extensive surgery, nonunion, avascular necrosis, thromboembolic events, and a higher mortality rate. 4 Therefore, early diagnosis is essential for optimizing treatment and improving outcomes because most hip fractures require surgical intervention. Although most hip fractures can be identified and managed based on radiographic imaging, occult hip fractures may be present in 3%–10% of cases where the findings on initial radiographs appear negative.5,6 If clinical concerns persist despite initial radiographs appearing negative for fractures, additional imaging should be conducted.
Magnetic resonance imaging (MRI) is the standard imaging technique used to detect occult hip fractures because of its sensitivity in identifying associated bone marrow edema (BME).7,8 However, patient comfort during an MRI examination can be an issue, with up to 2% of examinations being terminated early due to claustrophobia. 9 Some facilities face challenges because they are unable to perform MRI examinations promptly, and MRI examinations themselves are also limited in that patients with implanted pacemakers or those who cannot remain still due to dementia or restlessness cannot undergo the procedure.
BME associated with fractures and bone contusions was previously challenging to diagnose using conventional computed tomography (CT) alone. Recently, dual-energy computed tomography (DECT) has emerged as a viable alternative imaging modality that enables such lesions to be visualized.10 –12 Reports suggest that information from DECT images can be analyzed using three-material decomposition to differentiate calcium signals and detect BME.10,13 Moreover, DECT can differentiate materials based on their distinct X-ray absorption characteristics, which vary according to atomic number. By acquiring data using two different X-ray energy spectra, DECT highlights the energy-dependent absorption behaviors of various materials. 14
Our hospital, an acute care facility specializing in orthopedic, neurological, and acute coronary artery conditions, implemented a Revolution CT from GE HealthCare Japan in October 2017. We have been utilizing the dual energy GSI Xtream (GE HealthCare Japan Corporation, Tokyo, Japan) for imaging BME related to fractures and bone contusions. This system uses fast kVp switching between 80 and 140 kVp, enabling 2 high-density datasets to be collected without misalignment or time shifts. 15
Furthermore, we implement DECT imaging to detect BME in cases of suspected occult hip fractures and to determine whether additional MRI is necessary. If DECT suggests a fracture, we always perform an MRI, except in patients for whom MRI is not available. If DECT alone is sufficient for diagnosis, it would be beneficial, as it would eliminate the need for MRI. However, the diagnostic accuracy and clinical utility of DECT, particularly in comparison to MRI, are not yet fully established. Therefore, this study aimed to evaluate the effectiveness of DECT in diagnosing occult hip fractures.
Methods
Participants
This retrospective observational study included 22 patients who underwent DECT imaging for suspected occult hip fractures between May 2018 and March 2024. Three patients were excluded due to the absence of MRI scans, as their fractures were visible on conventional CT and were not classified as occult hip fractures. Additionally, one patient with a superior pubic ramus fracture, rather than a hip fracture, was excluded. Ultimately, 18 cases were included in the study.
No patients with pathological fractures were included in this series. MRI and CT showed no bone destruction (destruction of cortex or something like that) or mass; thus, the fracture was judged to be normal, not pathological.
Study procedure
A trained musculoskeletal radiologist interpreted the DECT and MRI scans, which were then reviewed by two senior orthopedic surgeons. The confirmed diagnoses included 14 femoral trochanteric fractures and 4 femoral neck fractures. Moreover, four junior orthopedic surgeons independently reviewed the DECT scans only and conducted diagnostic examinations. Patients were subsequently categorized into two groups: those with unanimous diagnostic agreement (unanimity group) and those with discrepancies (objection group).
Two senior orthopedic surgeons reviewed the radiology report and evaluated MRI and DECT images to confirm the diagnosis. A fracture was diagnosed when the MRI findings exhibited low signal intensity on T1-weighted images and high signal intensity in the bone marrow on T2-weighted and STIR images compared to the uninjured side. Furthermore, a femoral neck fracture was identified when the fracture line was confined to the neck, whereas a femoral trochanteric fracture was diagnosed when the fracture line extended between the trochanters. The diagnosis was further confirmed by assessing the presence of BME on DECT and its correspondence with areas of signal change on MRI. The confirmed diagnosis was established through consultation between two senior orthopedic surgeons.
Image assessment
Bone mineral density was evaluated using dual-energy X-ray absorptiometry. Bone mineral density measurements were juxtaposed with the diagnostic standards for primary osteoporosis outlined by the Japanese Society for Bone and Mineral Research in 2012. 16 Specifically, bone mineral density values were compared to the Japanese Young Adult Mean proximal femur bone mineral density and expressed as a percentage of this mean (%Young Adult Mean).
Statistical analysis
Between-group comparisons of demographic characteristics were conducted using Student’s t-test and Fisher’s exact test. Continuous and categorical variables are reported as means ± SDs and proportions, respectively.
Logistic regression analyses identified factors associated with the unanimity group. The unanimity group was the response variable, with body mass index (BMI), dose length product (DLP), and supervisor diagnosis (Femoral trochanteric fracture) as explanatory variables.
All comparisons were performed using two-tailed tests, with statistical significance set at p < 0.05. Odds ratios (ORs), 95% confidence intervals, and p-values were calculated using standard formulas.
Statistical analyses were performed with EZR version 1.68 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), 17 a graphical user interface for R version 4.3.1 (The R Foundation for Statistical Computing, Vienna, Austria), which is a modified version of R Commander designed to include statistical functions frequently used in biostatistics.
Sample size
The sample size was determined through a priori analysis using G*Power version 3.1.9.6 (Franz Faul, Kiel University, Germany). The analysis used the Student’s t-test, with goodness-of-fit parameters set at α = 0.05, 1 − β = 0.8, and an effect size of 0.8. 18 Based on this, the minimum sample size required for the study was 26 patients per group, totaling 52 patients.
Results
During the study period, 22 patients underwent DECT imaging for suspected occult hip fractures. Four patients were excluded, resulting in a final study cohort of 18 patients. The confirmed diagnoses included 14 femoral trochanteric fractures and 4 femoral neck fractures. Four junior orthopedic surgeons independently reviewed the DECT scans only and performed diagnostic examinations. Among them, 13 patients were classified in the unanimity group, where all 4 surgeons made correct diagnoses, while 5 patients were categorized in the objection group due to nonunanimous diagnoses. The study selection flowchart is presented in Figure 1, and representative images are shown in Figure 2.

Flow diagram of participant enrollment.
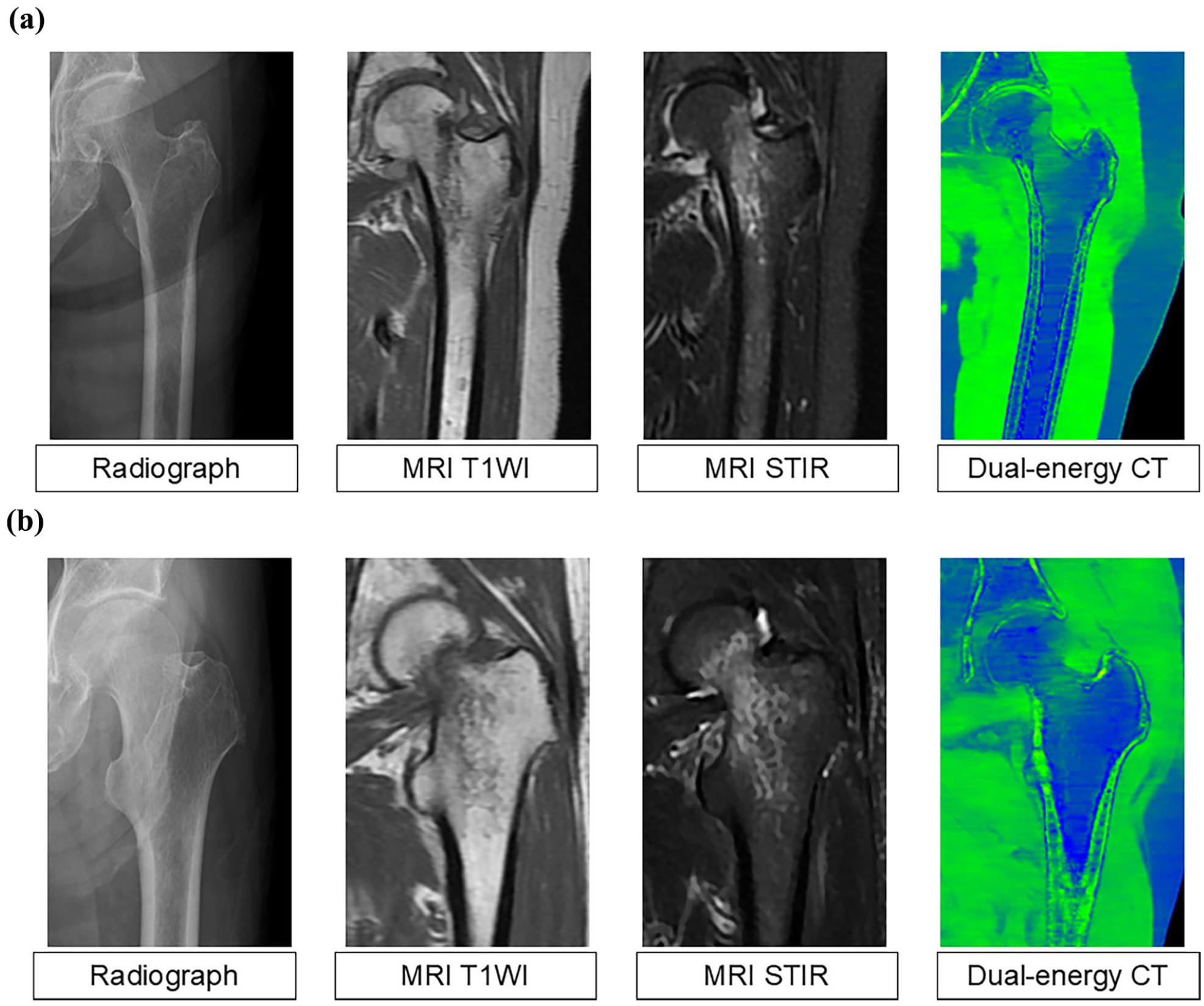
Representative images of a femoral trochanteric fracture (a) and a femoral neck fracture (b). In the dual-energy computed tomography images, bone marrow edema is highlighted in green across the intertrochanteric line.
Table 1 presents the diagnostic performance of DECT. For femoral trochanteric fractures, sensitivity, specificity, accuracy, and Cohen’s Kappa coefficient were 94%, 81%, 0.91, and 0.75, respectively. For femoral neck fractures, sensitivity, specificity, accuracy, and Cohen’s Kappa coefficient were 68%, 96%, 0.90, and 0.69, respectively. DECT demonstrated high sensitivity and specificity for both fracture types, highlighting its strong diagnostic capability. However, sensitivity was slightly lower for femoral neck fractures. The high accuracy values further affirm the reliability of DECT-based diagnoses. Moreover, Cohen’s kappa coefficients exceeding 0.6 indicate substantial interobserver agreement. The negative likelihood ratio for femoral trochanteric fractures was 0.06, emphasizing DECT's value in ruling out this fracture type. Conversely, the positive likelihood ratio for femoral neck fractures was 19.25, confirming DECT as a reliable diagnostic tool.
The diagnostic performance of DECT.

CI: confidence interval; Cohen’s kappa: Cohen’s kappa coefficient; DECT: dual-energy computed tomography; −LR: negative likelihood ratio; NPV: negative predictive value; +LR: positive likelihood ratio; PPV: positive predictive value.
Table 2 shows a comparison of the demographic and clinical characteristics of patients in the unanimity and objection groups. In the diagnostic examinations, a significant difference in diagnostic ease was noted (p = 0.04), with agreement achieved for 12 of the 14 femoral trochanteric fractures and one of the four femoral neck fractures. The groups exhibited no significant differences in patient demographics or DECT settings.
Demographic and clinical characteristics of patients in the unanimity and objection groups.

BMI: body mass index; DLP: dose length product; SD: standard deviation; YAM: young adult mean.
Statistically significant (p < 0.05).
Table 3 presents the results of a logistic regression analysis of factors associated with the unanimity group. The regression coefficient for femoral trochanteric fractures was 3.05 (p = 0.03), indicating that these fractures were more easily diagnosed than femoral neck fractures. Neither BMI nor DLP were identified as confounding factors associated with unanimity groups.
Logistic regression analysis of factors associated with unanimity group.

AIC: Akaike’s information criterion; BMI: body mass index; DLP: dose length product; SE: standard error.
Statistically significant (p < 0.05).
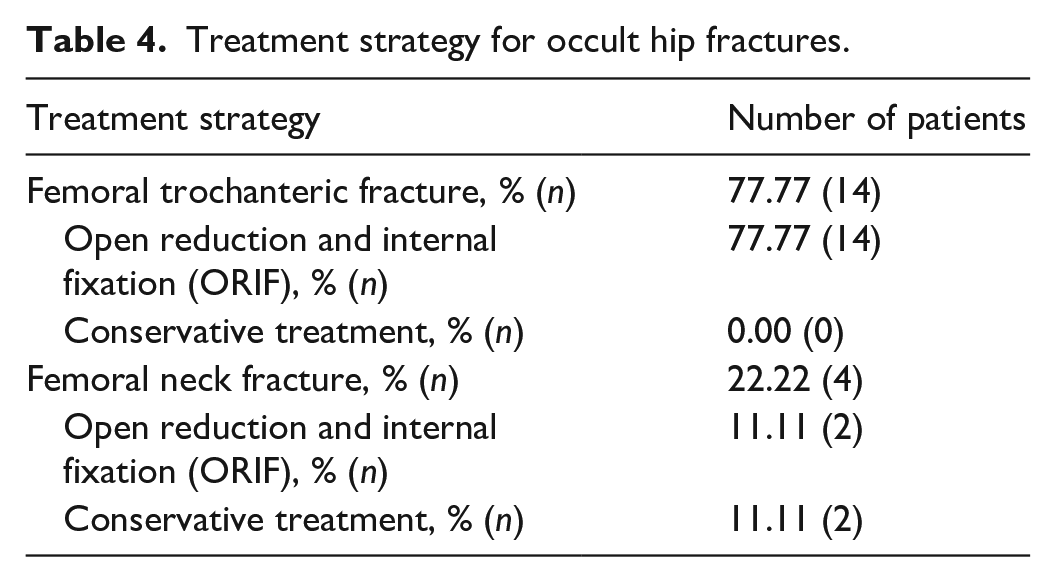
Table 4 outlines the treatment strategies for occult hip fractures. In this study, all femoral trochanteric fractures were treated with open reduction and internal fixation (ORIF). Conversely, two femoral neck fractures were treated with ORIF, while the other two received conservative treatment. The surgical group for neck fractures had an average hospital stay of 39 days, whereas the conservative treatment group had an average stay of 34 days. At the time of the final follow-up, all patients had achieved successful bone fusion with no dislocation at the fracture site.
Treatment strategy for occult hip fractures.
Discussion
This study assessed the effectiveness of DECT in diagnosing occult hip fractures. DECT demonstrated high sensitivity and specificity, performing well in detecting both femoral trochanteric and femoral neck fractures. It was particularly effective in confirming and excluding femoral trochanteric fractures.
The sensitivity of DECT for detecting BME in the extremities is 86%, with a specificity of 93%, primarily reported for the lower extremities. 19 A meta-analysis found DECT sensitivity and specificity to be 89% and 96%, respectively, for detecting BME in spinal compression fractures. 20 Consistent with these findings, the present study also demonstrated high sensitivity and specificity for DECT.
Conventional CT struggles to detect BME due to the dense trabecular bone structure, which can obscure qualitative assessments.21,22 The accuracy of conventional CT in evaluating hip fractures ranges from 83% to 100%.23,24 Law et al. 25 reported that patients with negative conventional CT results for suspected occult hip fractures did not require hospitalization for fractures within a year, suggesting that modern CT techniques are comparable to MRI in detecting occult hip fractures. While nondisplaced fractures may be missed with conventional CT, DECT enhances diagnostic reliability.
This study is the first to compare DECT’s diagnostic performance for femoral trochanteric versus femoral neck fractures. DECT proved valuable in confirming or excluding occult hip fractures, particularly those of the femoral trochanter. While DECT exhibited high overall sensitivity and specificity for femoral trochanteric fractures, its sensitivity for femoral neck fractures was lower at 68%. Notably, among femoral neck fractures, unanimous diagnostic agreement was low, with consensus achieved in only one of four cases. The lower sensitivity and consensus for femoral neck fractures raise concerns about potential delayed diagnoses. DECT effectively visualizes BME and depicts subtle cortical and trabecular disruptions. Moreover, in femoral neck fractures, BME is confined to a narrow area, whereas in femoral trochanteric fractures, it extends beyond the intertrochanteric line. This broader distribution may contribute to DECT’s higher detection rate for femoral trochanteric fractures.
MRI remains the gold standard for detecting occult hip fractures due to its superior sensitivity and specificity in visualizing BME, particularly in complex cases such as femoral neck fractures. However, MRI scans may be incomplete or canceled due to claustrophobia, patient intolerance, or contraindications such as pacemakers or implants. Additionally, MRI availability in emergency settings is limited, leading to delays. Moreover, MRI scanning is constrained by time and the availability of skilled technicians, making it challenging to schedule during off-hours when many emergency patients present with hip fractures. Conversely, DECT offers advantages in accessibility, speed, and cost-effectiveness, making it a valuable first-line screening tool where MRI is unavailable. However, its practical benefits must be weighed against its lower sensitivity for femoral neck fractures. DECT is a useful alternative for patients unable to undergo MRI, but clinicians should be aware of the potential for false negatives, particularly in femoral neck fractures. Given DECT’s limitations, a high index of clinical suspicion should prompt follow-up MRI regardless of initial DECT findings.
The Japanese Orthopedic Association guidelines state that when an occult hip fracture is suspected, virtual noncalcium DECT has greater diagnostic sensitivity than multiplanar reconstruction alone. 26 Japan’s aging population has led to a rise in orthopedic diseases and fractures, highlighting the need for early diagnosis and treatment to maintain patients’ daily activities and reduce dependency on nursing care. In orthopedic CT imaging, evaluating fractures from multiple angles is essential to assess microfractures, fracture extent, and instability, aiding treatment planning and surgical decision-making.
In most cases, standard radiography is sufficient for diagnosing hip fractures and guiding treatment. However, in patients with strong clinical suspicion of fracture but normal radiographs, additional imaging is required to rule out occult fractures. Conventional CT is preferred in most emergency departments due to its widespread availability. 27 When CT is necessary, DECT is recommended for improved diagnostic accuracy.
Finally, treatment strategies for occult hip fractures should be considered. The Japanese Orthopedic Association guidelines emphasize that early diagnosis is crucial, as delayed detection increases the risk of fracture displacement. 26 A meta-analysis of conservative treatment for nondisplaced femoral neck fractures reported a 19.6% incidence of displacement or pseudoarticulation. 28 For occult femoral neck fractures, ORIF is preferred to prevent displacement, facilitate early mobilization, and enable weight-bearing. Because early diagnosis using DECT was achieved in this study, conservative treatment may be a viable option. However, the management of occult femoral trochanteric fractures remains less clear and requires further research. Recent retrospective studies suggest that greater trochanter fractures with less than 50% extension into the intertrochanteric region heal with bone union without displacement under conservative treatment.29 –32 Katsuyama et al. 33 reported that combined greater trochanter and occult femoral trochanteric fractures could be managed conservatively without progressing to complete fractures, regardless of intertrochanteric extension. Treatment should be individualized, considering patient age, daily activity levels, comorbidities, and surgeon preference. Since diagnosing occult femoral trochanteric fractures is a particular strength of DECT, it plays a key role in guiding treatment decisions.
Limitations
A notable limitation of this study is the insufficient sample size. The limited number of occult hip fracture cases at a single institution made it challenging to achieve an adequate sample size. Additionally, the images used for diagnosis should ideally have included DECT images without fractures, which were not included in this study. As additional DECT images of cases without fracture become available, the sensitivity and specificity of the findings may diminish.
Conclusions
DECT demonstrated high sensitivity and specificity in detecting occult hip fractures, particularly those of the femoral trochanter. However, its sensitivity was lower for femoral neck fractures, indicating limited reliability in their diagnosis. Further investigation and MRI scans are recommended for suspected femoral neck fractures.
Footnotes
Ethical considerations
The study was conducted following the Declaration of Helsinki and was approved by the Research Ethics Committee of Sendai Medical Association Hospital (approval number 6-010) on September 6, 2024.
Consent to participate
This study is a retrospective cohort study, and written informed consent was exempted by the Institutional Review Board. Oral informed consent was obtained from patients who agreed to collect their data for publication.
Author contributions
Hirotaka Kawakami: conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, writing – original draft. Hiromi Sasaki: project administration, supervision, writing – original draft, writing – review & editing. Junichi Kamizono: conceptualization, methodology, writing – original draft. Yuki Yasutake: data curation, investigation. Kana Yamada: data curation, investigation. Suguru Saho: data curation, investigation. Takehiro Kawauchi: data curation, investigation. Noboru Taniguchi: project administration, supervision, writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.