
Abstract
Objective
This study was performed to assess low-dose scan parameters in dual-energy computed tomography (CT) for displaying the anterior cruciate ligament.
Methods
Dual-energy CT scans with low and standard dose parameters, respectively, were performed in nine human knee joint specimens. Eighteen imaging data sets for cruciate ligament specimens were obtained and processed. Statistical analysis was performed for signal-to-noise ratios of the CT images and subjective scores.
Results
Comparable signal-to-noise ratios and subjective image quality scores by evaluators in dual-energy CT anterior cruciate ligament images between the low and standard-dose groups were observed.
Conclusion
Low-dose scan parameters do not compromise the outcomes of anterior cruciate ligament imaging.
Keywords
Introduction
Anterior cruciate ligament (ACL) injury is a common and frequently occurring condition in clinical practice, and it severely impacts patients’ daily lives. The physical examination findings often depend on the patient’s severity of pain, which affects the accuracy of the diagnosis. Magnetic resonance imaging (MRI) has good tissue contrast but poor accuracy in diagnosing partial damage despite the ability to provide reasonably good contrast. Several studies have shown that MRI has low accuracy for identifying partial ACL tears.1–3 It also has many contraindications. Patients with cardiac pacemakers or claustrophobia cannot undergo MRI. Dual-energy computed tomography (DECT) complements traditional computed tomography (CT) in improving soft tissue resolution, increasing the potential for diagnosis of ACL injury. Our previous study showed that the color mapping degrees of the ACLs in the bilateral joints of the same patient were similar (Figure 1) and that the color mapping degree of the torn ACL was lower than that of the corresponding contralateral ACL (Figure 2). This finding was termed “diminution sign-on dual-energy color mapping.”
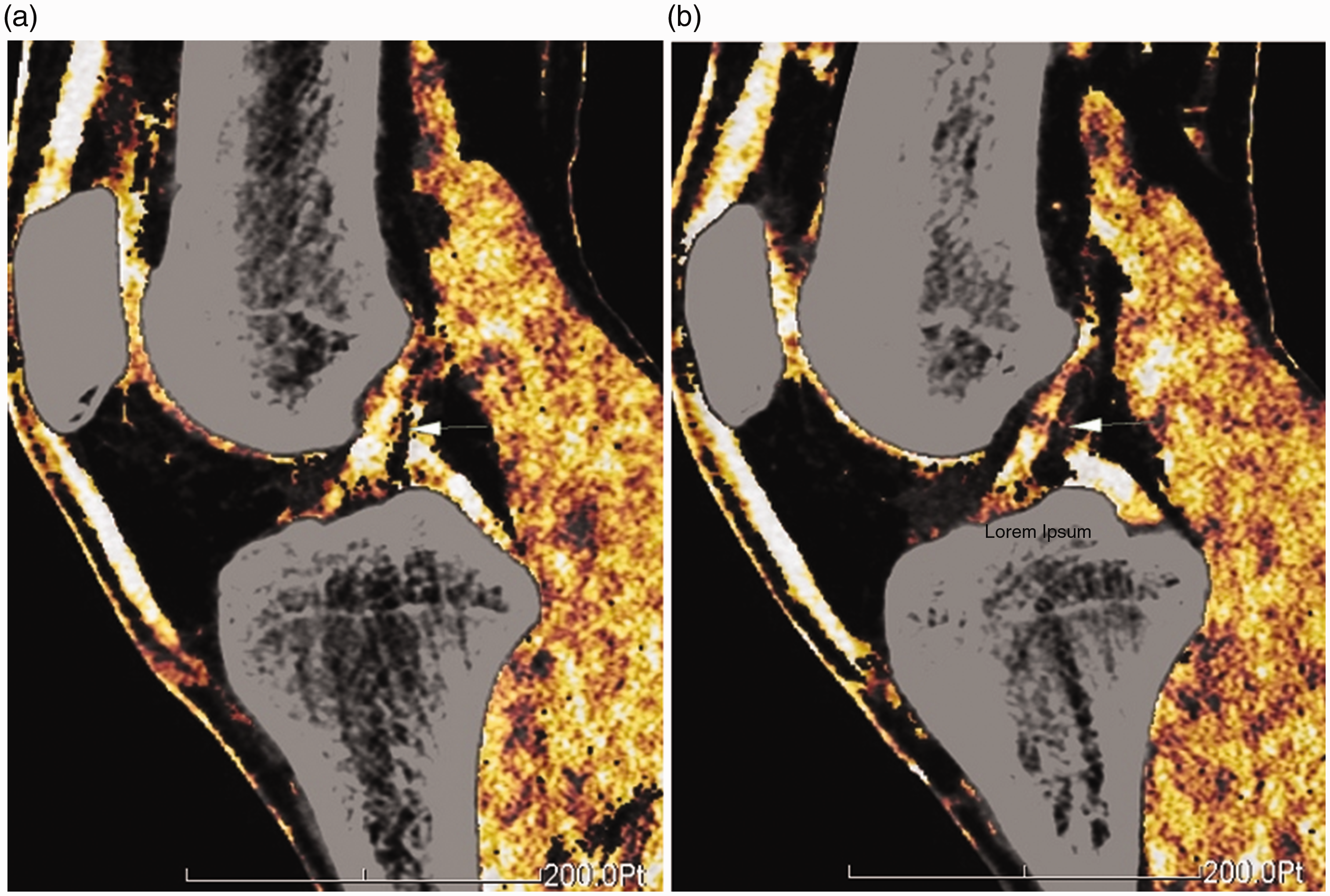
Normal anterior cruciate ligament (ACL) on dual-energy color mapping in a 33-year-old man. (a) Left ACL. (b) Right ACL.

The color mapping degree of the torn left anterior cruciate ligament (ACL) (confirmed by arthroscopy) was lower than that of the right ACL in a 24-year-old man. (a) Left ACL. (b) Right ACL.
DECT shows promise for the diagnosis of ACL injury. Fickert et al. 4 and Peltola and Koskinen 5 also reported the use of DECT for the diagnosis of cruciate ligament injury in piglet models and patients. Although encouraging results are constantly emerging, CT radiation-induced damage remains a real problem that cannot be overlooked. Minimizing the radiation dose in patients to reduce the negative impact of X-ray exposure while maintaining the imaging quality necessary to meet the requirements for diagnosis and treatment is a challenging problem. In the present study, we evaluated a technique with which to achieve both good imaging outcomes and minimal X-ray damage.
Materials and methods
Ethics
Human research ethics approval was obtained from the Ethics Committee of Zhujiang Hospital, Southern Medical University. Informed consent was obtained from all individual participants enrolled in the study.
Experimental materials
Nine human knee joint specimens prefixed with formalin (provided by the Anatomy Department) were included in the study.
Scanning method
A Siemens dual-source CT scanner (Siemens Somatom Definition 2012B; Siemens Healthineers, Erlangen, Germany) in dual-energy mode was used. In the standard-dose group (manufacturer-recommended scheme), the tube current intensities of bulbs A and B were 55 and 234 mAs, respectively. The tube voltages were set at 140 and 80 kV, respectively. The collimation was 20 × 0.6 mm at a pitch of 0.7. The reconstruction slice thickness was 1 mm, the reconstruction increment was 0.7 mm, and the field of view was 250 mm. The kernel was D30s medium smooth convolution with filtered back projection, and the window was Extremity. A fixed scan length was selected to facilitate data analysis. The upper boundary of the scan range included the upper end of the femoral condyle. The lower boundary encompassed the tibial condyle and the lower end of the fibular head. In the low-dose group, the tube current intensities of bulbs A and B were 29 and 123 mAs, respectively (the intensity of bulb B was a device-specific value that could not be manually adjusted); the remaining parameters were the same as in the standard-dose group (Figure 3).

Specimen scanning conditions.
Image post-processing
On a workstation (syngo Multimodality Workplace, VA40; Siemens Healthineers), dual-energy color mapping was performed using the dedicated dual-energy tendon application. The information was color-coded with a specific color lookup table (“tendon,” which codes tendons and ligaments in shades of yellow to orange). Images in the horizontal, oblique coronal, and oblique sagittal planes were reconstructed to assess the ACL morphology and path under color mapping (Figure 4).

Reconstruction of anterior cruciate ligament in the (left) low-dose group and (right) standard dose group in the same subject.
Image evaluation
Objective measurement
CT values and noise (i.e., the standard deviation of the CT values) for the three regions of interest in the proximal, middle, and distal ACLs were measured. The slice that most effectively displayed one of these three regions of the ACL was chosen. The regions of interest were about 3 mm2 (Figure 5). The signal-to-noise ratio (SNR) was calculated as the CT value divided by the CT noise. All measurements were repeated three times, and the average results were used for the analysis.

Schematic diagram of objective anterior cruciate ligament measurement.
Subjective evaluation
Two radiologists with >10 years of clinical experience evaluated the 18 image sets (scan parameters hidden) of 9 specimens using a 5-point Likert scale. Image quality was scored as follows:
Radiation dose representation
The volume CT dose index (CTDIvol) and dose–length product (DLP) were recorded for each scan. The effective dose (ED) of each scan was calculated as k × DLP, where k is the weight factor obtained using the average value (0.0004 ·mGy−1 · cm−1) of the proximal lower limb proposed by the American Association of Physicists in Medicine. 6
Statistical analysis
SNRs and image quality scores are expressed as mean and margin of error of difference between the low- and standard-dose groups. All statistical analyses were performed with SAS 9.4 statistical software (SAS Institute, Cary, NC, USA), with a two-tailed P value of <0.05 considered statistically significant.
Results
SNR comparison
Eighteen sets of dual-energy reconstruction data (nine sets each in the low- and standard-dose groups) were obtained for the nine human knee joint specimens. Image quality was directly reflected by the SNR. The nine samples contained 27 pairs of images, which included the distal end, the middle part, and the proximal end of the ACL for each sample. For each pair of low- and standard-dose images, the average ratio between the SNRs was 1.18 with a 95% confidence interval (CI) of 1.01 to 1.35. The standard dose provided a slightly better SNR. However, the difference was very small and did not affect the image reading by the experts.
Subjective scores
Although quantifying the image quality by measuring the image noise level is a more objective technique, the most important clinical outcome is the subjective information provided by imaging; in other words, the experts’ conclusion obtained by reading the CT images. The 5-point Likert scale of imaging quality between standard- and low-dose X-rays is the most effective tool for subjective evaluation. We invited two radiologists to provide subjective scores for the nine samples in a double-blind manner. Of the 18 pairs, 11 pairs agreed exactly; the remaining 7 pairs showed a difference of only 1 point. The average difference between the two methods was 0.38 (95% CI, 0.15–0.61). When the interobserver agreement for only the standard-dose group of the nine samples was considered, six pairs agreed exactly, two pairs showed a difference of 1 point, and one pair showed a difference of 2 points. This resulted in a difference of 0.44 (95% CI, 0.00–0.91). We also tested the intraobserver agreement with one radiologist. Six pairs agreed exactly and three pairs showed a difference of 1 point. Again, the average difference was 0.33 (95% CI, 0.00–0.66). These results demonstrate that the difference between low and standard doses is comparable with the differences in interobserver and intraobserver agreement.
Radiation doses
The CTDIvol in the standard-dose group was 10.18 mGy, for a DLP of 174.0 mGy; the ED was 0.0696 mSv. The CTDIvol in the low-dose group was 5.88 mGy, for a DLP of 100.5 mGy; the ED was 0.0402 mSv. The equivalent dose in the low-dose group was 42.2% lower than that in the standard-dose group.
Discussion
With the continuous advancements in science and technology during the last decade, the top medical equipment manufacturers have gradually realized the clinical application of the DECT technique by means of dual-source imaging, the homologous high-voltage fast switching technique, continuous dual fast scanning under homologous high and low voltages, superimposed detectors, and other techniques. DECT is widely accepted for obtaining virtual noncontrast images, displaying gout, analyzing stone components, and other uses.
Basic DECT studies have shown that although some soft tissues, including tendons, ligaments, and cartilage, mainly comprise components with a small atomic number, their X-ray attenuation coefficients are similar; this limits imaging contrast and resolution. However, densely packed hydroxylysine and hydroxyproline in the side chains of collagen molecules in these structural components have obvious attenuation differences from X-rays with different energies.7,8 Correspondingly, changes in the CT values of soft tissues under X-rays with different energies provide a new angle to obtain tissue-specific images of tendons and ligaments based on their histochemical composition, which are blind to traditional CT. Sun et al. 9 reported that dual-source DECT imaging can clearly display parameters such as the shape, path, and edge of the cruciate ligament in two- and three-dimensional modes, showing details in multiple directions and angles. Fickert et al. 4 and Peltola and Koskinen 5 also showed the use of DECT for the diagnosis of cruciate ligament injuries in piglet models as well as human patients. Regardless, radiation damage caused by CT in patients is an important issue that cannot be overlooked.
Since the advent of CT in the 1970s and its subsequent clinical application, its ever-increasing application demands have led to a significant increase in the annual average effective radiation dose in the population, with the potential related risks attracting increasing attention. Studies have shown that children and adolescents are 10 to 15 times more sensitive to radiation than adults. 10 Administration of relatively high radiation doses increases the potential for harm to both patients and medical staff. Therefore, the radiation dose has currently become the focus of attention. The as low as reasonably achievable (ALARA) principle was proposed for this reason. 11 The radiation dose should be minimized to the greatest degree possible under the premise of meeting the requirements for clinical diagnosis. The concept of low-dose techniques has been rapidly applied to practical work since its description in 1990.
As a large load-bearing joint in the human body, the knee joint has a relatively stable anatomical structure and few developmental variations. Its main components, including the anterior and posterior cruciate ligaments in the joint cavity, are generally clear with the surrounding tissue and have good image recognition. Although low-dose scanning increases image noise, it does not substantially interfere with bony structure observation. The post-processing technique of DECT can be used to color-code the anterior and posterior cruciate ligaments. Combined with multiplanar reconstruction of volume data, the negative impact caused by an insufficient dose can be counterbalanced to some extent.
Under the premise of not affecting the image quality, the scanning parameters in DECT cruciate ligament imaging should be optimized as much as possible, and targeted scanning should be carried out to achieve the ALARA principle in clinical application. In other words, the lowest possible dose should be used while simultaneously meeting the clinical requirements. Therefore, a balance should be achieved between image quality and radiation dose. In the present study, the objective evaluation results of image quality were not significantly different between the low- and standard-dose groups. There were also no statistically significant differences in the two experts’ subjective evaluation of images between the two groups. These findings indicate that the image quality using a low dose can fully meet the requirements for clinical diagnosis while greatly reducing the radiation dose (by 42.2% on average). This can substantially benefit the patients by protecting them from radiation damage and subsequent adverse effects.
When applied to knee joint scanning, the advantages of DECT are not limited to better display of the bone; visualization of soft tissues such as ligaments is also enhanced. Additionally, compared with MRI, CT has the advantages of fast scanning, high patient tolerance, fewer contraindications, and low examination cost. It can serve as an effective supplement to MRI and may even constitute the first-choice imaging technique for patients who cannot undergo MRI.
This study had two main limitations. First, this pilot study had a limited number of samples because of low sample availability. However, the number of included samples was still adequate to answer the essential question of the study. Second, the study employed ex vivo samples. When transferred to in vivo application, the conclusions may not be applied to the injured ACL because the boundary between the ACL and surrounding tissues may not be clear. Therefore, further studies are required to focus on these issues.