
Abstract
Objective
This study was performed to determine the outcomes of patients with coronavirus disease 2019 (COVID-19) who developed hypoxemic respiratory failure necessitating high-flow nasal cannula (HFNC) therapy and to identify the predictors of HFNC therapy success.
Methods
This retrospective observational study involved all patients treated with HFNC therapy at a center for COVID-19 in Viet Nam from August to October 2021.
Results
The study recruited 302 patients. Of these 302 patients, 171 (56.6%) underwent successful HFNC therapy, and the all-cause mortality rate was 33.44%. Non-critical COVID-19 and a higher respiratory rate–oxygenation (ROX) index at 48 hours after initiating HFNC therapy were independently correlated with HFNC therapy success. The statistically significant predictors of HFNC therapy success were younger age, non-critical COVID-19, a higher platelet count when starting HFNC therapy, and a higher ROX index at 24, 36, and 48 hours after HFNC therapy initiation.
Conclusions
HFNC therapy appears to be effective in patients with COVID-19 who develop respiratory failure requiring respiratory support. Non-critical COVID-19 and a higher ROX index measured 48 hours after HFNC therapy initiation might serve as predictive factors for the success of HFNC therapy.
Keywords
Key messages
The success rate of HFNC therapy in patients with severe and critical COVID-19 was 56.6%, suggesting that this modality might be effective in this group of patients. Non-critical COVID-19 and a higher ROX index 48 hours after initiating HFNC therapy were independently correlated with the success of HFNC therapy. The initial ROX indices were indicative of HFNC therapy failure, whereas the subsequent ROX indices, particularly at the 48-hour time point, were predictive of HFNC therapy success.
Introduction
At the end of 2019, the newly emerging severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) began to spread throughout the continents, resulting in infection of more than 500 million people and death of 6.2 million people globally. As of 12 April 2022, the number of registered cases of coronavirus disease 2019 (COVID-19) in Viet Nam was 10 million, causing approximately 43,000 deaths. 1 Two studies in Wuhan, China in late 2019 to early 2020 showed that acute respiratory distress syndrome occurred in 20% to 42% of patients with COVID-19, and the percentage of patients requiring invasive mechanical ventilation (IMV) was 12.3%.2,3 This overwhelmed the intensive care units (ICUs), especially in vulnerable healthcare systems.
In recent years, high-flow nasal cannula (HFNC) therapy has gradually become a new effective, safe, and well-tolerated method of noninvasive respiratory support. 4 An experimental study demonstrated that HFNC therapy did not spread virus-containing aerosols more than an oxygen mask with a reservoir bag. 5 In addition, beneficial effects of HFNC therapy have been demonstrated in patients with hypoxemic respiratory failure.6–8 However, prolonged and unmonitored HFNC support may harmfully delay timely intubation and necessary IMV, leading to poorer outcomes in patients with severe and critical COVID-19. 9
In Viet Nam, HFNC therapy has been widely adopted in the last 2 years to cope with the surges of the COVID-19 pandemic. Different protocols of HFNC therapy, most of which were slightly modified from international experience, have been used in different centers. To the best of our knowledge, however, no study has focused on HFNC therapy in patients with COVID-19 in Viet Nam, the healthcare system of which is much different from that in developed countries, where most studies of HFNC therapy have been conducted. We performed the present study with two objectives: first, to determine the outcomes of patients with COVID-19 who developed hypoxemic respiratory failure and received HFNC therapy during their hospital stay, and second, to identify the predictors of HFNC therapy success in this specific group of patients.
Materials and methods
Study design
This observational, retrospective, single-center study was conducted at a COVID-19 intensive care center from 2 August to 15 October 2021. The reporting of this study conforms to the STROBE guidelines. 10 The tertiary referral center involved in this study was established during the peak of the COVID-19 pandemic. This center catered to patients in a city of 10 million inhabitants. Patients were recruited into the study when they met the following criteria: clinical manifestations suggesting SARS-CoV-2 infection, confirmation of SARS-CoV-2 infection by real-time polymerase chain reaction, and respiratory failure necessitating a course of HFNC therapy during the ICU stay. We excluded all patients with an HFNC therapy duration of <30 minutes, patients who underwent post-extubation HFNC therapy, patients who underwent HFNC therapy as a last resort when they or their relatives refused intubation because of old age with frailty or multiple final-stage comorbidities, and patients who began HFNC therapy before admission to our center.
We only recruited patients who began HFNC therapy in our center. HFNC therapy was indicated in patients who met at least one of the following two criteria: hypoxemic respiratory failure with pulse oxygen saturation of ≤92% despite conventional oxygen therapy (nasal cannula or face mask oxygenation), 11 or pulse oxygen saturation of ≤92% and the presence of respiratory effort such as an increased respiratory rate and mobilization of accessory respiratory muscles. After starting HFNC therapy for each patient, we assessed the response to HFNC therapy (general status, utilization of accessory respiratory muscles, respiratory rate–oxygenation (ROX) index, and patient comfort) after 1, 2, 4, 8, 12, 24, 36, and 48 hours. The patients were then further assessed for their response to HFNC therapy on a daily basis until they no longer required HFNC, and their progress was monitored until discharge.
HFNC therapy failure was defined as worsening respiratory distress requiring endotracheal intubation and mechanical ventilation. Determination of HFNC therapy failure was based on the patient’s clinical condition as determined by the treating physician. Clinical criteria indicative of HFNC therapy failure included a respiratory rate of >30 breaths per minute despite optimal HFNC adjustment, evidence of paradoxical chest wall movement after HFNC use, and an arterial pH of ≤7.2.
The HFNC machines used in this study were an Airvo 2 (Fisher & Paykel, Auckland, New Zealand), VUN-001 (Vincent Medical, Hung Hom, Kowloon, Hong Kong), and NF5 (Shenzhen Comen Medical Instruments, Shenzhen, China). Based on the in-house protocol regarding the indications for HFNC therapy and its subsequent monitoring, adjustment, and termination, the physician in charge determined the whole regimen of HFNC therapy for each patient. Only in some borderline clinical situations was the decision regarding therapy made after consulting an experienced intensivist or, rarely, a group of intensivists.
Data collection
The following patient data were collected from the electronic medical records: demographic characteristics, comorbidities (cardiovascular disease, diabetes, chronic renal failure, and chronic lung diseases), COVID-19 vaccination and focused information related to diagnosis and management of COVID-19 before the current admission, clinical characteristics (vital signs on admission, when starting HFNC therapy, and during HFNC therapy until termination of HFNC, as well as other relevant morbidities), severity of COVID-19, laboratory results upon starting HFNC therapy, chest X-ray findings on admission and upon starting HFNC therapy, HFNC therapy setting and ROX index throughout HFNC therapy, other relevant management, and outcomes (durations of HFNC therapy, IMV, and hospital stay, as well as clinical status on discharge). If available, information on antibiotic therapy, corticosteroid therapy, anticoagulant medications, remdesivir, tocilizumab, and baricitinib was also collected.
The laboratory results selected for analysis were those obtained at the shortest interval from the start of HFNC therapy. When the results were obtained >24 hours after starting HFNC therapy, we excluded the patients from the study. The lung lesion severity was classified based on the simplified Radiographic Assessment of Lung Edema (sRALE) 12 : a score of 0 to 4 was assigned to each lung depending on the extent of involvement by consolidation or ground-glass opacities (0: no involvement, 1: <25% involvement, 2: 25%–50% involvement, 3: 50%–75% involvement, and 4: >75% involvement). The scores for each lung were summed to produce the final severity score.
The ROX index is the ratio of blood oxygenation and the respiratory rate and is calculated as follows
13
:

In this study, the ROX index was collected at 1, 2, 4, 8, 12, 24, 36, and 48 hours after initiation of HFNC therapy.
Statistical analysis
The collected data were coded and archived using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). The statistical analysis was performed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was performed to check the normality of the distribution of continuous variables. Continuous variables with a normal distribution are expressed as mean ± standard deviation. The independent-samples t-test or one-way analysis of variance was used to compare the means between the HFNC therapy failure and success groups. Continuous variables without a normal distribution are expressed as median (interquartile range), and the Mann–Whitney U test was used for comparison. A global mixed-effects linear model was used to compare the ROX indices between the HFNC therapy failure and success groups at each time point. Categorical variables are expressed as percentages and were compared using the chi-square test. Univariate and multivariate logistic regressions were performed to determine the independent predictors of HFNC therapy success. We selected variables showing a statistically significant correlation with HFNC therapy success in the univariate analysis for inclusion in the multivariate model. We then narrowed down the selection to include only factors that had a significant correlation with HFNC therapy success (p-value of <0.001) in the final multivariate model. When performing the multivariate regression, we excluded patients who had undergone HFNC therapy for <24 hours to avoid interference because these patients did not have ROX index results at the 24-, 36-, and 48-hour time points after starting HFNC therapy. Missing values were imputed using multiple imputation by chained equations with the predictive mean matching method. The discriminating power of predictors was calculated using a receiving operating characteristics (ROC) curve and the area under the ROC curve (AuROC). The cut-off value of each predictor was determined by the Youden method. The sensitivity, specificity, and positive and negative predictive values were calculated at the cut-off value. A p-value of <0.05 was considered statistically significant.
Research ethics
The present study was approved by our university hospital’s institutional review board (Approval No. 221/GCN-HDDD). Because of the city’s lockdown during the peak of the COVID-19 pandemic, informed consent for participation was not obtained. All methods were performed in accordance with the Declaration of Helsinki. Patients’ details were de-identified so that they may not be identified in any way.
Results
Of 350 patients with COVID-19 treated with HFNC therapy at our center, we recruited 302 patients for this study (Figure 1). Most of the patients had comorbidities (60.9% had hypertension, 38.1% had diabetes, and 14.9% had chronic coronary arterial disease), and 71.2% were not vaccinated against COVID-19. Laboratory results indicated an increased inflammatory reaction and acute hypoxemic respiratory failure with a significantly reduced PaO2/FiO2 ratio in the studied population at HFNC therapy initiation (Table 1).

Study flow chart. Pts, patients; RT-PCR, real-time polymerase chain reaction; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; HFNC, high-flow nasal cannula.
Laboratory results of the studied population at HFNC therapy initiation

Data are presented as mean ± standard deviation or median (interquartile range).
Independent-samples t-test, #Mann–Whitney U test.
ABG, arterial blood gas; ALT, alanine transaminase; AST, aspartate transferase; Cr, creatinine; CRP, C-reactive protein; Hb, hemoglobin; HFNC, high-flow nasal cannula; IL-6, interleukin-6; LDH, lactate dehydrogenase; PCT, procalcitonin; RBC, red blood cell count; WBC, white blood cell count.
In total, 171 (56.6%) patients were treated successfully with HFNC therapy. The ROX indices at 1, 2, 4, 8, 12, 24, 36, and 48 hours after starting HFNC therapy were significantly higher in the HFNC therapy success group than in the HFNC therapy failure group (Table 2). In particular, the difference in the ROX indices between the two groups became significantly noticeable after 12 hours (Figure 2).
Therapeutic characteristics and outcomes of the studied population.

Data are presented as n (%), mean ± standard deviation, or median (interquartile range).
Independent-samples t-test, ¶chi-square test, #global mixed-effects linear model.
DXM, dexamethasone; HFNC, high-flow nasal cannula; ICU, intensive care unit; PST, pulse corticosteroid therapy; ROX index, respiratory rate–oxygenation index.

ROX indices at different time points in the two study groups. *p < 0.05 for each time point
The mean hospital stay of the studied population was 20.38 ± 11.79 days. A total of 101 (33.44%) patients died (Figure 1). The HFNC therapy success group had a longer HFNC therapy duration (7.51 ± 5.85 vs. 4.65 ± 6.09 days, p < 0.001) but a shorter hospital stay (16.58 ± 7.65 vs. 23.26 ± 14.84 days, p < 0.001) and lower mortality rate (2.9% vs. 73.3%, p < 0.001) than the HFNC therapy failure group (Table 2).
The predictors of HFNC therapy success were younger age (AuROC, 0.686; p < 0.001), non-critical COVID-19 (0.803, p < 0.001), higher platelet count when starting HFNC therapy (0.693, p < 0.001), and higher ROX index at 24 hours (0.711, p < 0.001), 36 hours (0.740, p < 0.001), and 48 hours after beginning HFNC therapy (0.850, p < 0.001) (Figure 3). Notably, an ROX index cut-off value of ≥5.85 at 48 hours after starting HFNC therapy was the best predictor of HFNC success with a sensitivity of 77.2%, specificity of 73.9%, positive predictive value of 85.4%, and negative predictive value of 62.2% (Table 3).

Area under the ROC curve of different predictors of HFNC therapy success. HFNC, high-flow nasal cannula; ROC, receiver operating characteristic; ROX index, respiratory rate–oxygenation index; ROX24h, ROX index calculated at 24 hours after initiation of HFNC therapy; ROX36h, ROX index calculated at 36 hours after initiation of HFNC therapy; ROX48h, ROX index calculated at 48 hours after initiation of HFNC therapy.
Predictors of HFNC therapy success.
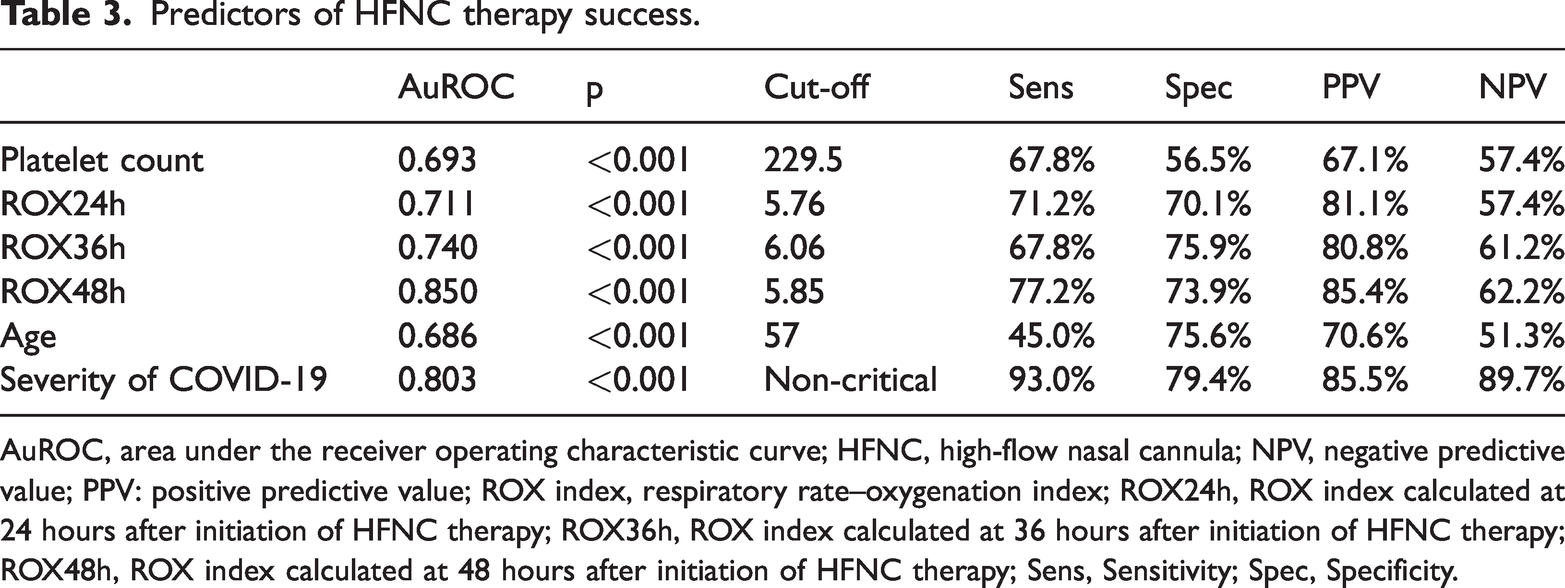
AuROC, area under the receiver operating characteristic curve; HFNC, high-flow nasal cannula; NPV, negative predictive value; PPV: positive predictive value; ROX index, respiratory rate–oxygenation index; ROX24h, ROX index calculated at 24 hours after initiation of HFNC therapy; ROX36h, ROX index calculated at 36 hours after initiation of HFNC therapy; ROX48h, ROX index calculated at 48 hours after initiation of HFNC therapy; Sens, Sensitivity; Spec, Specificity.
The univariate analysis showed that HFNC therapy success was associated with younger age, non-diabetes, non-critical SARS-CoV-2 infection, no bacterial pneumonia, lower heart rate, higher PaO2/FiO2 ratio, higher platelet count, lower blood urea concentration, lower sRALE score, and higher ROX indices at 24, 36, and 48 hours after starting HFNC. The multivariate analysis revealed the following independent factors associated with HFNC success: non-critical SARS-CoV-2 infection and higher ROX index at 48 hours after starting HFNC therapy (Table 4).
Univariate and multivariate logistic regression of different candidate predictors of HFNC therapy success (n = 254)
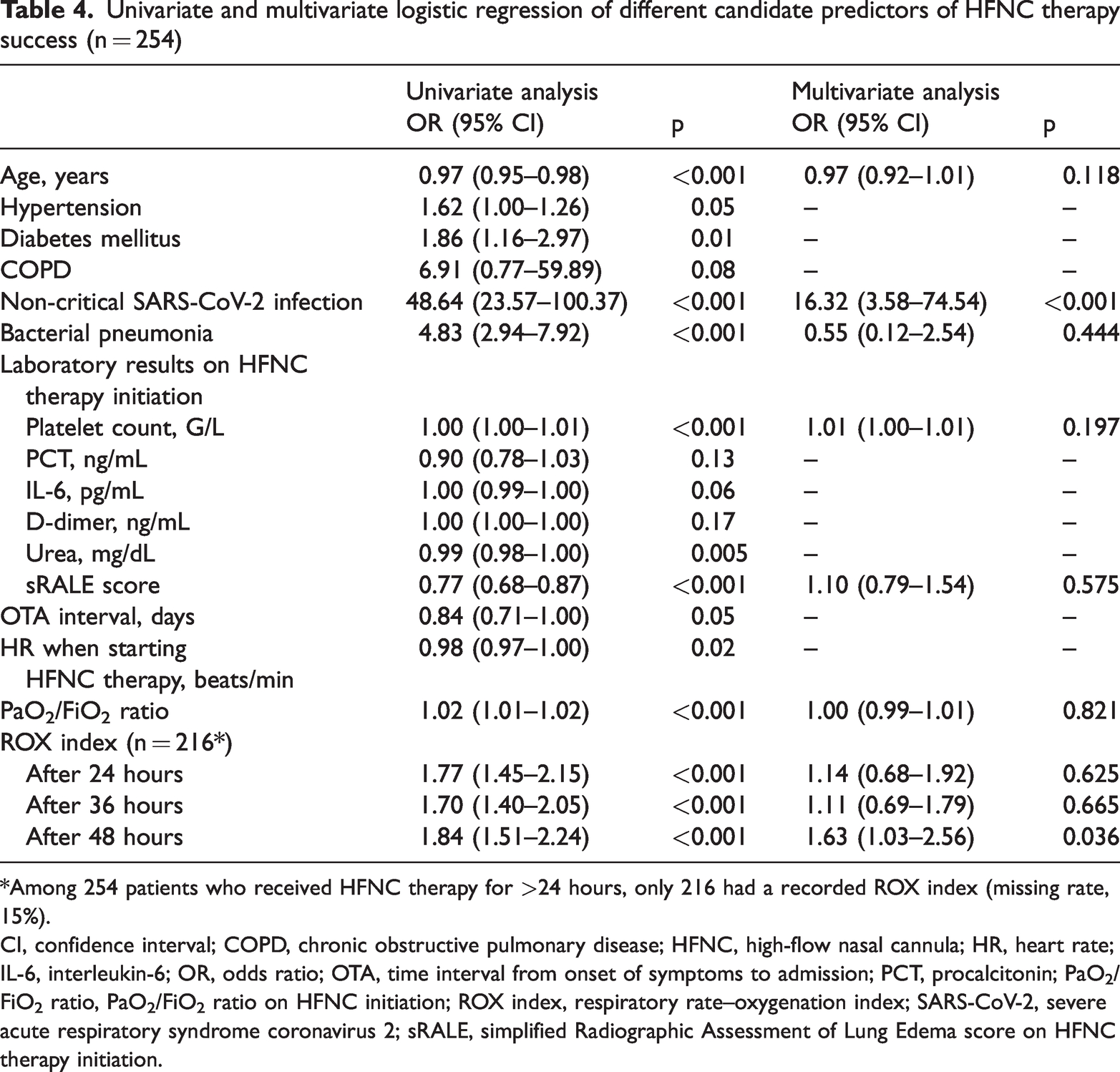
*Among 254 patients who received HFNC therapy for >24 hours, only 216 had a recorded ROX index (missing rate, 15%).
CI, confidence interval; COPD, chronic obstructive pulmonary disease; HFNC, high-flow nasal cannula; HR, heart rate; IL-6, interleukin-6; OR, odds ratio; OTA, time interval from onset of symptoms to admission; PCT, procalcitonin; PaO2/FiO2 ratio, PaO2/FiO2 ratio on HFNC initiation; ROX index, respiratory rate–oxygenation index; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; sRALE, simplified Radiographic Assessment of Lung Edema score on HFNC therapy initiation.
Discussion
Our study was conducted at an ICU in a field hospital built when COVID-19 peaked in our city of Viet Nam and claimed many lives. With the shortage of medical equipment, especially mechanical ventilators, HFNC therapy for patients with COVID-19 who developed hypoxemic respiratory failure was widely adopted. However, this modality also raised a serious question regarding whether HFNC therapy is really effective despite the bulk of literature from developed countries with far more effective healthcare systems and disaster preparedness. We expect the results of this real-world study to be helpful for both Viet Nam and countries with a similar level of development. The HFNC therapy success rate in our study was 56.6%, and the overall survival rate was 66.6%. This HFNC therapy success rate is comparable to that in other studies involving patients with COVID-19 in China, the United States, and Europe, where the success rate ranged from 52% to 62%.14–17 This high success rate in the context of a developing country with limited facilities and human resources is encouraging. HFNC therapy can be a reasonable choice for managing patients with severe and critical COVID-19 or other respiratory diseases in future. This is particularly important in developing countries with healthcare system capacities similar to those in Viet Nam.
In contrast to the high HFNC therapy success rate in our study and those mentioned above, Garner et al. 18 reported a much lower HFNC therapy success rate of only 23% in a study with a small sample of 30 patients with COVID-19. This discrepancy might be explained, at least in part, by the fact that the maximum flow rate was set at only 40 L/min in their study; this rate is considerably lower than that in our study. Mauri et al. 19 demonstrated that when increasing the flow rate from 30 to 60 L/min, the ROX index significantly improved, especially in patients with more severe hypoxemia. Higher inspiratory flow increases the positive end-expiratory pressure generated by HFNC therapy, improving blood oxygenation. Parke and McGuinness 20 demonstrated that positive end-expiratory pressure increased by approximately 1 cmH2O when the HFNC inspiratory flow rate was increased by 10 L/min. We started HFNC therapy with a flow rate of 50 to 60 L/min in all patients, and this practice might have contributed to our higher success rate.
Several factors can influence the patient’s response to HFNC therapy, such as underlying respiratory conditions (chronic obstructive pulmonary disease (COPD), asthma) or the use of corticosteroids. The proportion of patients with COVID-19 who had underlying COPD was significantly higher in the HFNC therapy failure than success group (3.9% vs. 0.6%, p = 0.04) (Table 5). However, HFNC therapy was successful in all patients with underlying asthma. The number of patients with underlying respiratory conditions in our study was small, and we did not collect information on the severity of COPD in these patients; therefore, we cannot draw a clear conclusion on this issue. Nonetheless, our findings in patients with COPD are similar to those reported by Xia et al., 21 who showed that HFNC therapy did not improve the intubation rate in patients with acute COPD exacerbation with mild respiratory distress. We also found no difference in the usage rate of corticosteroid therapy between the HFNC therapy success and failure groups (100.0% vs. 98.5%) (Table 2). The proportions of patients using different doses of corticosteroids between the two groups also showed no statistically significant difference; the low-dose, high-dose, and pulse steroid usage rates in the HFNC therapy success group were 28.7%, 56.1%, and 15.2%, respectively, and those in the failure group were 34.4%, 47.3%, and 16.8% (p = 0.203) (Table 2). Therefore, the effectiveness of HFNC therapy is not influenced by the presence or absence of corticosteroid treatment or by the dosage of corticosteroids. These results are consistent with the findings of the MEDEAS study. 22 The HFNC therapy success group showed a much lower mortality rate and shorter hospital stay than the HFNC therapy failure group: 2.9% vs. 73.3% (p < 0.001) and 16.6 ± 7.7 vs. 23.3 ± 14.8 days (p < 0.001), respectively. The COVID-ICU study, which involved 1491 patients with COVID-19 who were not intubated on admission to the ICUs in 137 European hospitals, showed that HFNC therapy was associated with a lower failure rate of oxygenation therapy (odds ratio, 0.60; 95% confidence interval, 0.36–0.99; p = 0.013), whereas noninvasive ventilation was associated with increased mortality (odds ratio, 2.75; 95% confidence interval, 1.79–4.21; p < 0.001). 17 Moreover, the SOHO-COVID study in 34 ICUs in France, including 711 patients with respiratory failure due to COVID-19, showed that the intubation rate was significantly lower with high-flow oxygen than with standard oxygen (45% [160/357] vs. 53% [186/354]; absolute difference, −7.7% [95% confidence interval, −14.9% to −0.4%]; p = 0.04). 23 Successful HFNC treatment helps circumvent intubation and complications secondary to IMV, such as ventilator-associated pneumonia, ventilator-induced lung injury, barotrauma, and volutrauma. Furthermore, a lower rate of intubation among patients undergoing HFNC therapy can allow the limited number of available ventilators to be used for patients with a definite need for IMV. This may play an important role in resource allocation in low- and middle-income countries coping with the overwhelming pandemic.
Patients’ clinical characteristics and disease severity at HFNC therapy initiation

Data are presented as mean ± standard deviation or n (%).
Independent-samples t-test, ¶chi-square test.
COPD, chronic obstructive pulmonary disease; DBP, diastolic blood pressure; HFNC, high-flow nasal cannula; OTA, time interval from onset of symptoms to admission; ROXi, respiratory rate–oxygenation index; SBP, systolic blood pressure; sRALE, simplified Radiographic Assessment of Lung Edema.
It is important to quickly identify patients who are likely to fail to respond to HFNC therapy and those who will benefit from this support technique. This stratification helps optimize the most practical therapeutic strategy and develop a suitable monitoring plan. Delays in intubation and IMV can increase patient-induced lung injury, respiratory muscle exhaustion, and mortality. By contrast, hasty intubation and IMV while patients can instead be successfully managed with HFNC therapy can lead to high costs, ventilator-associated pneumonia, and other complications. This contributes to increased mortality and overloads the healthcare system, which is already weakened by the pandemic.
In the current study, we found that younger age, a lower sRALE score, and higher PaO2/FiO2 ratio were associated with a higher HFNC therapy success rate. These findings are in agreement with those reported by Xu et al., 24 who also found that the above-mentioned factors were associated with a higher chance of developing acute respiratory distress syndrome. Coagulation disorders, thrombosis, and endothelial dysfunction are often seen in patients with COVID-19, especially those in the ICU.25,26 Thrombocytopenia has been shown to be associated with an unfavorable prognosis.27,28 Additionally, Katsoularis et al. 29 showed that higher D-dimer levels were associated with an increased risk of HFNC therapy failure. The reason for this association might be the presence of pulmonary emboli and/or increased inflammation. 29
Previous studies have demonstrated that the ROX index can predict the patient’s respiratory response to HFNC therapy. One study showed that a ROX index of ≥4.88 was consistently correlated with a reduced intubation rate at any time during the course of HFNC therapy, whereas a ROX index of <3.85 at 12 hours after starting HFNC therapy predicted the failure of this technique. 30 Hu et al. 16 also found that in patients with COVID-19, the ROX indices at 6, 12, and 24 hours after starting HFNC therapy predicted HFNC therapy success with AuROCs of 0.798, 0.820, and 0.874, respectively. Our study similarly showed that the ROX index at any time point during HFNC therapy was significantly different between the success and failure groups. However, the multivariate logistic regression did not show a correlation between the ROX index before 36 hours and success of HFNC therapy. Several studies have shown that a low ROX index 6 hours after beginning HFNC therapy predicted failure of HFNC therapy.16,30,31 Patients with COVID-19 who have a low ROX index at early time points (≤6 hours) after starting HFNC therapy are usually simultaneously affected by more severe respiratory manifestations, making the management decision straightforward. A recent meta-analysis showed that the ROX index at 6 hours after starting HFNC therapy most effectively predicted failure of HFNC therapy in patients with COVID-19, 32 whereas another meta-analysis showed that the ROX index at a later times better predicted the patient’s response to HFNC therapy. 33 Although early prediction of HFNC therapy failure is well established, prediction of success seems more difficult in the early hours of HFNC therapy and hence requires a longer observation period. If the ROX index remains high or improves, HFNC therapy success is certain. At the bedside, we identified a relatively large number of patients whose ROX index at 6 hours and even at 24 hours after starting HFNC therapy was low and met the criteria of HFNC therapy failure, but these patients’ clinical status and respiratory function were relatively stable. In such cases, we should not immediately intubate and start IMV because of its inherent potential complications. A more conservative approach involving thorough and regular assessment of the ROX index and the patient’s general status might be more beneficial. This delay is also the period during which other therapeutic interventions (antiviral antibiotics, anticoagulants, corticosteroids, and prone positioning) are expected to exert their effectiveness. We presume that a mindful delay in intubation and IMV can reduce complications and increase the chance of survival. Our study showed that the difference in the ROX indices between the success and failure groups was more pronounced from 24 to 48 hours after beginning HFNC therapy than before 24 hours (Figure 1). Therefore, the ROX index at 48 hours after starting HFNC therapy appears to be a clinically relevant predictor of HFNC therapy success.
The present study had some limitations that need to be addressed. First, this was a retrospective investigation at a single center; therefore, the findings cannot be generalized without critical evaluation. Second, at any given time point after starting HFNC therapy, either not all patients were evaluated for the ROX index or the ROX index was calculated but not documented if the management was not changed. Third, there might have been competitive risk between death (or live ICU discharge) and the HFNC success/failure rate, but we were not able to analyze the immortal time bias. Fourth, we started prone positioning quite early in most patients, but we did not issue any institutional guidelines for the initiation, management, or termination of prone HFNC therapy. The decision to use prone positioning was largely dependent on each physician in charge and the patient’s cooperation. This practice might have affected the patient’s response to HFNC therapy. Unfortunately, we were unable to delineate the impact of different regimens of prone positioning in patients undergoing HFNC therapy.
Conclusion
HFNC therapy might be effective in patients with COVID-19 who develop respiratory failure necessitating respiratory support to maintain adequate oxygenation. This noninvasive respiratory support technique was successfully applied during the turmoil of the COVID-19 pandemic at a field ICU in a developing country with a shortage of well-trained intensivists and medical equipment. Non-critical severity of COVID-19 and a higher ROX index at 48 hours after HFNC therapy initiation might help predict the success of HFNC therapy. We hope that our encouraging results in Vietnamese patients with COVID-19 will stimulate further investigations of HFNC therapy in ICUs, especially in developing countries.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231193580 - Supplemental material for High-flow nasal cannula therapy in patients with COVID-19 in intensive care units in a country with limited resources: a single-center experience
Supplemental material, sj-pdf-1-imr-10.1177_03000605231193580 for High-flow nasal cannula therapy in patients with COVID-19 in intensive care units in a country with limited resources: a single-center experience by Anh-Minh Vu Phan, Hai-Yen Thi Hoang Thanh-Son Truong Do, Trung Quoc Hoang Thuan Van Phan Nguyet-Anh Phuong Huynh Khoi Minh Le in Journal of International Medical Research
Footnotes
Authors’ contributions
Acknowledgement
We sincerely thank Phung Tran Huy Nhat (Oxford University Clinical Research Unit, Ho Chi Minh City) for assisting with the data analysis.
Data availability statement
The data supporting this study’s findings are available on request from the corresponding author (KML).
Declaration of conflicting interests
The authors declare no potential conflict of interest relevant to this article.
Funding
The authors did not receive any financial support for performing this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.