
Abstract
Flexible video bronchoscopy is a procedure that plays an important role in diagnosing various types of pulmonary lesions and abnormalities. Case 1 is a 68-year-old male patient with a lesion in the right lung apex of approximately 4 mm × 28 mm with atelectasis bands due to a crash injury. High-flow system with 35 L/min and fraction of inspired oxygen (FiO2) 0.45 and temperature of 34 °C was installed prior to the video bronchoscopy. SpO2 was maintained at 98%–100%. The total dose of sedative was 50 mg of propofol. In Case 2, a 64-year-old male patient with bronchiectasis, cystic lesions and pulmonary fibrosis of the left lung field was placed on a high-flow system with 45 L/min and 0.35 FiO2 at a temperature of 34 °C. SpO2 was maintained at 100%. The total duration of the procedure was 25 min; SpO2 of 100% was sustained with oxygenation during maintenance time with the flexible bronchoscope within the airway. The total dose of propofol to reach the degree of desired sedation was 0.5–1 mg/kg. Both patients presented hypotension. For the patient of case 1, a vasopressor (norepinephrine at doses of 0.04 µg/kg/min) was given, and for the patient of case 2, only saline volume expansion was used. The video bronchoscopy with propofol sedation and high-flow nasal cannula allows adequate oxygenation during procedure in the intensive care unit.
Introduction
In the intensive care unit (ICU), flexible video bronchoscopy (FVB) is often used in the lower respiratory tract for resolution of mass atelectasis and to wash the lung in certain clinical conditions, especially in intubated patients; in these last FVB scenarios, the patient usually requires intubation with some form of invasive ventilatory support. 1 In the daily practice in the ICU, FVB is performed when the patient could not be intubated or could not undergo a tracheostomy. For ventilated patients, it is used when emergency removal of secretions is indicated. These common scenarios in the ICU are examples of FVB use aside of diagnostic evaluations.
It is important to note that inserting a bronchoscope into the respiratory tract may cause a decrease in minute ventilation, an increase in resistance in the airway and hypoxemia by decreasing the tracheal lumen. Therefore, this procedure entails a significant risk for cardiorespiratory complications. 2 However, the use of noninvasive ventilation (NIV) as an alternative for intubation to prevent respiratory failure is generally associated with better outcomes. 3 Recently, it was shown that lung lavage with flexible bronchoscopy (FB) is facilitated by NIV. 4
A potential alternative of NIV to treat respiratory failure is the nasal delivery of high-flow oxygen which refers to the entry of air and oxygen through a humidifier in a high-flow circuit. It has been shown that a flow of air of 40 L/min is well tolerated in adults and that the gas flowing during inspiration is maintained at the appropriate temperature and humidity. One study demonstrated that this method was even more comfortable for patients than other ventilator mechanisms. 5
Studies about high-flow nasal cannula (HFNC) and bronchoscopies have been performed in different clinical scenarios. 6 Some studies have focused on hypoxic and non-hypoxic ICU patients for whom HFNC was used as preoxygenation for anesthesia. 7 In addition, recent studies have shown the advantages of the use of high flow during flexible bronchoscopy (FB) in preventing hypoxemia compared with standard treatment.8,9
Here we present the cases of two ICU patients with hemoptysis who underwent FVB according to protocol using HFNC and propofol sedation.
Case reports
Case 1
A 68-year-old male patient had been hospitalized for 5 days after presenting in the emergency department with respiratory distress, dyspnea and hemoptysis. The patient complained of dyspnea, cough and hemoptysis lasting 1 month, in addition to significant weight loss of >15 kg over the previous 3 months. The patient was scheduled for FVB.
In his medical history, the patient had hypertension and type II diabetes, treated with Losartan 50 mg and intermediate acting insulin (NPH human insulin). As for his surgical history, he had a prostatectomy and cardiac catheterization for an acute myocardial infarction (AMI) 1 year prior to this hospitalization. Laboratory studies included a complete blood count that showed hemoglobin of 11 g/dL (normal range, 12–16 g/dL) and glucose of 298 mg/dL (normal range, 70–110 mg/dL)
A computed tomography (CT) scan of the thorax including a pulmonary window revealed a rounded hyperdense image of 4 mm × 28 mm with poorly defined borders in the right upper lobe.
Initial vital signs included blood pressure of 120/65 mmHg, heart rate of 82 bpm, and SpO2 of 96%. Initial arterial blood gas (ABG) analysis showed pH 7.52, pCO2 44 mmHg, PaO2 87 mmHg, HCO3 32.1 mmol/L, BE 3.9 mmol/L, and SaO2 95% with oxygen cannula at 3 liters per minute (FiO2 30%).
The bronchoscope (brand The PENTAX Medical) was used for the FVB. The HFNC oxygenation system (AIRVO™ 2 Fisher & Paykel Healthcare System) was installed prior to the FVB with the flow of oxygen adjusted to 35 L/min, FiO2 45% and temperature of 34 °C. SpO2 was maintained at 98%–100%. After 20 min, ABG analysis with the HFNC showed pH 7.45, pCO2 38 mmHg, PaO2 92 mmHg, HCO3 26.4 mmol/L, BE 2.4 mmol/L, and SaO2 98%–100%. The total time of procedure was 30 min, and a SaO2 of 98% was maintained during the time the FB was within the airway.
Sedation with propofol 1% was administered at an initial dose of 0.5–1 mg/kg to reach the degree of desired sedation (total dose: 75 mg). The patient developed hypotension during the procedure; therefore, a bolus of 500 mL of normal saline was administered and due to the persistence of hypotension, doses of 0.04 µg/kg/min norepinephrine were instituted.
The patient was discharged to the ICU after the 1-hr procedure without vasopressor support and was able to breathe in ambient air without complications.
Written informed consent was obtained from the patient.
Case 2
A 64-year-old male patient was admitted to the ICU after presenting with hemoptysis and chills.
Physical examination showed bilateral breathing sounds with fine crackles in the left basal and apical fields. His medical history was consistent with smoking, former alcoholism, and hypertension treated with Losartan. He did not have a surgical history. His CT scan of the thorax showed the presence of cystic bronchiectasis and areas of fibrosis in the apex of the left lung (Figure 1).

CT scan of the chest in lung window showing (a) a poorly defined, hyperdense image with round edges in the right upper lobe and (b) a residual fibrosis area and areas of cystic bronchiectasis in the left upper lobe.
Initial vital signs included blood pressure of 110/70 mmHg, heart rate of 74 bpm, and SpO2 of 94%. Initial analysis of ABG showed pH 7.37, pCO2 41 mmHg, PaO2, 77 mmHg, HCO3/L 28.3 mmol, BE 2.9 mmol/L and SaO2 94% with oxygen cannula at 3 liters per minute. (FiO2 30%)
The bronchoscope (brand The PENTAX Medical) was used for the FVB HFNC oxygenation system (AIRVO System™ 2 Fisher & Paykel Healthcare) and was pre-installed for FVB with the flow of oxygen adjusted to 45 L/min and FiO2 35% and temperature of 34 °C. SpO2 was kept at 100% during the 25 min the FB was within the airway. The total time of procedure was approximately 35 min starting from the introduction of the bronchoscope.
Propofol sedation at 1% was administered at an initial dose of 0.5–1 mg/kg to reach the desired degree of sedation. The total dose in this patient was 50 mg. The patient developed hypotension during the procedure; therefore, a bolus of 500 mL of normal saline was administered. The patient was discharged after the 1-hr long procedure to the ICU without complications and being able to breathe in ambient air.
The decision to use HFNC for both patients was due to the risk of hypoxemia as a consequence of airway narrowing when introducing the FVB, specifically in patients with chronic lung diseases. In addition, the possible hypotensive effects of the use of propofol should be considered. HFNC was kept for 15–30 min after the FVB procedure was completed in both patients.
Written informed consent was obtained from the patient.
Discussion
We present two clinical cases in which we successfully performed FVB with HFNC and propofol sedation in the ICU.
HFNC is easy to use in endoscopic procedures due to its ability to provide stable FiO2 delivery while providing high rates of airflow with minimal interference of endoscopic devices inserted via different routes. Moreover, HFNC can create a positive end-expiratory pressure to prevent variations in the expiratory flow. 6 Some studies have reported cases of other medical specialties in which the high-flow nasal cannula oxygen delivery has been beneficial, thus the feasibility of applying this technique to other fields should be considered.
Despite the fact that the benefit of high-flow nasal oxygen (HFNO) has been observed between 30 and 70 L/min in adults, there is an improved washing of the air that does not contain oxygen as the flow rate increases. This effect is especially seen in the oral cavity. Consequently, the speed of secretions and possibility of obstruction of the airway could increase without the use of high-speed flow of oxygen. In our management, we used a flow rate in the range 30–40 L/min, which allows an efficient supply of air and oxygen. 7
In the case of our first patient, he presented with hemoptysis and baseline SO2 of 95%, whereas our second patient presented with a baseline SO2 of 94% with moderate secretions due to the presence of cystic bronchiectasis. Both patients underwent bronchoalveolar lavage and biopsy; these procedures can lead to complications such as hypoxemia and risk of bleeding.
The use of HFNC for bronchoscopy protocol was efficient in the clinical cases presented. Patients undergoing this procedure frequently present hypoxemia, not only because the introduction of the bronchoscope into the airway decreases the lumen of the trachea by 10%–15%, but also because of the sedation used during the procedure. During the FVB procedure, the use of HFNC has been shown to prevent the deterioration of oxygenation, maintain an adequate tidal volume with preservation of diaphragmatic activity and less volume loss at the end of exhalation when compared with the standard procedure. 8 Other trials have also shown that HFNC used during FVB with transbronchial lung biopsy reduces the percentage of desaturations as well as the number of interventions and interruptions of the procedure. 9
In this setting, patients with chronic lung diseases could be at risk of experiencing hypoxemia during FVB. 10 In those patients with comorbidities and baseline SO2 of 94%–96% (Table 1), the introduction of FVB could cause deeper desaturations and increase the number of repetitive interventions in the airways with interruptions of the procedure.
Gasometric characteristics of both clinical cases pre and post FVB.
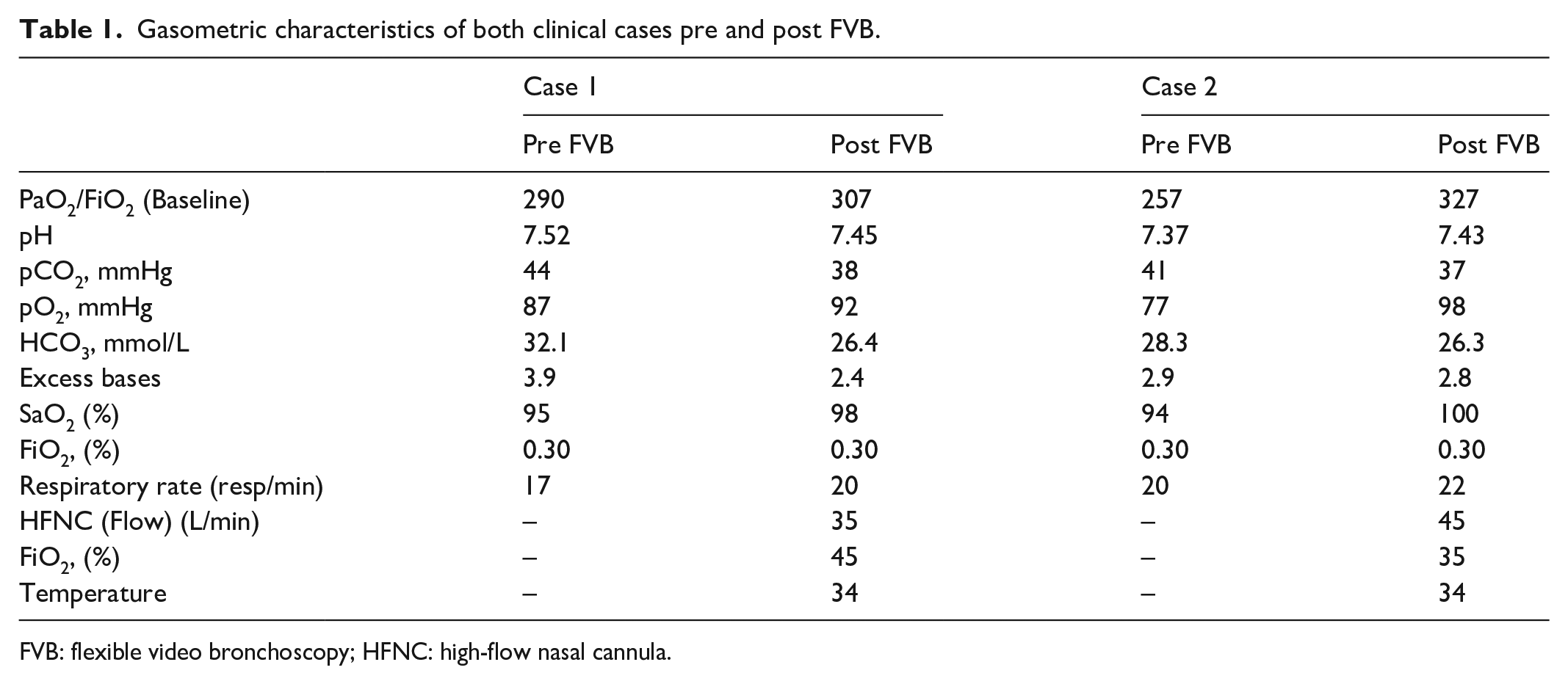
FVB: flexible video bronchoscopy; HFNC: high-flow nasal cannula.
Despite this, FVB provides greater pulmonary oxygen therapy and decreases inspiratory resistance. In this study, our two patients did not develop hypoxemia during the procedure, most likely due to the possibility to provide stable high rates of airflow and FiO2 through HFNC and minimal interference with the bronchoscope device inserted through the nostril. As the pharyngeal pressures increase, the HFNC promotes the opening of the superior airway, contributing to pulmonary recruitment and improving pulmonary CRF. 11 HFNC-related expenses are cost-effective in this case due to the benefits of better oxygenation, less procedure time and possibility of use in patients with prior lung diseases. 12
FVB is a procedure in which entry and exit of the airway could be repetitive with consequent pain, anxiety, dyspnea, and cough while passing the bronchoscope. Therefore, the British Thoracic Society (BTS) 13 recommends the use of sedation in the absence of contraindications in individuals undergoing an endoscopic procedure. Moreover, The American Society of Anesthesiology (ASA) recommends sedation guidelines with progressive degrees of sedation-anesthesia during FVB. 14 Furthermore, while under anesthesia, functional residual capacity (FRC) is decreased by 20%–25% in patients with previous pulmonary disease (e.g. cancer and chronic obstructive pulmonary disease, among others). General anesthesia can reduce lung capacity and can lead to subsequent postsurgical complications (e.g. intubation, severe hypoxemia).
For patients who have a tendency toward desaturation, bronchoscopy can entail a double risk due to the use of sedatives like propofol, which can exacerbate their condition. Propofol can have adverse effects due to its ability to induce hypoxemia through several mechanisms, including hypoventilation, airway collapse, and suction and retention of carbon dioxide (CO2). 15 On the flip side, studies have shown that propofol sedation is a safe 16 method when used during FVB. It can be done by pulmonologists, by physicians who are not anesthesiologists, and by nurses supervised by pulmonologists, as long as they have the knowledge and expertise with adequate monitoring and preparation to treat complications that could arise. 17
Other sedatives have been shown to have different safety profiles when used in FVB procedures. In this scenario, dexmedetomidine, despite not affecting ventilatory conduction, could produce adverse cardiovascular effects such as hypotension and bradycardia. On the other hand, midazolam, as well as other benzodiazepines, could produce desaturations and ventilatory depressive effects. 18
Our two patients were stable with adequate oxygen saturation with the use of high-flow oxygen through nasal cannula. There are cases reported of other specialties in which this method was beneficial, thus supporting the benefits of this technique. 15
Conclusion
Due to the presence of desaturations during the FVB procedure with affectations in the ventilatory impulse and in the ventilatory conduction, the HFNC could prevent hypoxemia as well as reduce the number of interventions and interruptions of the procedure in patients with chronic underlying disease at high risk of gas exchange disturbances.
It was shown in these two clinical cases that the HFNC technique combined with propofol sedation could be safe for performing bronchoscopy in a high-dependency area such as the ICU.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was approved by the Ethics Committee of Clinical Research of the Ecuadorian Institute of Social Security IEESS Babahoyo (IESS-HG-BA-DTMC-2019-1231 / CODIGO 003).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient.
Site where this research study was conducted
Intensive Care Unit, Ecuadorian Institute of Social Security (IESS), Babahoyo, Ecuador.