
Abstract
Currently, it is quite difficult to determine the best timeframe of operative treatment, as well as conduct surgery on asymptomatic COVID-19 patients due to misunderstandings and unawareness of the patient’s inflammation state. Caution needs to be taken in specific patient cohorts, particularly those with femoral shaft fractures, who are more likely to develop diseases like acute respiratory distress syndrome after a procedure like intramedullary nailing. In this case report, a 36-year-old patient suffered a motorcycle accident in which he suffered an ipsilateral femoral shaft and neck fracture of the hip. The patient’s screening test for COVID-19 was positive before admission. Because the patient did not display any COVID-19-related symptoms upon arrival to the hospital, surgical fixation with a reamed intramedullary femoral nail was performed. Despite having a successful post-surgical outcome, the patient was diagnosed with acute respiratory distress syndrome 36 h after surgery, recovering fully after about 2 weeks. To prevent subsequent complications such as acute respiratory distress syndrome in a high inflammatory state patient like COVID-19, the respiratory status and the degree of systemic inflammation should be considered precisely when determining the surgical timing and method.
Graphical abstract

Introduction
The coronavirus disease 2019 (COVID-19) outbreak has had a substantial influence on surgery delays worldwide. According to the National Health Service (NHS) guidelines, all elective surgeries should be postponed as late as possible. 1 However, typically when it comes to orthopedic surgery and fractures, it is recommended that surgery be performed earlier rather than later in order to obtain better outcomes. Surgery delays can have a negative impact on a patient’s prognosis which can be more harmful than some COVID-19-related complications. 2 Therefore, it is difficult to determine the best timing of surgery for COVID-19 patients with orthopedic fractures.
Acute respiratory distress syndrome (ARDS) is widely known as a life-threatening complication that can occur after reamed intramedullary (IM) nailing of the femur. Because it is understood that a patient’s inflammatory profile is associated with the onset of ARDS, a thorough evaluation of a patient’s inflammatory condition at the time of surgery should be done. 3
We present and discuss a case in which an asymptomatic COVID-19 patient with an ipsilateral femoral neck and shaft fracture suffered ARDS after the reamed IM nailing procedure.
Case
This study was conducted after approval of the Daegu Catholic University Medical Center Institutional Review Board (CR-22-018). An American Society of Anesthesiologists (ASA) grade I, 4 healthy 36-year-old male was admitted through emergency room after a motorbike accident. Upon arrival, the patient was alert and complained of a sharp pain on his left thigh. Physical examination showed swelling, a 1-cm open wound at the anterolateral thigh region, and a paradoxical movement in the middle portion of the left femur. A Pauwels classification type 3 femoral neck fracture and ipsilateral shaft fracture was found in the left femur after radiograph assessment (Figure 1(a)). Chest computed tomography (CT) showed a mild chest wall contusion without any lung lesions. The patient was confirmed to not have any life-threatening injuries. The Injury Severity Score was 17 points (Abbreviated Injury Scale 1 for thoracic, 4 for extremity).5,6 Initial lab findings included White blood cell count (7500), hemoglobin (12.6 g/dL), erythrocyte sedimentation rate (ESR) (7 mm/h), C-reactive protein (CRP) (1.1 g/dL), prothrombin time (PT) (11.6 s), and the activated partial thromboplastin time test (aPTT) (22.8 s). Initial arterial blood gas analysis (ABGA) showed a normal respiratory status (pH = 7.404, pCO2 = 41.3 mm Hg, pO2 = 84.8 mm Hg) and a viral nucleic acid test by way of a throat swab (a routine test for every patient who is admitted to our hospital) showed a positive COVID-19 test. 7 The patient was admitted to an isolated ward and treated with remdesivir (100 mg by IV) every 24 h and piperacillin/tazobactam (4.5 g by IV) 3 times daily. Immediately after taking the test, the patient showed no sign of COVID-19 symptoms such as a fever, cough, fatigue, or pulmonary lesion on a radiograph (Figure 2(a)). The patient had no previous treatment history, comorbidities, family history, allergy history, and was physiologically stable upon admission. Since the protocol for asymptomatic COVID-19 patients with femoral fractures in our hospital is performing a surgery under adequate protection, the surgery was proceeded under general anesthesia 48 h after admission. Forty-eighty hours after admission, surgery for an ipsilateral femoral neck and shaft fracture was performed with adequate precautions in-line with the standard COVID-19 protocols at our hospital.

Radiographic images of the left femur: (a) obtained at our emergency room showing a left ipsilateral femoral neck and shaft fracture; (b) plain radiographs of the left femur taken the day after surgery.
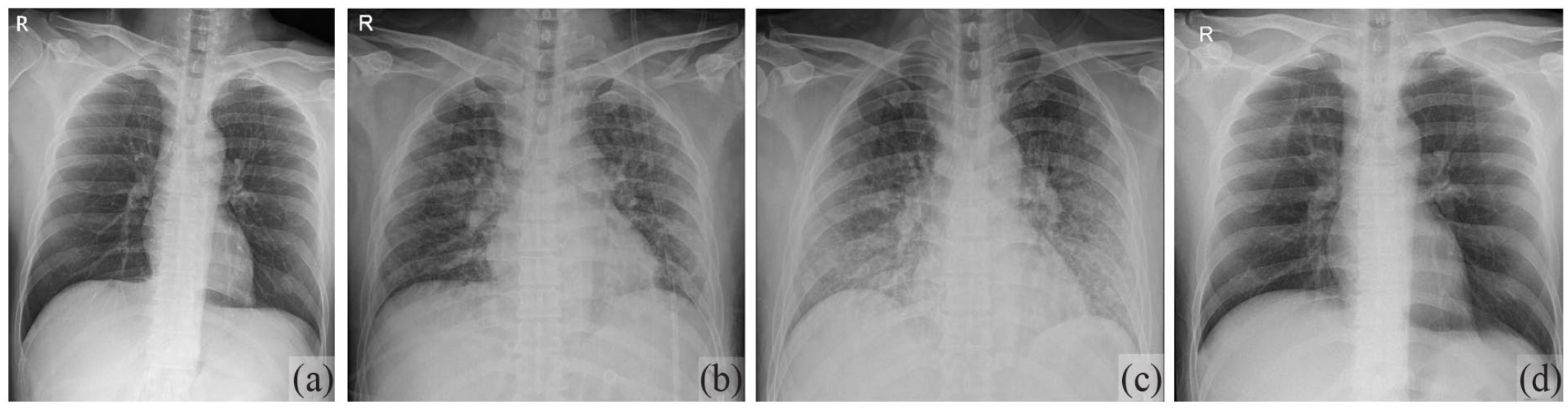
Radiographic images of the chest: (a) chest radiographs obtained at our emergency room indicates no active pulmonary abnormalities; (b) obtained on POD2, reveals bronchopneumonia with multiple patch consolidation in both lungs; (c) ARDS can be seen on POD3; (d) resolved lesion on POD 14.
All surgical procedures were conducted in a negative-pressure operating room dedicated to patients with contagious diseases. The room is located in a remote corner of the operation center with separate access. A biological isolation chamber with a negative-pressure filtration system was used to move the patient from the isolation ward to the operating room. The anesthesia doctor wore level D personal protective equipment with an N-95 facemask and air-purifying respirator. Due to the limited field of view while wearing level D protector, intubation was performed via video scope. Every staff who participated in the surgery wore level D personal protective equipment with N-95 facemasks. Surgery was performed on a fracture table. To manage the shaft and neck fracture of the femur, IM nail fixation with cephallomedullary screws was done after closed reduction (Figure 1(b)). The total surgery time was 45 min from skin incision to skin suture and the total amount of bleeding that occurred was 350 mL. The surgery was completed under standard respiratory and hemodynamic parameters, and postoperative radiographs displayed acceptable reduction and fracture fixation (Figure 1(b)).
Thirty-six hours after surgery, the patient presented with hypoxia (SpO2: 74%), fever (38°C), dyspnea, and a productive cough. Following chest radiograph examination, bronchopneumonia in both lungs with multiple patch consolidation was found (Figure 2(b)) and high flow nasal oxygenation (HFNO) was initiated. Since the patient’s symptoms did not improve as expected, continuous positive airway pressure (CPAP) was started at a pressure of 5 cmH2O at 4-h intervals. One day after CPAP therapy, chest radiographs showed aggravated pneumonia and the patient was diagnosed with ARDS using Berlin’s definition (Figure 2(c)). The most commonly used definition of ARDS, the Berlin definition defines ARDS by the presence within 7 days of a known clinical insult or new or worsening respiratory symptoms of a combination of acute hypoxemia (PaO2/FiO2 ⩽ 300 mm Hg), and bilateral lung opacities. 8 After the ARDS diagnosis, the patient was treated conservatively for both COVID-19 and ARDS before HFNO was successfully weaned off after 9 days. The patient was discharged from the hospital on day 14 after surgery (Figure 2(d)).
Discussion
During the COVID-19 pandemic, it became commonplace for patients with fractures to also arrive at the hospital with COVID-19. Because of this, it continues to be a challenge today for surgeons to determine the best timing of surgery as well as the best procedure method for treating concurrent COVID-19 fracture patients. While COVID-19 measures differ across nations, early surgeries are recommended universally for urgent or emergency cases in trauma and orthopedic fields. 2 When specifically looking at ipsilateral femoral neck and shaft fracture cases, such situations require urgent surgery, and thus need to be dealt with more quickly than normal. In the case of femoral fracture patients, ARDS is a common complication after surgery, exacerbated by the IM nailing golden standard of femoral fracture treatment. 3 However, Boose et al. have contested that IM nailing increases the incidence of ARDS after surgery in the general population. The authors compared two surgical methods (femur IM nailing and plating) between two groups (femoral fracture with or without thoracic injury). Neither of these groups had a significant difference in ARDS occurrence. 9
Therefore, it would be a dilemma for surgeons in selecting the surgical method and right timing when a COVID-19 patient needs surgery for femoral shaft fracture. Numerous other studies have suggested that delay of surgery may have a negative impact on the prognosis, which could be more harmful than the COVID-19-related complications. 2 Thus, early surgical intervention is recommended. On the contrary, COVID-19 infection might increase the risk of ARDS occurrence after surgery. It could be safer to perform the surgery after the recovery of COVID-19.
In our case, the patient did not show COVID-19 symptoms upon initial admission to the hospital. Therefore, we decided that surgery was the best course of action to improve mobility, healing, and pain control based on our hospital’s protocol. Unfortunately, the patient suffered ARDS on the 2nd day after surgery. Prior to this case, we performed surgeries on asymptomatic COVID-19 fracture patients predicting low probability of ARDS. However, in this particular case, the ipsilateral femoral neck and shaft fracture increased the risk for pulmonary complications such as ARDS. Extra caution and surgical planning are necessary when dealing with this specific patient cohort.
Typically in COVID-19 patients, inflammatory responses are dramatically heightened due to the large release of cytokines TNF-α, IL-1β, and IL-6 in the damaged tissue. In addition, when the IM reaming procedure is performed, which greatly increases the amount of inflammation in the body, the amount of inflammation in a patient’s body can reach a “tipping point,” leading to challenges such as ARDS.10–12 Currently, physicians nowadays determine the tipping point to be a state of clinical instability associated with microvascular injury, interstitial edema, hemodynamic lability, and end-organ failure. 13 Further, it appears as though IL-6 is the most important factor in inducing a flood of cytokines in the body that can leave a patient susceptible to infection, specifically those that are in the elderly population. 14 IL-6 has been found to be the cytokine that most influences coagulation activity and tissue factor in the body, both found to be higher in patients with COVID-19. 14 In order to best determine the total amount of inflammation in a patient’s body before surgery and the “tipping point,” IL-6 can be quantified, which has been shown to be related to multiple organ failures.
Asymptomatic COVID-19 patients have been shown to have subclinical levels of systemic inflammation caused by the virus. However, a hyperinflammatory response will occur when additional trauma and surgical procedures like IM reaming come into play. Together, COVID-19 infection, trauma, and surgical intervention can create a massive amount of cytokines in the body, leading to major inflammation and clinical instability. 15 When the amount of inflammation reaches an extremely high level, adverse outcome like ARDS will occur, which can lead to organ failure.13,16
In order to prevent these types of hyperinflammatory responses from occurring and to select the best surgical timing when dealing with COVID-19 femoral fracture patients, precise categorization of the severity of inflammation should be assessed prior to treatment. The severity of the COVID-19 can be assessed based on numerous factors (symptoms, comorbidities, age, laboratory findings, etc.). In terms of patient’s phenotype expressions, COVID-19 severity can be categorized using The National Institutes of Health guideline (Asymptomatic or Pre-symptomatic Infection; Mild Illness; Moderate Illness; Severe Illness; Critical Illness; see Appendix 1 for full description). 17 In terms of IL-6, for example, of inflammatory marker, there are two meta-analyses showing severe COVID 19 infection has 2.9-fold or +23.1 pg/mL higher levels of IL-6 compared to non-severe infection.18,19
If systematic inflammation has already reached a high level prior to surgical intervention, postponing surgery or alternative management like nonoperative treatment or damage control orthopedics should be considered. Even if the clinical symptoms of COVID-19 are not severe, the likelihood of developing ARDS after surgery is still higher in COVID-19 patients than non-COVID-19 patients. In terms of specific surgical treatments for these patients, those that do not involve the medullary canal should be considered or procedures involving excessive reaming should be avoided if IM fixation is performed. For instance, an unreamed femoral IM nail (UFN) could be an alternative choice of device rather than a reamed nail when looking at surgical options, due to specific advantages. 20 However, UFN usage is controversial as recent studies show similar risks for pulmonary complications and inferior clinical outcome (union rate and implant failure).21,22
This is the first study to describe the outcomes of an asymptomatic COVID-19 patient with an ipsilateral femoral neck and shaft fracture who developed ARDS after surgery.
Conclusion
There is a high risk of ARDS complications after surgery in the COVID-19 patient, even an asymptomatic one. To avoid such complications, it is important to determine the best timing and method of surgery by considering the inflammatory status of the patient. Precise and broad lab tests should be performed of multiple inflammation markers (ESR, CRP, IL-6, D-dimer, etc.), and pulmonary function data points (ABGA, etc.) to determine the severity of inflammation.
Footnotes
Appendix 1
Asymptomatic or Presymptomatic Infection: Individuals who test positive for SARS-CoV-2 using a virologic test (i.e. a nucleic acid amplification test (NAAT) or an antigen test) but who have no symptoms that are consistent with COVID-19.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g. fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath, dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have an oxygen saturation (SpO2) ⩾ 94% on room air at sea level.
Severe Illness: Individuals who have SpO2 < 94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mm Hg, a respiratory rate > 30 breaths/min, or lung infiltrates > 50%.
Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction
Author contributions
C.J., MD, contributed to draft manuscript preparation, analysis and interpretation of results. Y.-J.C., MD, contributed to data collection. P.M.Q., BA, contributed to draft manuscript preparation. S.-K.S., MD, contributed to study conception and design. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted after approval of the Daegu Catholic University Medical Center Institutional Review Board (CR-22-018).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.