
Abstract
During the coronavirus disease 2019 pandemic, Ecuador reported a collapse of the healthcare system, in which intensive care unit beds were lacking. Therefore, we sought to determine whether the use of threshold expiratory positive pressure with an adult non-rebreather oxygen mask plus prone positioning is useful for improving oxygenation. Twelve patients were included. Eight patients (66.7%) survived, while four patients (33.3%) died. Baseline arterial oxygen saturation (%) prior placement median (interquartile range) 85.5% (80%–89%) and arterial oxygen saturation (%) post placement of the device was median (interquartile range) (93%–96%) (P = 0.0001). Respiratory rate before placement was median (interquartile range) 38 (36–42) and post placement of the device was median (interquartile range) 24 (22–30) (P = 0.0005). The use of an adapted device might be useful for the management of acute hypoxemic respiratory failure due to severe acute respiratory syndrome coronavirus 2 pneumonia, particularly when mechanical ventilators and high-flow oxygen systems are unavailable.
Keywords
Introduction
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pneumonia associated with hypoxemic acute respiratory failure (HARF) and coronavirus disease-associated acute respiratory distress syndrome are currently the main causes of requests for medical assistance in hospitals globally. 1 In addition, the increase in patients in need of hospitalization during this pandemic rapidly exceeds the availability of resources, with a shortage of beds in intensive care units and equipment to support HARF, such as high-flow nasal cannula (HFNC), non-invasive mechanical ventilation (NIMV), and/or invasive mechanical ventilation (NIMV). Studies have shown that SARS-CoV-2 aerosolization might include several challenges when NIMV systems are compared to HFNC. 2 However, the control of propagation factors might improve oxygenation and decrease mortality in patients who use non-invasive equipment. 3
Studies have shown a positive response to HFNC and prone ventilation in alert patients. 4 However, during the collapse of the healthcare system and lack of resource capacity, the expiratory positive pressure (PEP) device with the non-rebreather device could maximize clinical benefit and minimize costs in this clinical setting. 5
Our study aimed to explore the use of threshold PEP with an adult non-rebreather oxygen mask plus prone positioning in conscious patients with HARF due to SARS-CoV-2 infection in the absence of available equipment for HFNC and invasive and non-invasive mechanical ventilator support during the collapse of the health system in a low-income country.
Cases series
This case series included 12 patients who attended the emergency department of Ecuadorian Institute of Social Security (IESS), Babahoyo, Ecuador between 22 March 2020 and 30 March 2020.
Patients admitted to the emergency department who were aged 18–80 years and had a confirmed diagnosis of real-time polymerase chain reaction test SARS-CoV-2 pneumonia and required supplemental oxygen, some other form of oxygen support, non-invasive mechanical ventilation, or HFNC.
Patients with a relationship partial arterial oxygen pressure and inspired fraction oxygen (PaO2/FiO2) ratio <200 mmHg and respiratory rate (RR) > 20 breaths/min with the use of accessory respiratory muscles in the absence of immediate criteria for endotracheal intubation were included.
The device consists of a facial mask attached to the PEP adaptive threshold device (Threshold PEP™) (PHILIS), an oxygen reservoir mask, and a connecting hose for oxygen (Figure 1).
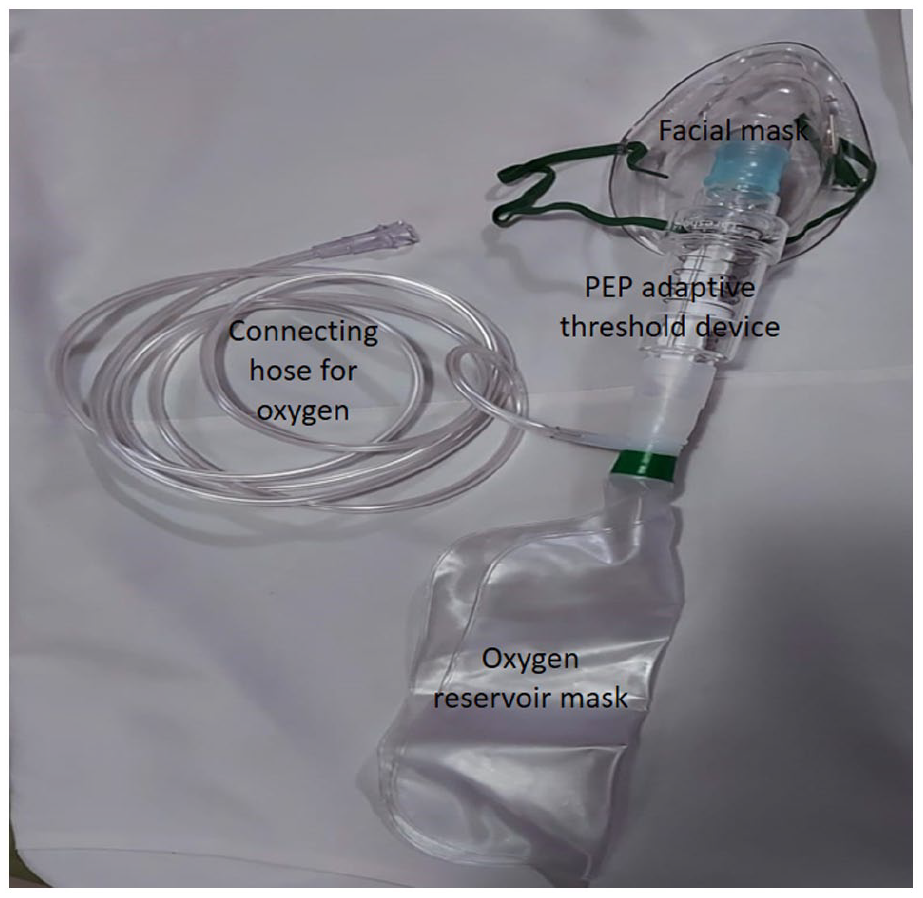
The device consists of a facial mask attached to the PEP adaptive threshold device plus an oxygen reservoir mask and a connecting hose for oxygen. PEP: expiratory positive pressure.
Patients were placed in the prone position, alternated every 2 h between the prone and supine positions during the day, and remained in the prone position at night, as tolerated. A physician supervised the position changes. Patients were instructed to be self-prone, and the nursing staff reminded patients to do so.
Patient demographics, laboratory findings, clinical findings, and medications utilized are reported in the Supplemental Materials.
Measurements and outcomes
Arterial blood gas (ABG) pH, partial pressure of carbon dioxide (pCO2) (mmHg), partial pressure of arterial oxygen (PO2) (mmHg), EB (excess base), HCO3 (mmol/L), alveolar-arterial gradient (mmHg), PaO2/FiO2 (mmHg), FiO2 (%), SaO2 (%), and RR were reported.
SaO2 (%) and RR before and after placement of the device were measured immediately before and 1 h after placement as a primary outcome.
The need for intubation (%), mortality (%), number of days of device use, and number of days of hospital stay were also recorded. All patients were followed for 28 days after hospital discharge.
Ethics approval
Written Informed Consent was obtained from Subjects and their Legally Authorized Representative (in case of deceased) for the publication of the case series
IESS, Babahoyo, Ecuador did not require ethical approval for reporting individual cases or case series because this study was designed as to understand and evaluate the use of a regulatory-approved medical device in a novel clinical setting as judged by established/accepted standards
The use of a non-rebreathing oxygen mask connected to a commercially available valve that exerts positive pressure while the patient expires and while in the prone position could be useful for the management of acute hypoxemic respiratory failure due to SARS-CoV-2 pneumonia, especially when mechanical ventilators and HFNC are not available during the collapse of the health system in a low-income country
A total of 12 cases were managed with this device for a week. Of these patients, 66.7% (eight patients) survived, while 33.3% (four patients) died, number of days of use of the device were median (interquartile range [IQR]) 5 (1–10), and number of days of hospital stay were median (IQR) 10 (3–23). The age at presentation was median (IQR) 58 (31–81) years.
Baseline characteristics of the ABG are presented in Table 1.
The baseline characteristics of the arterial blood gases (ABG) are described.

IQR: interquartile range; HCO3: sets the concentration of buffer or blood bicarbonate; pH: the negative algorithm of the hydrogen ion concentration; PO: partial pressure of oxygen; PCO2: partial pressure of carbon dioxide; SaO2: arterial oxygen saturation; EB: excess base.
SaO2 (%) prior placement median (IQR) 85.5% (80%–89%) and SaO2 (%) post placement of the device was median (IQR) (93%–96%) (P = 0.0001). RR before placement was median (IQR) 38 (36–42) and post placement of the device was median (IQR) 24 (22–30) (P = 0.0005; Wilcoxon test paired samples) 6 (Figure 2).

Graphic representation in Box and Whisker SaO2 (%) prior placement and SaO2 (%) post placement of the device (P = 0.0001).
Discussion
In our study, we found that the use of a PEP adaptive threshold device adult oxygen mask with a reservoir, accompanied by prone positioning, improved oxygenation and RR in patients with acute hypoxemic respiratory failure due to SARS-CoV-2 infection with a success rate of 66.7%.
This PEP device with a non-rebreather was used as a measure to maximize and improve oxygenation during the collapse of the sanitary system when there was a shortage of high-flow machines and mechanical ventilators while minimizing the costs in a resource-stretched situation.
Some case reports and case series have shown improvement in oxygenation and respiratory rate in patients placed in prone position, including patients undergoing or not undergoing non-invasive mechanical ventilation. 7 We used this device in patients with marked hypoxemia. Four of the 12 patients failed to improve with the use of the device and required further ventilatory support. The prone position preserves the redistribution of pulmonary blood flow and reduces atelectasis, and it has shown positive results in patients with marked hypoxemia. 8 We found that ground-glass pulmonary opacities were present in all our patients, followed by frequency by condensation areas and crazy paving patterns. The use of this device with a programmed positive end-expiratory pressure (PEEP) valve between 8 and 10 cm H2O plus prone positioning improves oxygenation and lung compliance because it promotes a decrease in the weight of the lung bases after the occurrence of acute pulmonary edema. These results did not differ from those found in patients with prone ventilation strategies, higher flow rates, and NIMV. Our patients had high biomarker values, especially D-dimer, ferritin, lactate dehydrogenase, and lymphopenia, which are factors associated with increased respiratory failure and death. 9
In addition, studies have shown that the lungs of patients with SARS-CoV-2 infection show fibrinous exudation and proliferation of alveolar epithelial cells type II and macrophages. Alveolar septal vascular congestion, edema, vascular thrombi with focal intraparenchymal hemorrhage, and hemorrhagic infarction are also common, suggesting an important role of the vascular compartment and pulmonary perfusion in the pathophysiology of SARS-CoV-2. 10
Four of our patients were intubated and mechanically ventilated, and they died; however, our results showed a significant improvement in the primary results of SaO2 and RR, with a survival percentage of 66.7.
Similar to our case series, the meta-analysis reported that mortality was variable and declined over time in critically ill patients (45.73%). 11 On the other hand, the Centers for Disease Control and Prevention of the United States revealed 65.2% mortality among hospitalized patients as of 14 April 2021. 12
The device used during the study consisted of a mask connected to the PEP and an additional reservoir bag through which the inhaled oxygen flowed connected through these devices. This requires a minimum oxygen flow of 10–15 L/min. This device can increase the supply of oxygen in addition to providing PEEP, which is important for reducing ventilatory work and hypoxemia in pneumonia due to SARS-CoV-2 infection, mainly in settings where there are limited resources for HFNC or NIMV systems. HFNC, 13 which requires a permanent source of power, either to be supplied through a mechanical ventilator or with independent high-flow oxygen systems, 14 could also be of restricted use in limited-resource settings. In addition, patients can alternate between prone and supine positions, which could result in a significant improvement in oxygenation.
Other methods can generate PEEP either through NIMV 15 using a full-face mask or a specific continuous positive airway pressure hood or helmet.
The study limitations include the lack of a control group and the small sample size, FiO2 measurement could be inaccurate. However, the reported results could be useful in situations of limited resources due to the pandemic.
Conclusion
The use of a PEP adaptive threshold device and adult oxygen mask with reservoir plus prone positioning implementation improved patient oxygenation and decreased RR and effort. This method could be useful for the treatment of hypoxemic respiratory failure due to SARS-CoV-2 infection, especially in settings where limited mechanical ventilators and HFNCs are available.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X231154064 – Supplemental material for Use of threshold PEP with an adult non-rebreather oxygen mask plus prone positioning in acute hypoxemic respiratory failure due to SARS-CoV-2 infection during the collapse of the health system in a low-income country
Supplemental material, sj-docx-1-sco-10.1177_2050313X231154064 for Use of threshold PEP with an adult non-rebreather oxygen mask plus prone positioning in acute hypoxemic respiratory failure due to SARS-CoV-2 infection during the collapse of the health system in a low-income country by Killen H Briones-Claudett, Monica H Briones-Claudett, Eduardo A Martinez Armijos, Jorge J Rios-Marcillo, Lourdes A Orozco Holguin, Killen H Briones-Zamora, Diana C Briones-Marquez, Andrea P Icaza-Freire and Michelle Grunauer in SAGE Open Medical Case Reports
Footnotes
Author contributions
K.H.B.C., M.H.B.C., and E.A.M.A. conceived the idea and initiated this protocol. L.A.O.H. and J.J.R.M. contributed to the development of the search strategy for this review protocol. K.H.B.Z. and D.C.B.M. prepared and wrote the manuscript and M.G. participated in critical revision of the manuscript. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ecuadorian Institute of Social Security (IESS), Babahoyo, Ecuador did not require ethical approval for reporting individual cases or case series because this study was designed as to understand and evaluate the use of a regulatory-approved medical device in a novel clinical setting as judged by established/accepted standards. The use of a non-rebreathing oxygen mask connected to a commercially available valve that exerts positive pressure while the patient expires and while in the prone position could be useful for the management of acute hypoxemic respiratory failure due to SARS-CoV-2 pneumonia, especially when mechanical ventilators and HFNC are not available during the collapse of the health system in a low-income country.
Informed consent
Written informed consent was obtained from Subjects and their Legally Authorized Representative (in case of deceased) for the publication of the case series.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.