
Abstract
To date, only 34 cases of primary pulmonary rhabdomyosarcoma (PPRMS) in the middle-aged and elderly population have been published. However, analyses of the clinicopathological characteristics and prognosis of PPRMS in this population have not been performed. A 75-year-old man visited our hospital because of abdominal pain and discomfort. His serum lactate dehydrogenase, neuron specific enolase, and progastrin-releasing peptide levels were elevated. Positron emission tomography–computed tomography revealed a lobulated mass of 7.6 × 5.5 cm2 in the lower lobe of the left lung with abnormally high fluoro-2-deoxy-
Keywords
Introduction
Rhabdomyosarcoma (RMS) is a malignant primitive mesenchymal tumor with skeletal muscle differentiation, and it is the most common sarcoma in children, accounting for >50% of soft tissue sarcomas in children versus <5% of sarcomas in adults.1–3 RMS usually develops in the head and neck (35%), urogenital system (21%), extremities (19%), and chest (7%). 4 The clinicopathological features and prognosis of 76 cases of RMS in middle-aged and elderly individuals aged ≥40 years were previously analyzed. Only two cases occurred in the lungs; 5 hence, primary pulmonary RMS (PPRMS) is rare in the middle-aged and elderly population, which has been defined as age ≥45 years in the latest categorization of the World Health Organization. At present, studies on the clinicopathological features and prognosis of PPRMS in the middle-aged and elderly population have not been reported.
This study first reported a case of pulmonary acinar RMS in an elderly man, retrospectively reviewed 34 cases of PPRMS in the middle-aged and elderly population reported in PubMed, and finally analyzed the clinicopathological characteristics and prognosis of 35 cases of PPRMS, including this present case, to obtain a general understanding of this malignancy in the middle-aged and elderly population for clinicians and pathologists.
Case presentation
Chief complaints
A 75-year-old man visited our hospital because of obstruction of the left lung.
History of present illness
The patient visited a local hospital for treatment for abdominal pain a week prior to visiting our institution. Chest and abdominal computed tomography (CT) in the local hospital revealed obstruction of the left lung. Thus, he visited our hospital for further treatment. The patient had no nausea, vomiting, diarrhea, or hemoptysis, and he had normal defecation.
History of past illness
The patient denied any infectious disease, chronic illness, allergy, or operative history.
Personal and family history
The patient lived in Haimen, Nantong city, Jiangsu Province, China for a long time, and he had no travel, smoking, drinking, or family history.
Physical examination
The patient’s consciousness was clear, and his temperature, heart rate, and blood pressure were normal. No abnormality was found in the general physical and special examinations.
Laboratory examinations
There were no significant abnormalities regarding blood routine and biochemical indices, excluding an increase in his lactate dehydrogenase (LDH) level to 442 U/L (normal, 106–211 U/L). The levels of serum tumor markers, including carcinoembryonic antigen, cytokeratin 19 (CK19) fragment, and squamous cell carcinoma antigen, were normal, whereas neuron-specific enolase (NSE) and progastrin-releasing peptide (pro-GRP) levels were increased to 63.07 ng/mL (normal, 0–17 ng/mL) and 84.68 pg/mL (normal, 25.3–69.2 pg/mL), respectively.
Imaging examinations
Positron emission tomography (PET)–CT revealed a lobulated mass of 7.6 × 5.5 cm2 in the lower lobe of the left lung with abnormally high fluoro-2-deoxy-
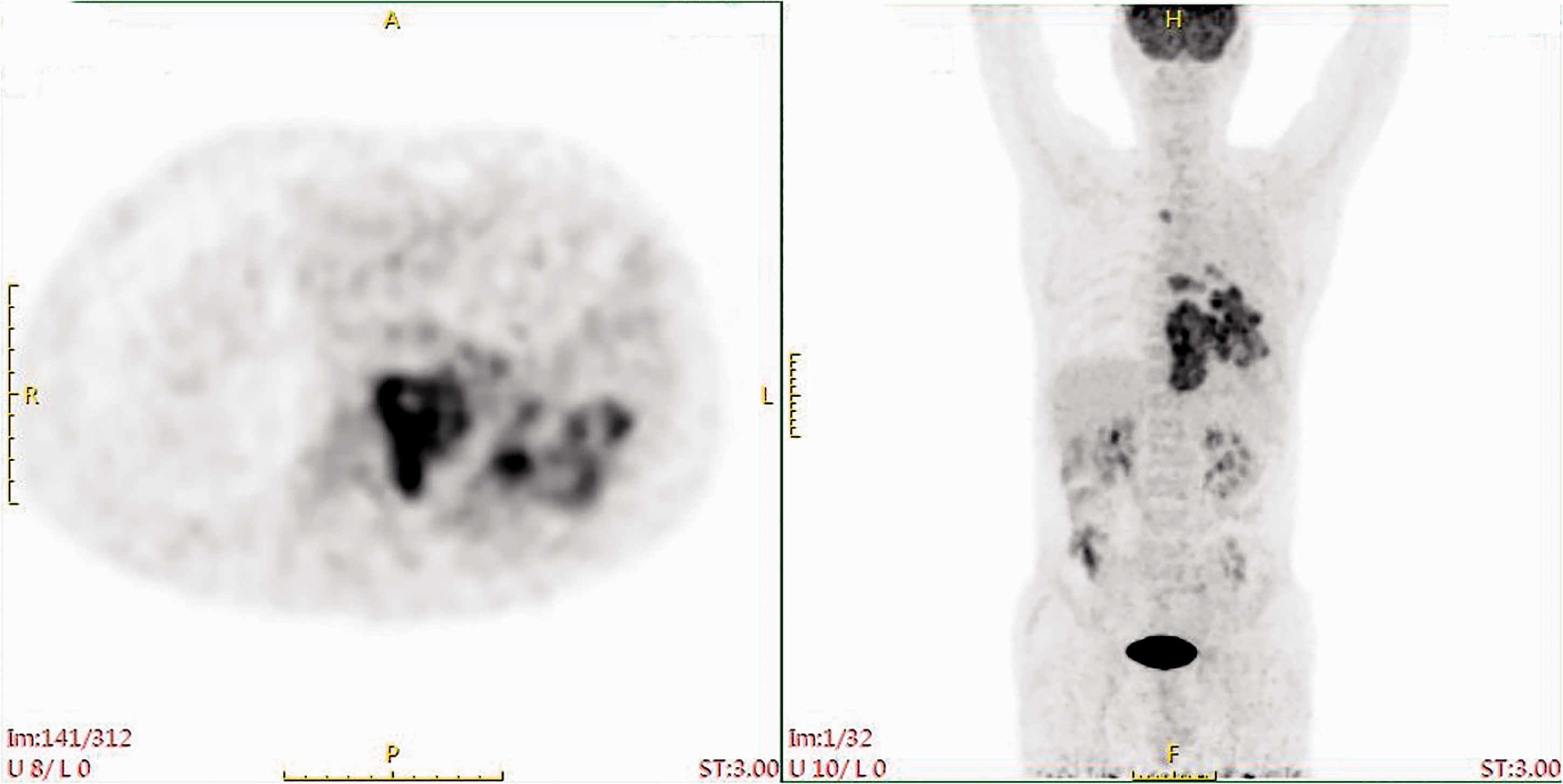
Transversal (left) and axial (right) section of positron emission tomography–computed tomography revealing a mass in the left lung with abnormally high fluoro-2-deoxy-
Further diagnostic workup
Histologically, biopsy of the left lung revealed that the tumor cells were small with little cytoplasm, deeply stained nuclei, and heavily stained nuclear chromatin, which is extremely similar to the morphology of small cell lung carcinoma (SCLC, Figure 2a). Immunohistochemically, the tumor cells were positive for desmin, MyoD1, myogenin, synaptophysin (Syn), CD56 (Figure 2b–f), and SMARCA4, and the Ki67 index was 90%. Negative staining was noted for epithelial markers CK (AE1/AE3), CK18, EpCAM, CK (CAM 5.2), CK7, CK8, and CK14, and other markers, such as TTF-1, chromogranin A (CgA), FLI-1, CD99, CD20, CD3, Pax5, HMB45, S-100, NUT, SALL4, SOX2, and CD34. Cytogenetic analysis for FOXO1A translocation was negative.

Histopathological morphology and immunohistochemical markers of rhabdomyosarcoma. (a) Rhabdomyosarcoma featuring small tumor cells with little cytoplasm and extrusion deformation caused by mechanical damage resembling small cell lung cancer (hematoxylin and eosin staining, magnification ×400). Tumor cells with strong nuclear staining for (b) MyoD1 (magnification ×400) and (c) myogenin (magnification ×400) and cytoplasmic reactivity for (d) desmin (magnification×400), (e) synaptophysin (magnification ×400), and (f) CD56 (magnification ×400).
Final diagnosis
The diagnosis of PPRMS was confirmed by Prof. Wang Jian from the Pathology Department of Fudan University Shanghai Cancer Center (Shanghai, China).
Treatment
RMS is usually treated by surgery, chemotherapy, and/or radiotherapy. 5 The treatment protocol was approved by the patient. Because of general weakness, he could not tolerate tumor resection, and he was administered combined chemotherapy with vincristine 1 mg, actinomycin 0.4 mg, and cyclophosphamide 0.8 mg.
Outcome and follow-up
The patient only received one course of chemotherapy, and he died 2 months after the diagnosis. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Discussion
Because of the rarity of PPRMS in the middle-aged and elderly population, information regarding its clinicopathological characteristics and prognosis is extremely limited. Large multi-institutional trials have not been performed, and only reports from single institutions have been published. More importantly, analyses on the clinicopathological characteristics and prognosis of PPRMS in the middle-aged and elderly population have not been conducted.
RMS develops in the lungs, and there is no specificity regarding its clinical manifestation and serum laboratory data. In our case, LDH, NSE, and pro-GRP levels in the blood were simultaneously elevated, but these three markers are useful in the diagnosis and prognosis of SCLC.6–8 Under microscopy, the tumor cells were small and deeply stained with extrusion deformation, which should be distinguished from some small round cell tumors in the lungs. (1) First, the serological data, microscopic morphology, and immunohistochemical results of neuroendocrine markers easily results in a misdiagnosis of SCLC because it is more common than RMS in the lungs. Moreover, the immunohistochemical results of RMS partially overlap with those of SCLC, as 43% of acinar PPRMS lesions express at least one specific neuroendocrine marker, 32% express Syn, 22% express CgA, and 11% express both Syn and CgA, whereas CD56 is expressed in almost all cases. 9 However, epithelial markers are usually positive, and TTF-1 is positively expressed up to 80% to 90% of cases of SCLC. 10 (2) Morphologically, monomorphous small- or medium-sized cells with scant cytoplasm might not be completely distinguished from nuclear protein in testis (NUT) carcinoma, which is an aggressive malignancy that often arises in the mediastinum and upper aerodigestive tract in patients of any age with variable symptoms at presentation depending on the anatomic location. However, NUT carcinoma often has foci of abrupt squamous differentiation with keratinization scattered among the more primitive-appearing cell nests. Immunohistochemically, the tumor cells are commonly positive for NUT, CK5/6, P63, P40, and other markers including CD99, Fli-1, Syn, EGFR, and HER2. 11 Our immunohistochemical results precluded a diagnosis of NUT carcinoma. (3) Thoracic SMARCA4-deficient undifferentiated tumors are also aggressive malignancies diagnosed more often in young male smokers with undifferentiated morphology and occasional hepatoid and rhabdoid features. Immunohistochemically, the tumor cells are often negative for SMARCA4 with the concurrent loss expression of SMARCA2 and positive for one or more stem cell markers (SOX2, CD34, and SALL4). 11 Our immunohistochemical results also precluded a diagnosis of this tumor. (4) Pleuropulmonary blastoma (PPB) might not be distinguishable from RMS, but the former is rare, typically occurring in children younger than 6 years. PPB is divided into subtypes I, Ir, II, and III. Type I tumors are purely cystic lesions, type II tumors have cystic and solid components, and type III tumors are purely solid lesions. PPB is associated with a germline mutation in DICER1. Histologically, PPB exhibits two components: small round uniform hyperchromatic blue cells and occasional large cells with a central nucleus and moderate cytoplasm. Immunohistochemically, the hyperchromatic blue cells are positive for vimentin, and occasional large cells exhibit immunoreactivity for pan-CK. Our immunohistochemical results also precluded a diagnosis of this malignancy.12,13 (5) Some other rare tumors, such as soft tissue clear cell sarcoma, extraosseous Ewing sarcoma, non-Hodgkin lymphoma, and malignant melanoma, resemble acinar RMS, but immunohistochemical markers of these tumors, such as HMB45, S-100, CD99, Fli-1, CD20, CD3, and Pax5, were all negative. (6) PET-CT revealed no other lesions in the whole body, dismissing the possibility of secondary tumors.
To better characterize the clinical features and outcomes of PPRMS in the middle-aged and elderly population, we searched all reports of PPRMS in this population from 1958 to 2021 available on PubMed and Elsevier websites and removed the repeated cases in this literature. We analyzed 35 cases of PPRMS, including 34 cases from PubMed14–21 and the current case (Table 1). These cases involved significantly more men than women (P = 0.001). The proportion of patients aged 50 to 69 years was higher than those of patients aged 45 to 49 years and ≥70 years (P < 0.001). The pleomorphic type was more common than the embryonal and acinar types (P < 0.001, Table 2). Thirty-three patients received different treatments. Among the 29 patients who received follow-up, the treatment received was significantly correlated with the prognosis. The survival time of patients who received supportive treatment was short, and that of patients who underwent surgical resection was significantly prolonged (P = 0.010, Figure 3).
Cases of primary pulmonary rhabdomyosarcoma in middle-aged and elderly patients (review of the literature).

M, male; F, female; NS, not specified; DOD, died of disease; DUD, died of unrelated disease; AWD, alive with disease; NED, no evidence of disease; SUP, supportive; S, surgery; RT, radiotherapy; CT, chemotherapy.
Clinicopathological features and significance of primary pulmonary rhabdomyosarcoma in middle-aged and elderly patients.

M, male; F, female; NS, not specified.

Survival of 29 middle-aged and elderly patients with primary pulmonary rhabdomyosarcoma diagnosed from 1958 to 2021 who were treated using different methods.
We found a significant sex difference and notable age distribution in PPRMS in the middle-aged and elderly population, as most patients were male and aged 50 to 69 years. Because of the rarity of PPRMS and low number of reports in the middle-aged and elderly population, there is no similar finding at present. A previous study recorded a male/female ratio of 1.5:1 among 76 patients with RMS aged ≥40 years. 5 A recent study also described 66 patients with embryonal and alveolar RMS, including 42 men and 24 women. 22 A large study analyzed data on RMS in 1071 adults (age >19 years) and 1529 children (age ≤19 years), and a male predominance was observed for both adults and children. 3 Some researchers found a male predominance (male/female ratio of 1.5:1) in almost all types of soft tissue sarcomas, and the age ranges were 20 to 76, 25 to 71, 18 to 86, and 55 to 76 years for head and neck, genitourinary, limbs, and other primary locations, respectively.23,24
There was a significant difference in the histological type of PPRMS in the middle-aged and elderly population, and most patients were diagnosed with the pleomorphic type. A large study demonstrated that the embryonal and alveolar subtypes were the first and second most common subtypes in children/adolescents, respectively, whereas embryonal and pleomorphic subtypes other than not otherwise specified were the two most common subtypes in adults. 3 A previous study on 76 cases of RMS in the middle-aged and elderly population also proposed that the embryonal and pleomorphic subtypes were most common. 5 Another study found that the incidence of pleomorphic RMS was higher than that in alveolar and embryonal RMS, and the median age (51 years) was higher for pleomorphic RMS than for the other types. 24 Pleomorphic RMS is an aggressive sarcoma, arising predominantly in the extremities of adult men aged ≥45 years. 25 Similar to the aforementioned findings, PPRMS in the middle-aged and elderly population is more common in men, and it usually has a pleomorphic subtype.
The combination of surgery, chemotherapy, and/or radiotherapy has achieved good results in children with RMS, and the prognosis of RMS in children has significantly improved. The successful experience in the treatment of RMS in children has been widely applied in the treatment of adult RMS (including middle-aged and elderly individuals), but the effect has been unsatisfactory. 5 Pleomorphic RMS is less sensitive to chemotherapy, and its treatment depends more on surgery. The unfavorable prognostic factors of RMS are the anatomical location (e.g., parameninges, extremities, abdomen, chest) histological subtypes (including acinar and pleomorphic RMS), tumor size >5 cm, and metastasis. 26 In this study, although some patients undergo surgery and/or chemotherapy, 24 of 35 patients were diagnosed with the pleomorphic or acinar type, and each lesion was located in the lungs. The prognosis of PPRMS in the middle-aged and elderly population is poor.
Limitations
Our analyses had multiple limitations. First, because most cases in the literature spanned a long period, progress in supplementary examination has shifted the diagnosis of RMS from standard morphological detection to the incorporation of immunohistochemical staining and molecular testing. It is possible that some cases included in our analyses were not RMS, particularly those with the pleomorphic type. Second, some cases lacked details regarding clinicopathological features and prognosis. Consequently, some clinicopathological features, such as tumor size, could not be statistically analyzed.
Conclusion
We reported a case of PPRMS and retrospectively reviewed and analyzed the clinicopathological features of PPRMS in the middle-aged and elderly population to help clinicians and pathologists better understand this rare tumor of the lungs in this population.
Footnotes
Authors’ contributions
The clinical data of the patient was collected by Zheng Guihua. Histopathology was performed by Chen Xudong. Wang Jiatai and Zhu Xinghua performed immunohistochemical and molecular pathological analyses. The manuscript was drafted by Wei Yingze and Jin Xiaoxia with contributions from all coauthors. The final manuscript was read and approved by all authors.
Availability of data and materials
The data and materials of this work are available on request by the corresponding authors.
Declaration of competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The reporting of this study conforms to the CARE guidelines. 27 This study was performed in line with regulations issued by the National Health Commission of China and was approved by the local Commission of Ethics (reference number 2021-A 10). Written informed consent was obtained from the participant included in the study.
Funding
There was no funding for this article.