
Abstract
Intracranial dissemination is rare among patients with glioblastoma multiforme (GBM). Very few GBM patients develop symptoms from intracranial dissemination, as most do not surviving long enough for intracranial dissemination to become clinically evident. Herein, we report a case of GBM in a 39-year-old woman who underwent surgical resection, concomitant chemoradiotherapy, and seven courses of adjuvant chemotherapy with temozolomide. The patient then complained of an instable gait and hearing loss. Imaging studies demonstrated that although the primary intracranial tumors were well-controlled by treatment, contralateral cerebellopontine angle seeding dissemination was present. The patient died 3 months after the diagnosis of seeding dissemination. In light of a previous report and our current case, heightened awareness could promote surgical strategies that minimize the possibility of dissemination, including avoiding ventricular entry or a no-touch strategy.
Introduction
Glioblastoma multiforme (GBM) is the most aggressive primary brain tumor in adults, accounting for 12% to 15% of all intracranial tumors. 1 The prognosis of GBM patients remains poor even with improvements in surgery, chemotherapy, and radiotherapy. During the last few years there have been an increasing number of reports about GBM dissemination, which is attributed to the prolonged survival of GBM patients after tumor excision.2,3 However, the incidence of GBM dissemination is lower than what is observed in autopsy studies. 4 Many studies have shown that GBM dissemination induces fatal outcomes. The median survival time of GBM patients ranges from 11 to 17 months; however, the average time between a diagnosis of GBM seeding dissemination and death is only 2 to 3 months. 5
Case report
A 39-year-old female patient with an unremarkable past medical history presented with headache and unilateral limb weakness and was admitted to our hospital. Neurological examination showed no positive signs. A head magnetic resonance imaging (MRI) scan revealed a long-T1 and long-T2 cystic and solid mass measuring 4.9 × 4.7 × 3.6 cm with obvious peritumoral edema in the right frontotemporal lobe, which compressed the lateral ventricles. After gadolinium injection, the mass was heterogeneously enhanced (Figure 1a, b and c). Then the patient underwent a gross total resection of the right frontotemporal tumor. The methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) promoter in the GBM sample was analyzed using methylation-specific PCR, and the MGMT promoter was found to be unmethylated.

Gadolinium-enhanced T1-weighted magnetic resonance imaging showing the intracranial tumors in the right frontal and insula prior to surgery (a: coronal image, b: sagittal image, c: axial image). Gadolinium-enhanced T1-weighted magnetic resonance imaging 7 months after surgery showing the tumor had been completely removed (d: coronal image, e: sagittal image, f: axial image).
Pathological examination of the tumor identified it as GBM. Immunohistochemistry (IHC) of the tumor demonstrated negative staining for glial fibrillary acidic protein (GFAP). The Ki-67 labeling index was 60% (Figure 2a, b, c and d). Three weeks after uneventful postoperative recovery, the patient started to receive concomitant chemoradiotherapy with temozolomide (TMZ; 75 mg/m2/day) and external beam X-ray irradiation therapy (60 Gy in 30 fractions), which was tolerated well. Adjuvant chemotherapy with TMZ (200 mg/m2/day) for 5 days every 4 weeks was subsequently administered. The patient's initial symptoms were resolved, and head MRI 7 months after primary tumor resection showed no recurrence (Figure 1 d, f and g).

(a) Hematoxylin and eosin staining of pathological sections after the first operation. (b) Immunohistochemistry showing the tumor was negative for GFAP; (c) the tumor was positive for OLIG2; (d) the Ki-67 labeling index was 60%.
It should be noted that after the seventh cycle of adjuvant chemotherapy, the patient complained of an instable gait and hearing loss. Gadolinium-enhanced head MRI revealed a new heterogeneously-enhanced solid mass in the left cerebellopontine angle region but no recurrence of the initial tumor in the right frontotemporal lobe and no spinal dissemination (Figure 3e, f and g). The patient underwent secondary resection of the tumor, and histology confirmed GBM dissemination. IHC of the new mass demonstrated positive staining for GFAP and OLIG2 and a Ki-67 labeling index of 30% (Figure 3a, b, c, and d). Her family refused further treatment, and the patients died 3 months after the second surgery, 12 months after the initial diagnosis. We have also included a table summarizing previously published articles of related cases (Table 1). The reporting of this study conforms to CARE guidelines. 6

(a) Hematoxylin and eosin staining of pathological sections after the second operation. (b) Immunohistochemistry showing the tumor was positive for GFAP; (c) the tumor was positive for OLIG2; (d) the Ki-67 labeling index was 30%. Magnetic resonance imaging performed after the 7th chemotherapy cycle revealed the presence of a mass in the left cerebellum. The mass appeared hyperintense on enhanced magnetic resonance imaging performed, with obvious heterogeneous enhancement (e: coronal image, f: sagittal image, g: axial image).
Summary of previous cases reporting patients with GBM metastases.
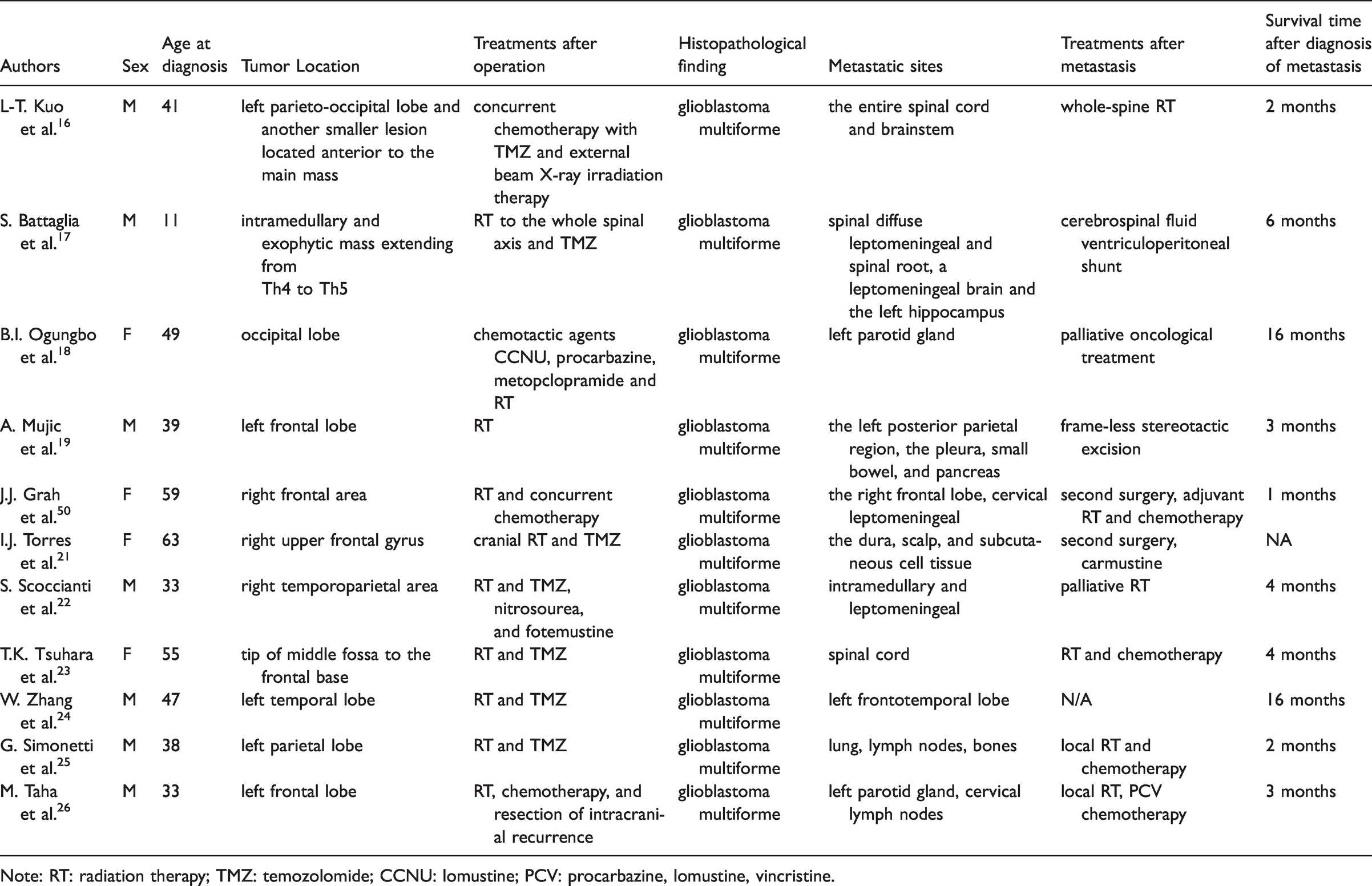
Note: RT: radiation therapy; TMZ: temozolomide; CCNU: lomustine; PCV: procarbazine, lomustine, vincristine.
Discussion
GBM is the most common malignant primary brain tumor, accounting for 12% to 15% of intracranial neoplasms. 7 GBM has a reported global incidence of 2 to 3 per 100,000 people. 1 Despite advancements in diagnostic and therapeutic approaches, GBM continues to have a poor prognosis with patient survival at approximately 15 months after diagnosis. 8 Previous studies indicated that GBM dissemination does not occur, primarily due to the strong protective mechanisms in the central nervous system, such as the lack of a true lymphatic system in the brain and because the venous sinuses are encased in dense dural membranes, both of which hinder invasion.9–11 GBM patients have a short survival time and commonly die from oncothlipsis, intracranial hypertension, and other complications before metastasis develops. 12
Advancements in early detection and therapeutic approaches have resulted in an increased median survival for GBM patients, which has consequently increased the detection of GBM dissemination. 12 Autopsy studies have also described that approximately 25% of GBM patients have evidence of spinal subarachnoid seeding, suggesting GBM dissemination is not uncommon.1,13,14 With the prolonged survival of GBM patients, it is important to study the GBM dissemination.
The most common metastasis sites for GBM are the spinal cord, lungs, bone, and lymph nodes. 3 To date, the factors that cause GBM metastasis remain unclear. Cellular spread in the subarachnoid space seems to be the most likely cause for intracranial and spinal dissemination. According to the literature, ventricular entry at operation, repeated tumor resection, male sex, ependymal invasion, fissuring of the ependymal due to hydrocephalus, depressed immune function after radiotherapy and chemotherapy, and fragmentation of the tumor in contact with cerebrospinal fluid were all associated with a statistically significant increased incidence of central nervous system dissemination. 3
In this case, the primary tumor was located at the lateral fissure, making cellular spread in the subarachnoid space the most likely cause. Heightened awareness can promote surgical strategies that minimize the possibility of dissemination, including avoiding ventricular entry or a no-touch strategy.
The prognosis of GBM patients with dissemination is bleak and almost always leads to fatal outcomes. The median time between a diagnosis of GBM dissemination and death is approximately 2 to 3 months, 15 and treatment is primarily palliative.
Conclusion
GBM dissemination is common to some extent. Heightened awareness will promote surgical strategies that reduce the possibility of dissemination, including avoiding ventricular entry and a no-touch strategy.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Written informed consent was obtained from the parents for the publication of this case report. The study protocol was approved by Shandong Provincial Hospital affiliated to Shandong First Medical University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Natural Science Foundation of Shandong Province (grant number: ZR2021MH228).