
Abstract
Objective
This article aimed to study the clinicopathological features, immunophenotypes, and differential diagnoses of plexiform fibromyxoma (PF).
Methods
We searched clinical and pathology databases of our hospital for patients with histologically confirmed PF from 2007 to 2020 and reviewed the relevant English and Chinese language literature.
Results
Two cases of PF were identified, a 67-year-old woman and a 23-year-old man. Both patients presented with melena and anemia and underwent partial gastrectomy. Histologically, the tumors exhibited a plexiform growth pattern in the gastric submucosa and the presence of bland-looking spindle cells in the fibromyxoid stroma with the formation of small blood vessels. Immunohistochemically, the two cases were strongly positive for vimentin, smooth muscle actin, and muscle-specific actin and negative for CD117, discovered on gastrointestinal stromal tumors protein 1, CD34, CD10, S100, desmin, H-caldesmon, estrogen receptor, progesterone receptor, β-catenin, and cytokeratin.
Conclusions
PF is a rare mesenchymal tumor of the stomach that can be distinguished from other gastrointestinal mesenchymal tumors based on its distinctive morphology and immunophenotype.
Keywords
Introduction
Gastrointestinal stromal tumors (GIST) are the most common gastrointestinal mesenchymal tumor. In 2007, Takahashi et al. 1 reported a rare gastric tumor with a distinctive morphology for the first time that was named a plexiform angiomyxoid myofibroblastic tumor (PAMT). The term PAMT is more of a histological description of the tumor, emphasizing the myofibroblastic differentiation noted in most cases. In 2009, Miettinen et al. 2 described another 12 cases of similar tumors, classifying them as plexiform fibromyxoma (PF), which was added to the 2010 World Health Organization Classification of Tumors of the Digestive System. PF is a broader term that incorporates all histological and immunohistochemical variants previously described. This rare mesenchymal tumor occurs primarily in the stomach and exhibits a benign clinical prognosis.1–12
Histologically, the tumor is characterized by a plexiform growth pattern, the proliferation of cytologically bland spindle cells, and a myxoid stroma rich in small blood vessels. 5 Substantial cytological atypia is absent, and the mitotic rate is low. Spindle cells are positive for vimentin, and most reported cases express muscle-specific actin (MSA) and smooth muscle actin (SMA). The tumor exhibits variable expression of CD10, progesterone receptor (PR), desmin, H-caldesmon, and calponin and is negative for CD34, CD117, discovered on gastrointestinal stromal tumors protein 1 (DOG-1), estrogen receptor (ER), and S-100 protein. Molecular studies show the absence of c-KIT or platelet-derived growth factor receptor (PDGFR)-a mutations. 2
To date, no patients with PF have reportedly developed recurrence or metastasis. PF is a distinctive mesenchymal neoplasm with a benign clinical course that should be distinguished from other gastrointestinal mesenchymal tumors, such as GIST, leiomyoma, schwannoma, and fibromyxoid neoplasms. Here, we describe two rare cases of gastric PF and review the current literature, providing valuable information to help avoid potential diagnostic pitfalls.
Materials and methods
Study subjects
This study was approved by the Institutional Review Board of Shanghai General Hospital. Patient consent was obtained by telephone, and the patients’ identities were protected. Both a clinical database and pathology archives were searched over a 13-year period (2007–2020) for patients with a histologically confirmed diagnosis of PF or PAMT who received treatment at our institution. The following parameters were recorded: patient age, sex, clinical presentation, tumor site and size, treatment, and follow-up data. All available hematoxylin and eosin-stained sections were reassessed by two senior pathologists.
Immunohistochemical analysis
Immunohistochemical studies were performed on 4-µm-thick unstained sections generated from formalin-fixed, paraffin-embedded tissues using antibodies against vimentin (V9, dilution 1:200), cytokeratin (AE1/AE3, dilution 1:50), SMA (1A4, dilution 1:100), MSA (HHF35, dilution 1:70), CD117 (YR145, dilution 1:70), DOG-1 (SP31, dilution 1:50), CD34 (QDEnd 10, dilution 1:50), S100 (4C4.9, dilution 1:80), CD10 (56C6, dilution 1:40), desmin (D33, dilution 1:70), H-caldesmon (h-CALD, dilution 1:70), ER (SP1, dilution 1:100), PR (SP2, dilution 1:100), β-catenin (E247, dilution 1:40), and Ki-67 (MIB-1, dilution 1:100) purchased from GeneTech (Shanghai, China). Immunohistochemical studies were performed using a Ventana Benchmark XT automatic immunohistochemical apparatus (Roche Ventana Company; Oro Valley, Arizona, USA). The sections were observed with an Olympus BX53 microscope (Olympus; Tokyo, Japan). Appropriate positive control samples were used throughout the study.
Results
Clinical features
The first case is a 67-year-old female patient who presented with abdominal pain and melena for 15 days. Routine blood examination indicated anemia (hemoglobin = 66 g/L). Endoscopic ultrasonography revealed a 3 cm × 2.5 cm submucosal tumor originating from the muscularis propria and showing heterogeneous hypoechoic changes. Additionally, mucosal ulceration was found at the gastric antrum anterior wall, suggesting a GIST (Figure 1a). Computed tomography (CT) revealed an enhancing, highly vascular exophytic submucosal mass in the anterior wall of the gastric antrum, indicating a GIST or neuroendocrine tumor. A wedge resection with a sufficient margin was performed without any other adjuvant therapy. She was alive at the 14-month follow-up with no evidence of recurrence.

Clinical features of a 67-year-old woman with plexiform fibromyxoma (case 1). (a) Gastroendoscopy revealed a submucosal tumor at the antrum. (b) Gross appearance of the tumor showed a submucosal mass protruding from the mucosal surface. (c) The cut section showing a multinodular, solid glistening translucid tumor.
The second case is a 23-year-old male patient who presented with dizziness, melena, and chest pain for 2 months. Routine blood examination indicated anemia (hemoglobin = 42 g/L). Gastroscopy revealed a proliferative mass. Enhanced CT and CT angiography of the abdomen revealed a 5.7-cm × 3.5-cm mass located in the gastric wall of the antrum and the lower part of the gastric body. Partial gastrectomy was performed without any other adjuvant therapy. He was alive at the 74-month follow-up with no evidence of recurrence.
Pathological findings
Gross examination of the specimens showed a relatively well-circumscribed and greyish white tumor (Figure 1b). Analysis of the cut section revealed a multinodular, solid glistening translucid tumor occupying the submucosa and muscularis propria (Figure 1c) and extending out of the serosa (Figure 2). The largest diameter measured 2.7 cm in case 1 and 5.3 cm in case 2. Both lesions showed mucosal ulceration (Figure 3a).

Pathological findings in a 23-year-old man with plexiform fibromyxoma (case 2). The tumor penetrated the serosa (arrow) and formed extraserosal nodules (star) (HE, ×2)

Histological characteristics of the tumor in case 1. (a) Biopsy sample exhibits a submucosal tumor with ulceration (HE, ×20). (b) The tumor shows a multinodular plexiform growth pattern within the muscularis propria (HE, ×40). (c) The tumor contains spindle-shaped bland tumor cells in the fibromyxoid stroma, which is abundant in small dilated and arborizing vessels with various shapes (HE, ×200). (d) Tumors cells contained round or ovoid nuclei and scanty eosinophilic cytoplasm, and some cells exhibited perinuclear cytoplasmic haloes (HE, ×400).
Histologically, the tumors were characterized by a multinodular plexiform growth pattern (Figure 3b) and the presence of spindle cells in the myxoid or fibromyxoid stroma rich in arborizing thin-walled vessels (Figure 3c). The spindle tumor cells contained round or ovoid nuclei and scanty eosinophilic cytoplasm. Some cells exhibited perinuclear cytoplasmic haloes. Lymphocytes and mast cells were observed in the stroma. There was no significant cytological atypia or necrosis in the tumor cells, and mitotic activity was negligible (Figure 3d).
Immunohistochemically, the spindle cells were consistently positive for SMA (Figure 4a), MSA (Figure 4b), and vimentin but negative for CD117 (Figure 4c), DOG-1, CD34, CD10, S100, desmin, H-caldesmon, β-catenin, ER, PR, and cytokeratin. Moreover, the Ki-67 index was particularly low (∼1%) (Figure 4d).
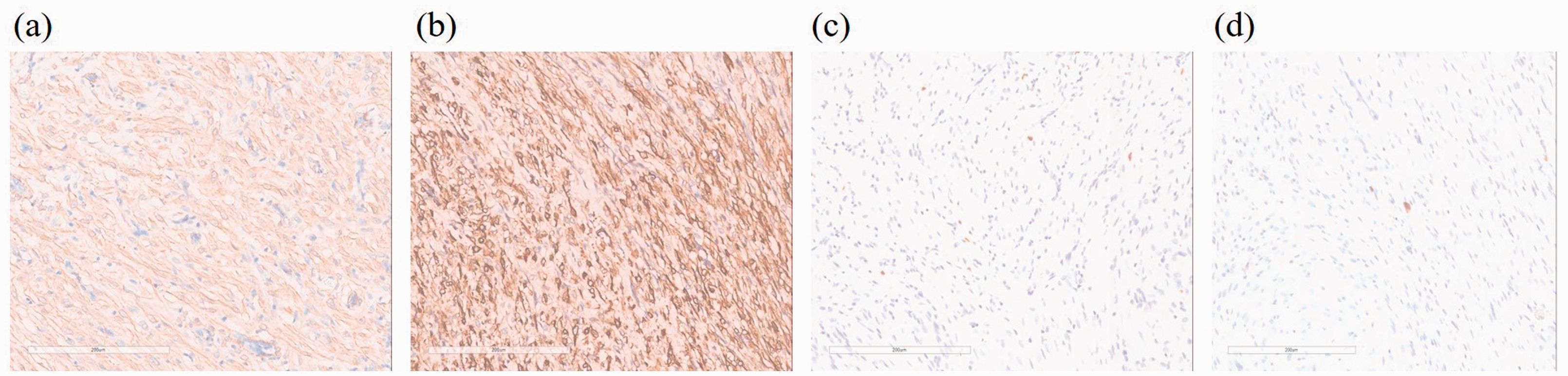
Histological analysis of case 1. (a) SMA is positive in neoplastic cells (×200). (b) MSA is positive in neoplastic cells (×200). (c) CD117 is negative in neoplastic cells (×200). (d) Ki-67 index is approximately 1% (×200).
We also performed a literature review, and the clinicopathological features of PF are summarized in Table 1.
Clinicopathologic features of plexiform fibromyxoma.
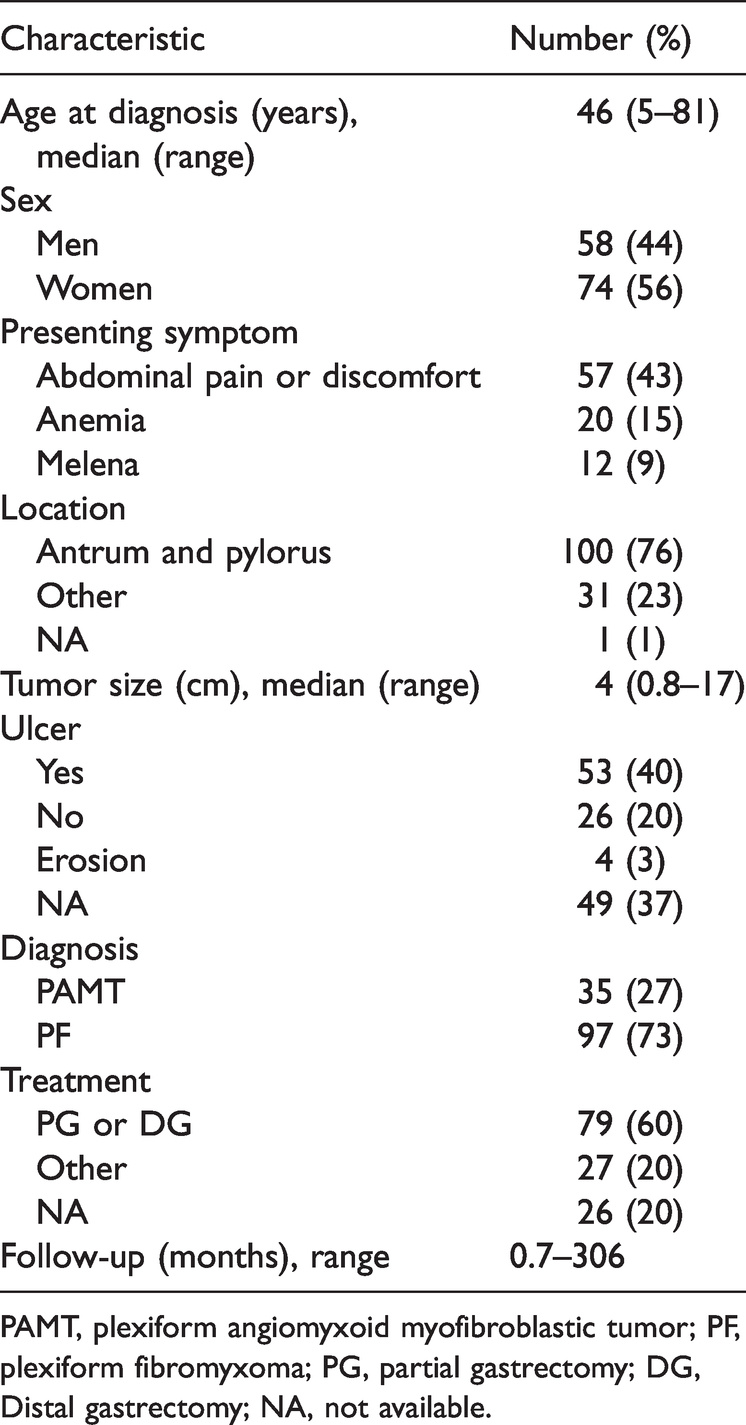
PAMT, plexiform angiomyxoid myofibroblastic tumor; PF, plexiform fibromyxoma; PG, partial gastrectomy; DG, Distal gastrectomy; NA, not available.
Discussion
PF is a rarely reported gastrointestinal mesenchymal neoplasm. To the best of our knowledge, only 130 cases of PF or PAMT have been reported in the Chinese and English literature.
To better understand the clinicopathologic features of PF, we performed a brief review of the literature (Table 1).1–51 Taking the present study into account, the tumor is located mainly in the gastric antrum and pylorus (76%), but other rare locations, such as the gastric fundus, gastric body, duodenum, jejunum, cecum, gallbladder, posterior mediastinum, and esophagus, have also been reported. 2 , 17 , 29 , 47 The overall median and average ages of patients with PF at diagnosis were 46 years and 43.3 years, respectively (range, 5 to 81 years). To date, a slightly higher prevalence of women with PF has been reported, with female patients accounting for 56% and male patients accounting for 44%. The clinical manifestations ranged from asymptomatic to common upper gastrointestinal symptoms and severe gastrointestinal bleeding or perforation. The most common symptoms include abdominal discomfort and pain, anemia, and melena. 5 , 14 , 33 Other clinical presentations include nausea, vomiting, hematemesis, dizziness, and weight loss. The maximum diameters of tumors ranged from 0.8 to 17 cm (median, 4 cm; mean, 5 cm). Including our two cases, 40% of tumors exhibited surface ulceration.
Radiological and endoscopic findings revealed a submucosal tumor-like elevated lesion that was often ulcerated, and endoscopic ultrasonography demonstrated a multinodular mass. 3 CT images showed mild enhancement during the arterial phase and strengthened progressive enhancement during the venous and delayed phases. 10 The tumor exhibited heterogeneous gradual enhancement on contrast-enhanced magnetic resonance imaging. 25 However, endoscopic and radiologic findings are non-specific in the diagnosis, and most cases were misdiagnosed as GIST or other gastric mesenchymal tumors.
The main treatment for PF is surgical resection, including partial gastrectomy and distal gastrectomy. 22 Conservative management includes endoscopic resection and nonsurgical intervention. Ultimately, the surgical technique is dependent on the size and location of the tumor. In all reported cases, follow-up periods ranged from 0.7 to 306 months. No malignant progression, local recurrence, or metastasis was reported. In agreement with previous reports, our two patients were followed up for 14 months in case 1 and 74 months in case 2, and no sign of recurrence was found.
Genetic mutations have also been examined. Spans et al. 9 described some cases of PF that showed metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) and glioma-associated oncogene homolog 1 (GLI1) gene translocation. Including our two patients, no reported PF cases showed C-KIT or PDGFR-a mutations.
Histopathologically, PF most commonly presents as a solitary, lobulated, submucosal, or transmural mass with whitish to brownish/reddish smooth mucosal surfaces or ulceration. 2 , 5 Typically, the tumor is interspersed between the smooth muscles of the stomach wall, with microscopic examination showing the characteristic plexiform or nodular growth pattern. In some cases, the tumor may reside in the mucosa or invade the serous membrane. Compared with eosinophilic smooth muscle, the plexiform structure is lightly stained. It is mainly composed of bland ovoid to spindle cells, abundant small arborizing blood vessels, and a myxoid or fibromyxoid background. 1 , 2 , 5 The tumor cells are relatively uniform in size with round to oval nuclei, mildly eosinophilic or scant cytoplasm, inconspicuous nucleoli, and fine chromatin. In the cases we reviewed, there was no obvious cellular atypia, and mitosis was rare. PF has a characteristic morphology, distinguishing it from other mesenchymal tumors. However, because there is some morphological overlap, adequate immunohistochemical staining should be performed.
Immunohistochemical staining showed diffuse positivity for vimentin, SMA, and MSA in most cases, whereas the tumor cells exhibited variable positivity for desmin, CD10, and H-caldesmon, indicating the fibroblastic, myofibroblastic, and smooth muscle cell natures of PF. Other antibodies, such as CD117, DOG-1, CD34, S100, β-catenin, anaplastic lymphoma kinase (ALK), and cytokeratin, were negative. 2 , 5 , 8 , 10 , 15 , 24 , 45 Here, both cases were negative for desmin, CD10, and H-caldesmon, consistent with most reported cases.
The differential diagnoses for PF include the following: [1] The most important differential diagnosis of PF is GIST. GIST is the most common mesenchymal tumor in the gastrointestinal tract, and many patients with PF are initially misdiagnosed as GIST. 2 , 43 Myxoid GISTs may show plexiform or multinodular growth patterns, including abundant myxoid stroma and spindle cell proliferation, similar to PF. However, the tumor cells are positive for CD117, DOG-1, and CD34, and genetic testing of C-KIT or PDGFR-a mutations can differentiate them from PF. 2 , 10 , 43 [2] In addition, gastrointestinal schwannoma 36 is an uncommon tumor entity and important in the differential diagnosis of mesenchymal tumors in the gastrointestinal tract. Immunohistochemical assays show strong and diffuse S100 and SRY-related HMG-box 10 expression. [3] Inflammatory myofibroblastic tumors (IMTs) are composed of myofibroblastic spindle cells and variable inflammatory cells, sometimes with a myxoid background, but the absence of a typical plexiform growth pattern and positivity for ALK immunoreactivity can help distinguish IMTs from PF. 52 [4] Inflammatory fibroid polyps show interwoven fascicles of CD34-positive spindle cells, loose and edematous stroma, and prominent inflammatory cells, especially eosinophils. The most important characteristic is the absence of a plexiform structure. 53 [5] Microscopically, gastric leiomyomas contain irregular fascicular smooth muscle cells with brightly eosinophilic cytoplasm and blunt-ended nuclei. The immunohistochemical staining of leiomyomas shows positivity for desmin, SMA, and caldesmon. [6] Desmoid fibromatosis is a histologically benign but locally aggressive lesion with a marked tendency to recur. Characteristic staining includes β-catenin nuclear reactivity. 54 [7] Gastroblastoma is a biphasic tumor arising in the gastric muscularis propria and consisting of uniform spindle and epithelial cells arranged in nests. Similar to PF, the spindle cells often have a myxoid background with a multinodular growth pattern, and both tumors share the same gene fusion (MALAT1-GLI1). However, spindle cells express CD56 and CD10 instead of SMA in PF. The most important defining characteristic is that PF lacks an obvious epithelial component.
Conclusion
Here, we report two new cases of PF, which is a rare mesenchymal tumor with benign biological behavior and no reports of recurrence or metastasis. The tumor is characterized by a plexiform growth pattern and contains a rich myxoid matrix with bland spindle cells and a delicate capillary network. Recognizing this rare entity is important to avoid misdiagnosis with other mesenchymal neoplasms of the gastrointestinal tract. Broad antibody panels should be used in routine differential diagnosis work.