
Abstract
The gastrointestinal tract is an uncommon site for metastasis. Gastrointestinal metastasis of melanoma is usually asymptomatic, often affects the small intestine (81.1%) and the colon (15.1%), and rarely affects the stomach. Our patient was a 40-year-old man presenting with gradually worsening dyspepsia of a few weeks’ duration. He did not mention other gastrointestinal symptoms, and he was not anemic. He had a history of auricular melanoma, which was resected. A black lesion with a diameter of approximately 20 mm was detected in the body of his stomach during upper gastrointestinal endoscopy. Biopsies were taken, and the diagnosis of metastatic melanoma was confirmed by immunohistochemistry (IHC). A gastrointestinal work-up, computed tomography (CT), and positron-emission tomography (PET) did not reveal additional lesions. The lesion in the stomach was resected, and a new course of chemotherapy was initiated. A lower threshold should be considered for gastrointestinal work-up in patients with melanoma.
Introduction
Melanoma is an aggressive skin cancer with an increasing incidence. 1 Melanoma is more common in lower latitudes and in older patients compared with higher latitudes and younger patients. 2 Melanoma is associated with a high mortality rate and accounts for a high proportion of cancer-related years of life lost per death from the disease. 2 Owing to the aggressive nature of this cancer and the poor response to chemotherapy, prevention and early diagnosis can effectively decrease the associated mortality rate. 3
Metastatic melanoma often spreads to the gastrointestinal tract, 4 usually affects the small bowel (81.1%) and colon (15.1%), and rarely affects the stomach (3.8%). 5 Gastrointestinal metastases can manifest as ulcerative, infiltrating, polypoid, cavitary, exoenteric, or small black spot-like lesions.5,6 The majority of gastrointestinal melanomas remain asymptomatic and are not diagnosed until autopsy.7,8 Here, we present a rare case of melanoma with gastric metastasis that manifested solely as dyspepsia.
Case report
The patient was a 40-year-old man with dyspepsia that began a few weeks prior to referral and that had worsened recently. He had no other symptoms, such as nausea, vomiting, hematemesis, melena, change in bowel habits, or weight loss. He was not anemic. The previous year, he was diagnosed with auricular melanoma, which was subsequently resected, and surgery was followed by chemotherapy with ipilimumab, 10 mg/kg every 3 weeks for four doses. He did not complete treatment because of poor compliance. At presentation to our clinic, he did not mention other medical or psychosocial conditions and was not taking medications. On physical examination, we found no significant findings, such as lymphadenopathy, hepatosplenomegaly, or tenderness.
The patient underwent upper gastrointestinal endoscopy at our hospital to rule out important etiologies, such as cancer and peptic ulcer disease. A black lesion with a diameter of approximately 20 mm was detected in the body of the stomach (Figure 1). Biopsies were taken, and histopathology revealed sheets of mitotically active cells with prominent nuclei. Additionally, melanin pigment was observed in some cells. The specimens were strongly positive for markers of melanoma, such as human melanoma black 45 (HMB-45) and Melan-A in immunohistochemistry (IHC) (Figure 2). Other parts of the gastrointestinal tract were normal on endoscopy, and no lesions were detected on computed tomography (CT). There was also no significant uptake on positron-emission tomography (PET), except in the gastric lesion. Palliative resection of the gastric lesion was performed with wide margins. The resection margins were clear, and no nodal involvement was detected in pathological assessments. Subsequently, the patient was treated with ipilimumab intravenously at 3 mg/kg every 3 weeks, for four doses. Mild adverse events, such as fatigue and diarrhea, occurred during treatment, which were tolerable for the patient. Long-term dermatological and gastrointestinal follow-up and serial imaging were recommended to the patient for early diagnosis of recurrence.
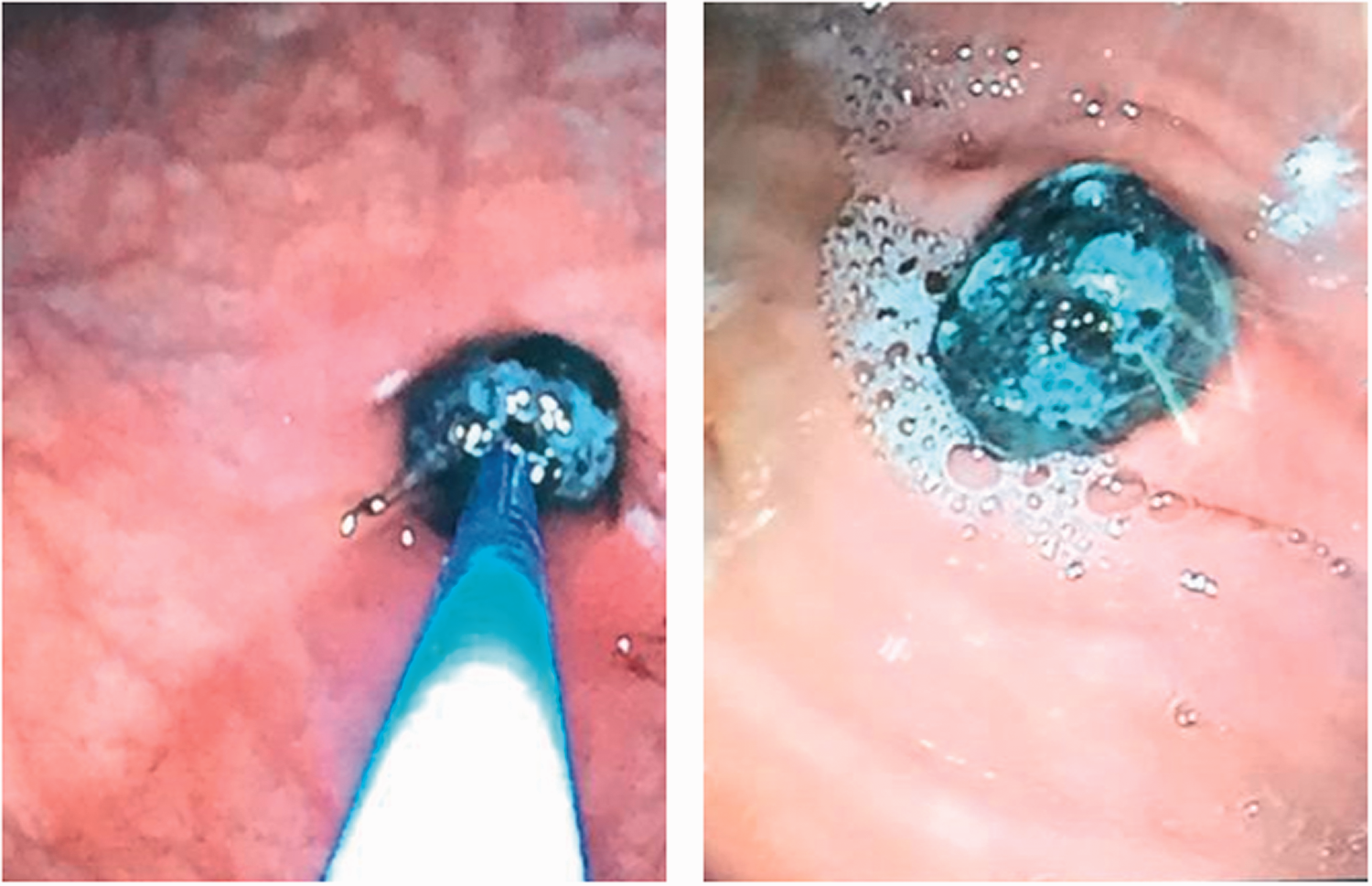
A black lesion was found in the body of the stomach during upper gastrointestinal endoscopy.

Histopathological findings in the resected gastric melanoma; hematoxylin and eosin (H&E) staining (a) and immunohistochemical (IHC) findings with HMB-45 staining (b). Magnification, ×100.
The reporting of this study conforms to the CARE guidelines. 9
Discussion
The gastrointestinal tract is an uncommon site for metastasis, and metastatic melanoma is among the most common types of cancer that spread to the gastrointestinal tract. 7 However, the stomach is an uncommon site of metastasis for melanoma. 5 Herein, we have reported an unusual case of melanoma with gastric metastasis and dyspepsia.
Gastrointestinal melanoma is often asymptomatic and found during autopsy.7,8 However, melanoma of the gastrointestinal tract can manifest with symptoms of dyspepsia, abdominal distension, nausea, vomiting, hematemesis, melena, iron deficiency, weight loss, bowel obstruction, and intussusception.4,6,10 The symptoms of gastrointestinal involvement can be non-specific and may manifest even 15 years after the initial diagnosis of melanoma. 8 Gastrointestinal melanoma can be multifocal and is usually found by careful assessment of the gastrointestinal tract. 11 Considering the high prevalence of gastrointestinal involvement in melanoma, physicians should consider gastrointestinal work-up even in patients with non-specific symptoms.
Endoscopic evaluation of the gastrointestinal tract is an effective method to diagnose gastrointestinal melanoma.12,13 Owing to the high prevalence of intestinal involvement in metastatic melanoma and the absence of specific gastrointestinal symptoms, video capsule endoscopy and enteroscopy can increase the diagnostic yield. 7 Melanomas can appear as polypoid, mass-like, amelanotic, ulcerated, or friable lesions. 13 Black plaques and pigmented lesions are highly suggestive of primary or secondary gastrointestinal melanoma on endoscopy. 12 Melanoma can also manifest as an irregular filling defect with barium swallow and radiography. 12 Endoscopic ultrasonography can determine the depth of infiltration of gastrointestinal melanoma. 12 Histopathological findings can confirm the diagnosis of gastrointestinal melanoma; 12 however, although melanin particles may be present, these can be absent in poorly differentiated melanoma. 12 Immunohistochemical examinations with monoclonal antibodies for melanoma, such as HMB-45, S-100, and vimentin, can accelerate the diagnosis of melanoma. 12
Recently, the use of BRAF-targeted therapies and immune checkpoint inhibitors have increased the survival of patients with metastatic melanoma.7 However, patients’ 5-year overall survival after diagnosis of advanced metastatic melanoma is approximately 52%. 7 Lymphocytic gastritis is an adverse effect of immunotherapy that can occur during the treatment of metastatic melanoma. 14 Surgical intervention for metastatic gastrointestinal melanoma alleviates patients’ symptoms, and improves their survival. 7
In conclusion, the gastrointestinal tract is a rare destination for metastatic tumors; however, metastatic melanoma often spreads to the gastrointestinal tract. Metastatic melanoma usually remains asymptomatic and rarely spreads to the stomach. However, gastrointestinal melanoma causes non-specific symptoms; hence, a lower threshold for endoscopic examination in patients with a previous history of melanoma is rational. Currently, metastatic melanoma of the gastrointestinal tract is treated with local resection, systemic chemotherapy, and immunotherapy.
Footnotes
Author contributions
Zahedin Kheyri: Conceptualization, Writing-review and editing; Masoomeh Shiravi Khoozani: Project administration, Resources; Moein Ala: Writing-original draft, Writing-review and editing.
Ethics statement
This case report was performed in accordance with the ethical standards defined by the 2013 version of the Declaration of Helsinki and with the approval of the Ethics Committee of Tehran University of Medical Sciences. The patient did not undergo any additional interventions for this article, and the patient provided written consent for publication.
Patient’s perspective
The patient was generally satisfied with the treatment. After recurrence, he was more compliant regarding follow-up and the early diagnosis of possible recurrence.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.