
Abstract
We herein describe the preoperative and postoperative clinical data of a patient with a rare case of vulvar malignant melanoma and discuss her clinical characteristics and prognosis. After surgical resection and immunotherapy, the patient’s illness continued to worsen. She then received local vulvar radiotherapy. However, further treatment was discontinued because of intolerable complications of radiotherapy, and the patient died about 18 months postoperatively. Management of vulvar malignant melanoma is challenging. No unified, effective, and standardized diagnostic and treatment plan has been established for this disease. Surgery remains the primary treatment modality for locally resectable vulvar malignant melanoma. Radiation therapy and chemotherapy do not benefit survival. Encouragingly, however, immunotherapy and targeted therapy have shown clinical efficacy in metastatic vulvar malignant melanoma.
Keywords
Introduction
Malignant melanoma is a life-threatening skin tumor derived from melanocytes. Vulvovaginal melanoma (VVM) represents an important subgroup of malignant melanoma with a distinct biology and mutational profile. 1 Data regarding VVM remain scarce. A recent United States population‐based study of 1863 patients showed that survival remains poorer than that of cutaneous melanomas, with lymph node involvement being the most important prognostic factor. 2 In the absence of VVM trials, treatment recommendations are mainly extrapolated from cutaneous melanomas.3,4 We herein describe a patient with vulvar melanoma who underwent surgical resection and adjuvant treatment. Unfortunately, her primary tumor progressed and she developed disseminated metastases.
Case report
A 42-year-old woman sought treatment for a 6-month history of vulvar itching and pain in June 2014. The patient was admitted to our hospital approximately 1 month after her initial presentation to her local hospital. The doctor at the local hospital had biopsied diseased tissue from her vulva, and the pathological result was malignant melanoma of the vulva. The result of the pathology consultation in our hospital was the same as that at the local hospital. No moles were seen on the skin or mucous membranes of the patient’s body, and other physical examination findings were normal. The gynecological examination revealed ulcerative black lesions with a diameter of about 1.5 cm on the anterolateral right side of the clitoris. Inguinal ultrasound showed enlarged right inguinal lymph nodes. Other preoperative examination findings were normal, including assessment of the regional lymph nodes of the neck, axillae, and popliteal fossae; ultrasound; thoracic, upper abdominal, lower abdominal, and pelvic computed tomography; a whole-body bone scan; and head magnetic resonance imaging. Based on the results of the pathologic examinations and inguinal ultrasound results, the patient underwent extensive vulvectomy and bilateral inguinal lymphadenectomy. A section of vulvar tissue measuring 12.0 × 7.5 × 2.5 cm was excised, and a gray-black raised lesion measuring 2.0 × 1.3 × 1.0 cm was seen next to the clitoris. The cut surface of the mass was gray-black and tough with shallow surface penetration. Pathological examination showed that the lesion was a malignant melanoma that invaded the epidermis but did not involve the margin (Figure 1). One of the right inguinal lymph nodes exhibited massive coagulation necrosis with the presence of fibrosis and phagocytic melanocytes. The possibility of tumor cells was not ruled out. Immunohistochemistry was unsuccessful because of the high amount of pigment. The patient received a subcutaneous injection of 3 million units of interferon-α every other day for 14 months. After the checkpoint inhibitor was approved for marketing, she started using interferon-α in January 2015.

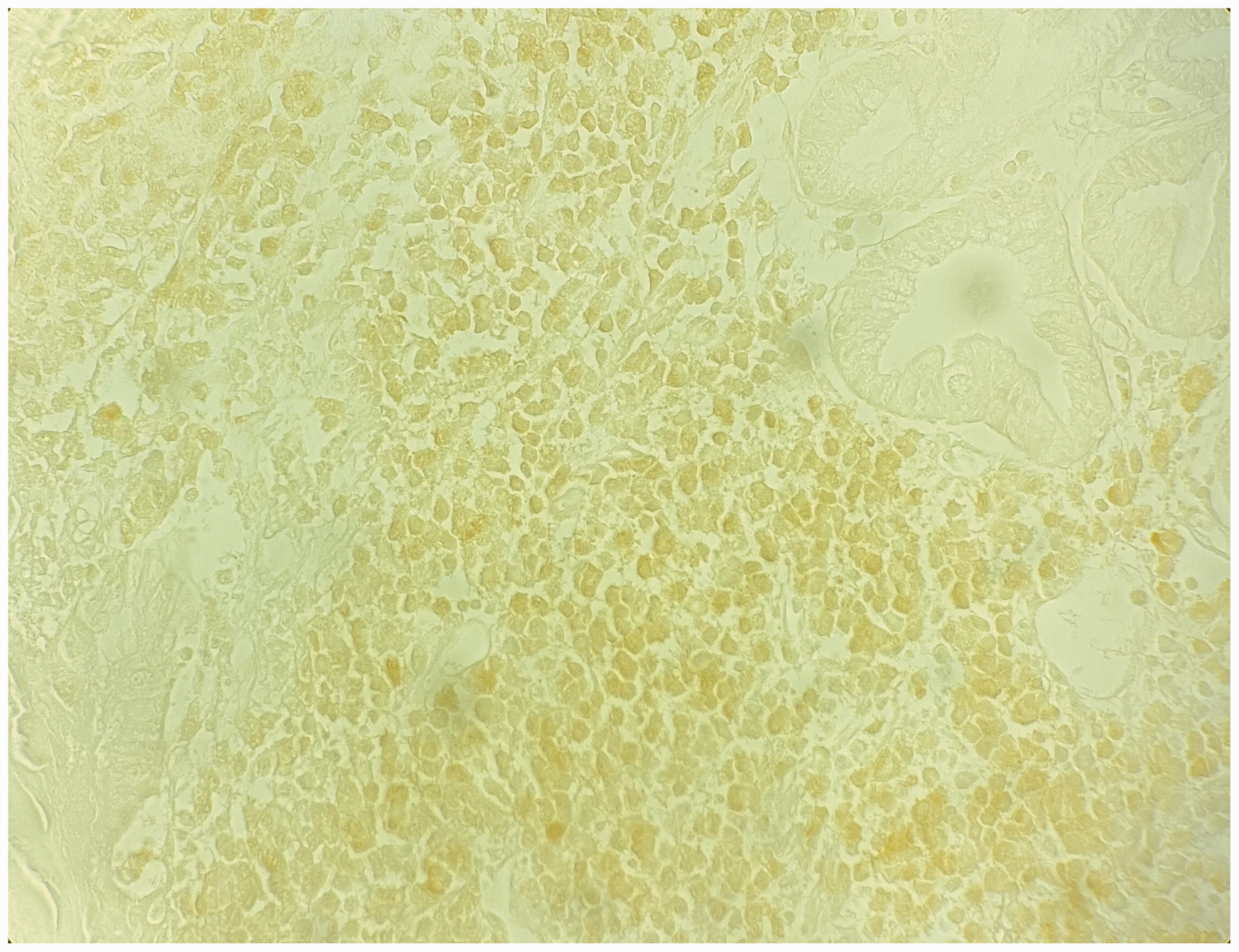
Pathological specimen obtained during extensive vulvectomy. Examination revealed tumor tissue invading the epidermis, consisting of fusiform and polygonal cells with clear cytoplasm and pale staining, unclear cell boundaries, distorted and strange nuclei, fine chromatin, and rare mitotic figures; pigment is visible in the local cytoplasm, and the histological findings were in accordance with melanoma.
Sixteen months postoperatively, the patient returned because of gradual enlargement and bleeding of the vulvar lump. Positron emission tomography–computed tomography showed multiple metastases in the lungs, liver, breasts, stomach, and bone. Suspicious lesions were present in the lungs, liver, right breast, stomach, mesentery, iliac joints, and knee joints. Combined with the immunohistochemistry results, examination of a gastric biopsy specimen obtained under gastroscopy confirmed metastasis of vulvar melanoma (Figures 2–4). The patient began local vulvar radiotherapy to manage vaginal bleeding. She eventually discontinued further treatment because of intolerable complications of radiotherapy, especially diarrhea, and died about 18 months postoperatively.

Gastric histopathological specimen (hematoxylin–eosin ×4).
Gastric histopathological specimen (S100).

Gastric histopathological specimen (HMB-45 antibody).
Discussion
We have herein reported a rare case of rapidly progressing vulvar melanoma. The disease continued to develop even after surgical resection and interferon-α therapy, and the patient received local vulvar radiotherapy. However, she eventually discontinued further treatment because of intolerable complications of radiotherapy. Her disease rapidly progressed, and she died 2 months later.
Although no prospective trials have been conducted for VVM, many key trials have included mucosal melanomas. Treatment strategies for VVM are based on expert consensus and have mainly been extrapolated from cutaneous melanomas.3,4
The treatments for VVM have mostly been extrapolated from cutaneous melanoma. Surgical excision with adequate margins remains the optimal treatment strategy for localized mucosal melanoma. 4 However, VVMs are often diagnosed at advanced disease stages, which sometimes complicates the achievement of surgical resection with optimal margins. 3 Both the prospective GOG-73 study of 81 patients and a recent United States population-based study of 1863 patients highlighted the prognostic role of lymph node involvement. 5 Lymph node assessment should therefore form an integral part of the treatment of localized disease. With clinically and radiographically normal-appearing lymph nodes, this is usually done by the sentinel node technique. The mitotic rate has been shown to be an independent prognostic factor. 6 Surgery is the cornerstone of treatment of primary VVM; however, patients’ postoperative quality of life and mental health are affected because of the anatomical location of the disease. Adjuvant radiation therapy and chemotherapy do not benefit survival. 7 The interest in the genetic profile of mucosal melanoma has recently grown. With the improvement and popularization of genetic testing technology, immunotherapy and targeted therapy have provided new ideas for the treatment of VVM. In particular, checkpoint inhibitors have achieved excellent results in the treatment of melanoma. Nivolumab and pembrolizumab have been approved for the treatment of metastatic melanoma. 8 They have shown promising results in cutaneous melanoma, but there is still much work to be done in this area for VVMs. 9
In summary, this case highlights that the treatment of VVM requires centralization of care in a multidisciplinary setting. Immunotherapy and targeted therapies provide new hope for the treatment of VVM, but their impact on survival needs to be addressed in future studies.
Footnotes
Acknowledgements
We thank the medical technicians working in the Affiliated Hospital of Qingdao University for their help.
Authors’ contributions
Wenjing Li was responsible for the study design and the writing and editing of the report. Jingzhi Song was responsible for the acquisition of clinical data, pathological review, study design, and editing of the report. Yiming Sun was responsible for the acquisition of clinical data, acquisition of informed consent, conception of the work, and manuscript editing. Zhumei Cui was responsible for the study design, editing of the report and later revisions.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Informed consent was obtained from the patient for publication of this case report. All identifying information was removed from this manuscript. The need for ethical approval was waived because this is a report of clinical practice and does not constitute biomedical research. The reporting meets all ethical requirements.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.