
Abstract
Objective
This study aimed to investigate the patterns of patients managed at the oral medicine service centres at the Faculty of Dentistry, University of Otago, New Zealand and Weifang People’s Hospital, Weifang, China.
Materials and methods
Patients’ clinical records were collected from 2015 to 2020. Patient data from electronic and paper records were examined. The data included in this study for each patient were age, sex, ethnicity, source of referral, clinical investigation, diagnosis, and management.
Results
There were 99,603 patients included in the analysis. Most of the patients (56.5%–71.0%) were women aged 50 to 70 years. Referrals were typically from internal sources (20.0%–52.7%), medical practitioners (27.5%–29.6%), and dental practitioners (18.3%–28.3%). The main clinical investigations included blood tests (22.1%–25.4%), diagnostic imaging (12.2%–28.3%), and biopsy (9.4%–12.8%). Oral and maxillofacial pathology accounted for 73.9% to 83.3% of all diagnoses. The main treatment was self-care (15.2%–36.6%), and the most prescribed medication was a corticosteroid (26.4%–30.2%).
Conclusions
Most patients in oral medicine clinics were 50 to 70-year-old women. Blood tests, imaging, and biopsy were the main clinical investigations. Most of the diagnoses were oromucosal diseases. The main treatments were self-care and corticosteroid prescriptions.
Keywords
Introduction
Oral medicine is the dental specialty concerned with establishing a clinical diagnosis and beginning non-surgical management of patients with chronic or recurrent medical-related disorders of the oral and maxillofacial anatomical region. 1 Oral medicine specialists typically work closely with medical specialists and provide co-managed care for patients who may require a multidisciplinary approach. Oral medicine specialists also collaborate with other dentists to coordinate dental treatment for patients with complex medical conditions. 2
Oral medicine services are available as an essential service component in most larger hospitals and dental schools; in developed countries with a high patient volume, the availability of complimentary private oral medicine services is also a necessity. 3 Studies on the prevalence of oral lesions are feasible by recruiting participants from the oral medicine services at dental schools,4–6 hospitals, and private oral medicine clinics.7,8 For example, in a Turkish study of patients referred for oral medical care, most patients had no detectable lesions and approximately 15% of the patients had detectable mucosal lesions. 6 Anatomical changes, particularly Fordyce’s spots and a linea alba, were the most common oral conditions referred. This study offered some epidemiological data related to oral mucosal lesions in the Turkish population. However, it only focused on oral mucosal lesions, while other complex oral lesions involving the salivary gland, temporomandibular disorders, and orofacial pain were not reported. A study conducted in the United States covered a broad spectrum of oral medicine-related conditions, including salivary gland and orofacial pain disorders. 8 Analysis of records from patients who were referred to the oral medicine clinic between 2008 and 2010 indicated that immune-mediated conditions were the most common diagnoses. A recent 1-year retrospective Canadian study revealed that immune-mediated conditions were the most common diagnoses for referrals. 4 Finally, a 5-year Australian study with 1604 patients indicated that hyperplastic mucosal lesions were the most common diagnoses. 7
In New Zealand, there are currently five registered oral medicine specialists. In Dunedin (population of approximately 128,800), New Zealand, the oral medicine service is part of the oral health service provided at the Faculty of Dentistry, University of Otago. In Weifang city (population of approximately 9.2 million), China, there are three chief physicians, three associate chief physicians, three attending physicians, and three resident dentists. The oral medicine service is part of the Weifang People’s Hospital general health service. Patient patterns in oral medicine services are of clinical importance, but the available information related to this issue is limited in both New Zealand and China.
This study aimed to investigate and compare the patterns of patients seen in the oral medicine clinics at the Faculty of Dentistry, University of Otago, New Zealand and Weifang People’s Hospital, Weifang, China. The main focus was on patients’ demographics, diagnostic services used for making a diagnosis, the spectrum of orofacial conditions encountered, and treatments provided by the oral medicine services.
Methods
The study was approved by Human Research Ethics Committee, University of Otago (HD 20/111) and the Weifang People’s Hospital Ethical Committee (2021004). The ethics committees waived the requirement for informed consent because this was a retrospective study with anonymity of personal information. This retrospective case record review study included data from electronic and paper clinical records of patients managed by the oral medicine services at the Faculty of Dentistry, University of Otago, New Zealand and Weifang People’s Hospital, Weifang, China from January 2015 to December 2020. The reporting of this study conforms to STROBE guidelines. 9 Inclusion criteria for this study were all patients who attended our hospitals for consultation, diagnosis, management, and follow-up. Exclusion criteria for this study were patients with inappropriate referrals or insufficient referral or patient details.
Data from all patients were recorded and stored in a password-encrypted spreadsheet program (Microsoft Corp., Redmond, WA, USA). The variables included the patient’s demographic information, the reason for referral, referring doctor’s specialty, laboratory investigations and imaging tests ordered at the consultation visit, and clinical diagnosis based on specialist evaluation and management. An internal referral was defined as a referral from within the dental hospital. An external referral was defined as a referral from outside the dental hospital. The various diagnoses were categorised into the following two major disease groups: orofacial pain and oral and maxillofacial pathology. Oral and maxillofacial pathology was further subdivided into subcategories on the basis of the “World Health Organization (WHO): a digital manual for the early diagnosis of oral neoplasia” and the “World Health Organization (WHO) classification of head and neck tumours.”10,11
Statistical analysis
Data were statistically analysed using IBM Statistical Package for Social Sciences (SPSS) version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as the mean ± standard deviation (SD) if normally distributed and compared using the Student’s t-test. Categorical variables were presented as the count and percentage and compared using the chi-square test. P < 0.05 was considered to be significant.
Results
Patient demographic characteristics
There were 99,603 patients included in this study from the two oral medicine centres (Table 1).
Patients’ age and sex (N, %) in oral medicine clinics between 2015 and 2020.

In Weifang, China, 97,070 patients were seen in oral medicine services between 2015 and 2020. Most patients were 50 to 70 years old (38.0%) and 30 to 50 years old (33.7%), with a mean age of 51.2 ± 21.0 years (range, 1 month–96 years). There were more women (56.5%) than men enrolled in this study.
In Dunedin, New Zealand, 2533 patients were seen at the oral medicine service between 2015 and 2020. Most patients were 50 to 70 years old (56.3%), with a mean age of 53.6 ± 19.0 years (range, 2–92 years). There were more women (71%) than men enrolled in this study.
Referral sources
In Weifang, China, 80% of the referrals were from external sources, with the greatest proportions coming from medical practitioners (29.6%), dental practitioners (28.3%), physiotherapists (12.6%), and other oral health practitioners (8.1%). The mean age for women was 51.8 years, which was younger than that of men (54.0 ± 19.6 years; P < 0.01) (Table 2).
Patients’ age (mean ± SD) and sex among referrals, oral and maxillofacial pathology, orofacial pain, temporomandibular disorder, oral lichen planus, and fibro-epithelial polyp.

TMD, temporomandibular disorder; OLP, oral lichen planus; FEP, fibro-epithelial polyp; SD, standard deviation.
In Dunedin, New Zealand, 47.3% of the referrals were from external sources, with the greatest proportions of these from medical practitioners (27.5%), followed by dental practitioners (18.3%), physiotherapists (0.4%), and other oral health practitioners (0.3%) (Figure 1). More women were referred to oral medicine clinics than men. The mean age for women was 54.5 years, which was younger than that of men (57.7 ± 17.8 years; P < 0.01) (Table 2).

Pattern of referral pathways to oral medicine.
Clinical investigation
A patient may present with more than one condition, which requires more than one clinical investigation or test to be conducted. The clinical tests performed for patients are summarised in Figure 2. Blood test (22.1%) was the most common test followed by biopsy (12.8%) and extraoral radiography (8.9%) in Dunedin, New Zealand. Comparatively, in Weifang, China, blood test (25.4%) was the most frequent test followed by cone beam computed tomography/computed tomography (CT)/magnetic resonance imaging/ultrasound (16.7%) and biopsy (9.4%). Approximately one-quarter of all patients who attend oral medicine clinics (36.3%, Dunedin; 20.1%, Weifang) required no further tests or investigations. Other tests, such as sialometry, smear, swab, cytology, and fine needle aspiration were uncommon at both centres.

Main investigation or special tests.
Diagnosis
Each patient could have more than one diagnosis (Figure 3). In Weifang, China, oral and maxillofacial pathology accounted for 83.3% of all diagnoses followed by 16.7% for orofacial pain. The three most common diagnoses were temporomandibular disorder (9.3%), oral lichen planus (8.8%), and recurrent aphthous stomatitis (6.3%). The frequency of normal oral mucosa/common anatomical variations (e.g., Fordyce granules and exostosis [or tori]) and unconfirmed/unclear diagnosis was 3.7% and 2.1%, respectively.
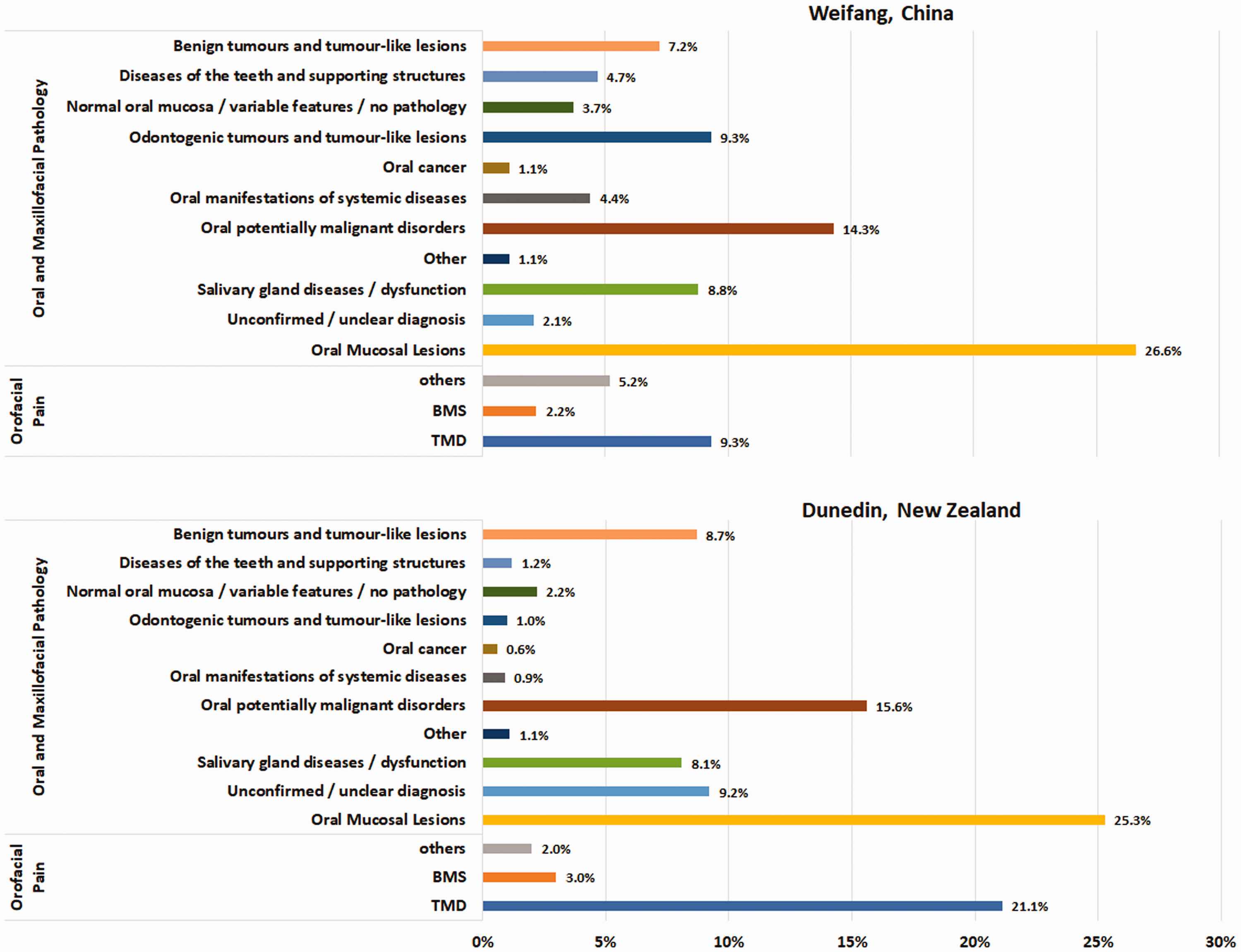
Most frequently diagnosed conditions.
Oral and maxillofacial pathology included oral mucosal lesions (26.6%), salivary gland diseases or dysfunction (8.8%), oral manifestations of systemic diseases (4.4%), oral potentially malignant disorders (14.3%), odontogenic tumours and tumour-like lesions (9.3%), benign tumours and tumour-like lesions (7.2%), diseases of the teeth and supporting structures (4.7%), and oral cancer (1.1%). Among the oral mucosal lesions, 7.2% were categorised as infections (e.g., angular cheilitis, oral candidosis, chronic hyperplastic candidosis, median rhomboid glossitis, squamous papilloma, verruca vulgaris, herpetic gingivostomatitis, and Staphylococcus aureus infection), 16.2% involved ulceration and vesiculobullous diseases (e.g., traumatic ulceration, recurrent aphthous stomatitis, traumatic ulcerative granuloma with stromal eosinophilia, pemphigoid, and pemphigus), 1.4% were pigmented lesions (e.g., amalgam tattoo, melanotic macule, melanocytic nevus, and smoker’s melanosis), and the other 1.8% were various benign conditions such as geographic tongue (erythema migrans), frictional keratosis, gingival hyperplasia, and nicotinic stomatitis. Oral potentially malignant disorders included oral lichen planus (8.8%), actinic cheilitis or solar keratosis (2.3%), and leukoplakia (2.2%). Erythroplakia, proliferative verrucous leukoplakia, and verrucous hyperplasia had a prevalence of less than 1%. Xerostomia and hyposalivation (3.4%) represented the chief complaints in the salivary gland diseases or dysfunction category, followed by Sjogren syndrome (2.5%), mucocele (1.2%), and sialolithiasis (0.5%). Other salivary gland diseases had a prevalence of 1.2%. The most common benign tumours or tumour-like lesions were fibroepithelial polyp (5.9%) followed by vascular malformation (1.0%). Others such as pyogenic granuloma, fibrous epulis, lipoma, and granular cell tumour all had an almost similar distribution at 0.1%.
The most common cause of orofacial pain was temporomandibular disorder (9.3%). Additionally, burning mouth syndrome accounted for 2.2% and the other orofacial pain including, but was not limited to, trigeminal neuralgia, persistent dental alveolar pain, persistent idiopathic facial pain, and paroxysmal hemicrania accounted for 5.2%.
In Dunedin, New Zealand, oral and maxillofacial pathology accounted for 73.9% of all diagnoses, followed by 26.1% for orofacial pain. The three most common diagnoses were temporomandibular disorder (21.1%), oral lichen planus (11.3%), and fibroepithelial polyp (4.4%). The prevalence of normal oral mucosa/common anatomical variation and unconfirmed or unclear diagnoses was 2.2% and 9.2%, respectively.
Oral and maxillofacial pathology included oral mucosal lesions (25.3%), oral potentially malignant disorders (15.6%), salivary gland diseases or dysfunction (8.1%), benign tumours and tumour-like lesions (8.7%), diseases of the teeth and supporting structures (1.2%), other (1.1%), odontogenic tumours and tumour-like lesions (1.0%), oral manifestations of systemic diseases (0.9%), and oral cancer (0.6%). Among the oral mucosal lesions (25.3%), 7.9% were categorised under infections, 4.3% involved ulceration and vesiculobullous diseases, 3.1% were pigmented lesions, and the other 10.0% were various benign conditions such as geographic tongue, frictional keratosis, gingival hyperplasia, and nicotinic stomatitis. Oral potentially malignant disorders included oral lichen planus (11.3%), actinic cheilitis or solar keratosis (1.8%), and leukoplakia (1.0%). The prevalence of other oral potentially malignant disorders was less than 1.5%. Xerostomia and hyposalivation (4.1%) represented the chief complaints under the salivary gland diseases or dysfunction category followed by Sjogren syndrome (2.0%), mucocele (1.3%), and sialolithiasis (0.4%). The prevalence of other salivary gland diseases was 0.3%. More than half of the benign tumours or tumour-like lesions were fibroepithelial polyps followed by vascular malformation (1.2%), while other lesions accounted for 3.1%.
The most common cause of orofacial pain was temporomandibular disorder (21.1%). Burning mouth syndrome accounted for 3.0% and other pain disorders were 2.0%. In all age groups, no significant differences with respect to sex were observed for all conditions.
Treatment
In Weifang, China, 9.8% of patients did not require further treatment. However, several other patients received more than one type of treatment. Further treatment included self-care instructions and education (15.2%), general dental treatment (such as restorative, endodontics, and denture-related management; 8.4%), physiotherapy (6.0%), minor oral surgery (4.5%), and other (which includes referrals to other dental specialists and multidisciplinary areas; 9.2%). No information on the treatment was found in 4.6% of the patients’ records (Figure 4). Among patients attending the oral medicine clinics, 42.3% of the patients were prescribed medications as a part of their treatment. Some patients were prescribed more than one medication, and medications were classified in accordance with the New Zealand formulary. Additionally, 5.2% of the medications were not specified. The most commonly prescribed medication was corticosteroids (26.4%) followed by antifungals, antibiotics, dry mouth treatment medications (such as dry mouth gel), anaesthetics, antiepileptics/antidepressants/related medications, antivirals, antiseptic mouthwash, analgesics and non-steroidal anti-inflammatories (NSAIDs), and capsaicin. The frequency of other medications including supplements was 2.1%.

Common management and treatment.
In Dunedin, New Zealand, 7.3% of the patients did not require further treatment. No information on the treatment was found in 7.1% of the patients’ records. More than one-third of the patients (36.6%) were provided with self-care instructions and education. Other management included general dental treatment (10.3%), minor oral surgery (9.9%), referrals to other disciplines (2.8%), and physiotherapy (1.6%). Among patients attending the oral medicine clinic, 24.4% were prescribed medications as a part of their treatment. The most commonly prescribed medication was corticosteroids (30.2%) followed by antifungals, dry mouth treatment medications, analgesics and NSAIDs, capsaicin, antiepileptics, antidepressants and related medications, and anaesthetics. Other medications (vitamin supplements and injections), antiseptics mouthwash, antibiotics, and antivirals were rarely prescribed (≤3% each).
Discussion
A good understanding of oral medicine services is important for delivering patient-centred care and optimising hospital resources. Both institutions are public, and patients can attend them either by professional or self-referral. This study analysed a large sample size of 99,603 patients who were managed at two international oral medicine centres (Faculty of Dentistry, University of Otago, New Zealand and Department of Stomatology, Weifang People’s Hospital, Weifang, China) between 2015 and 2020. Most of the patients were 50 to 70 years old, and most of the patients were women. Blood tests, imaging, and biopsy were the most commonly used clinical investigations. Management strategies included self-care instructions and education, medications, general dental treatment, minor oral surgery, physiotherapy, and referrals to other dental specialists or multidisciplinary teams.
First, the results of this study provided doctors and dentists with clinically new and useful information. There is a considerable demand for dental services dealing with orofacial lesions and conditions, which are often misconceived by doctors and dentists as diseases that are outside the scope of oral medicine. Second, these study results can assist policy-makers in maximising hospital resources and optimising health care funding. Third, these results are also helpful for the development of both dental and oral medicine student curricula, and they inform the design of continuing education courses for dentists and physicians.
The limitations of this study included insufficient medical and dental records for some patients; some old prescriptions were written on paper prescription pads and were not entered into the computer system or recorded in the patient files. Similar to other studies that were based on convenience samples, this study only retrospectively analysed data from Weifang, China and Dunedin, New Zealand. The results may not fully represent the general population of these two countries. The prevalence and spectrum of the orofacial diseases were different between these two centres, which may be a result of differences in the national healthcare systems and populations. Oral medicine training systems are different in China and New Zealand, and therefore, the presence of physicians with different levels of expertise in oral medicine may introduce bias when making a diagnosis. However, these study results provided insight into the range of orofacial conditions that were diagnosed and the use of oral medicine services in Weifang, China and Dunedin, New Zealand.
The number of patients seen at the two oral medicine clinics was different. Weifang had more patients who were treated by the oral medicine service compared with that in Dunedin. This may be because before 2018, there was one consultant working part-time and after 2018, this was increased to one full-time and one part-time consultant at the Faculty of Dentistry, University of Otago in Dunedin. However, there were always three chief physicians, three associate chief physicians, three attending physicians, and three resident dentists working in Weifang, China between 2015 and 2020. Among the 99,603 different patients who had attended the oral medicine services, most of them were women. This result was in agreement with the results of other studies.4,5,7,8 Patients who attended the oral medicine services had a wide age range, but they were mostly 50 to 70 years old. The mean age in the present study is similar to that reported by Villa et al. 8 and Friesen et al., 4 but slightly higher than that in previous studies.5,7 Age and sex differences may have been observed because women may have acted more positively toward oral health compared with men. 12 Differences between the patients’ age groups were observed between the evaluated institutions. This may be because New Zealand has an ageing population. Furthermore, the prevalence of common mucosal pathologies, such as oral lichen planus 13 and orofacial pain conditions such as temporomandibular disorder, 14 are higher in middle-aged women compared with those in men.
More than half of the patients attending the oral medicine services were from internal referrals, medical practitioners, and dental practitioners. The distribution of referral sources is similar to that in other studies.5,7 Clinical investigations were requested as indicated by the patients’ medical history and clinical examination data. Some of the conditions, such as traumatic ulceration, frictional keratosis, vascular malformation, melanotic macule, exostosis, geographic tongue, and angular cheilitis, might be clinically diagnosed without additional investigations. Diagnostic imaging was commonly requested for a temporomandibular joint disorder. Biopsies and blood tests were requested most to obtain a definitive diagnosis of certain conditions that cannot be confirmed by clinical examination and radiography and to allow for appropriate management of conditions that could significantly affect the patients’ quality of life.
More oral and maxillofacial pathology was encountered in the oral medicine services compared with that of orofacial pain. This pattern was similar to the results of a study conducted in the United States 8 where orofacial pain contributed to only 25.1% of the total diagnoses and the remainder were oral and maxillofacial pathology. Patients with unconfirmed or unclear diagnoses were encountered in 2.1% to 9.2% of patients, which was mostly attributed to their decision to defer further investigation and stop visiting the oral medicine services before the diagnosis could be finalised, patient records that could not be traced, or inconclusive findings or diagnosis after the examination.
Most of the patients had more than one type of management, and self-care management and education in Dunedin, New Zealand and pharmacology in Weifang, China were the most common management types at these two centres. Some patients (7.3%–9.8%) did not require further treatment, and this was associated with normal oral mucosa/common anatomical variation or stable lesions. General dental treatment was provided to 8.4% to 10.3% of patients who were diagnosed with orofacial pain, diseases of the teeth and supporting structures, or diseases caused by ill-fitting dentures. Minor oral surgery was performed on patients for some common benign tumours and tumour-like lesions. Consistent with other studies, corticosteroids and antifungals seemed to be the most common medications that were prescribed in the oral medicine services. 7 This might be due to immunologically mediated oral diseases that were commonly seen in oral medicine services and that were often managed using a combination of corticosteroids and antifungal medications. A relatively higher proportion of pharmacology management in Weifang, China was observed, whereas minor oral surgery and self-care education were more frequent in Dunedin, New Zealand. This may be because many diseases can be managed in several ways.
Conclusion
Most patients in oral medicine clinics were women who were 50 to 70 years of age. Blood tests, imaging, and biopsy were the main clinical investigations. Most of the diagnoses were oromucosal diseases. The main treatments were self-care and corticosteroid prescriptions. These results provided insight into the range of orofacial conditions that were diagnosed and oral medicine services that were used.
Footnotes
Data availability statement
Data available upon request due to privacy/ethical restrictions.
Declaration of conflicts of interest
The authors declare that they have no competing interests.
Funding
This research did not receive any funding.
Author contributions
The study was performed at the Department of Oral Diagnostic and Surgical Sciences, Faculty of Dentistry, University of Otago, New Zealand and Weifang People’s Hospital, Shandong Province, China. CBH, GGZ, and LM contributed to the conception and design of the experiments and analysis of data. CBH, GGZ, AYL, SYMH, and AP collected the data. CBH, GGZ, AYL, SYMH, LM, and AP contributed to the data interpretation, drafting, and/or revision of the manuscript, and approved the final version of the manuscript. All authors agree to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.