
Abstract
Objectives:
Diabetes mellitus is a metabolic disorder of major public health importance due to its prevalence and potential health complication. The success of long-term maintenance therapy of diabetes patients depends largely on their ability to adherence to self-care practices. Africa’s most populous country, Ethiopia, has the highest burden of diabetes mellitus. However, studies on self-care activities of diabetic patients are limited. Therefore, this study measures the level of self-care activities of diabetic patients in a follow-up clinic of public hospitals in Harar and Dire Dawa, Eastern Ethiopia.
Methods:
A hospital-based cross-sectional study was conducted on 320 randomly selected diabetic patients in Harar and Dire Dawa. A standard diabetic self-care activity interview tool was used to collect the data. Data were entered into Epi-data v 3.1 and STATA v 14.2 was used for analysis. Our outcome variable, self-care activities, has three ordered categories and a robust Ordinal logistic regression was used to identify predictors. All statistical tests with p-value <0.05 were considered as statistically significant.
Results:
The self-care activities of study participants were rated good for 38.1% (95% confidence interval: 32.94, 43.60). Being rural residents (adjusted odds ratio = 0.38, 95% confidence interval: 0.17, 0.82), attended secondary education (adjusted odds ratio = 2.96, 95% confidence interval: 1.51, 5.78), uncontrolled blood glucose (adjusted odds ratio = 1.68, 95% confidence interval: 1.02, 2.79), and had diabetic complications (one, adjusted odds ratio = 1.91, 95% confidence interval: 1.08, 3.38; two or more, adjusted odds ratio = 4.71, 95% confidence interval: 1.81, 12.25) were significantly associated with the better diabetes mellitus self-care activities.
Conclusion:
Significant number of diabetes mellitus patients living in rural areas did not adhere to diabetic self-care activities. This is more evident among participants who have limited or no formal education and patients with controlled blood glucose level. Therefore, individualized diabetic lifestyle education programs in follow-up clinics should target these population groups to improve self-care.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disease that occurs when the pancreas fail to produce enough insulin or when the body cannot effectively use the insulin it produces. 1 The global burden of diabetes among adults over 18 years of age has dramatically risen from 108 million in 1980 to 424.9 million in 2017.2–4 In 2015, an estimated 4.0 million deaths were directly caused by diabetes. 4 According to the 2017 International Diabetes Federation (IDF) report, close to 80% of the global DM burden exist in low- and middle-income countries. 4 Ethiopia, being a low-income country in sub-Saharan Africa, has the highest prevalence of diabetes among Africa’s most populous countries.4,5
Uncontrolled diabetes results in major complications like blindness, kidney failure, heart attacks, stroke, and lower limb amputation.6,7 According to the 2016 report of World Health Organization (WHO), an estimated 1.5 million deaths were directly associated with diabetes in 2012. It was estimated that it will be the seventh leading cause of death in 2030. 2 Obesity, impaired glucose intolerance, insulin resistance, and high blood pressure, low level of high-density lipoprotein cholesterol, gestational diabetes, sedentary lifestyle, family history, age, and polycystic ovarian syndrome are the major risk factors that contribute to the development of DM. 6
Diabetic self-care includes self-monitoring of blood glucose (SMBG), adequate nutrition, physical activity (PA), Foot care (FC), and compliance with medication.8–10 These self-care activities of diabetic patients are vital to keep their health problem under control. Poor self-care activities among diabetic patients are some of the important factors influencing the progression of diabetes and its complications, while they are largely preventable.11,12
Studies show that DM patients’ self-care activities were not adequate in almost all the domains (dietary practice (DP), PA, medication adherence (MA), glucose monitoring (GM), and FC.13–17 Factors such as age, gender, and marital status, level of education and DM complications were identified to affect self-care activities.13,18–20
Self-care in the form of adherence to diet and drugs, blood GM, FC, and exercise are crucial elements in the prevention of DM complication. 21 WHO encourages low- and middle-income countries to take on and provide support for the adoption of effective measures for surveillance, develop a mechanism for the prevention as well as to control diabetes and its complications through a primary health care approach. 7
Despite the benefits of practicing recommended self-care activities, there is limited evidence that used validated tools to assess the overall self-care activities in Ethiopia that will reveal comparable levels of self-care.13–20 Moreover, the current study disaggregated outcome variable into three ordered categories which will be useful to look into gradients of self-care activities. This disaggregation of the dependent outcome variable(s) will help identify the potential areas that need priority for intervention and to identify the factors at all gradient levels. The primary objective of this study was to measure the level of DM self-care activities, and the secondary objective was to identify predictors of DM self-care activities among patients attending diabetes follow-up clinics at public hospitals.
Methods
Study design and setting
A hospital-based cross-sectional study was conducted from June 1 to August 30, 2017 in four public hospitals, two in Harar (Hiwot Fana Specialized University Hospital and Jugal General Hospital), and two in Dire Dawa (Dilchora General Hospital and Sabian Primary Hospital). Harar is the capital city of the Harari Regional State, and it is located on a hilltop in the eastern extension of the Ethiopian Highlands about 526 km East of Addis Ababa at an elevation of 1885 m. Based on figures from the Central Statistical Agency in 2012, the estimated population of Harar was 151,000. Dire Dawa City Administration had an estimated total population of 369,641. 22 Both cities, Harar and Dire Dawa, are 48 km apart and share similar socio-demographic and cultural characteristics.
Population and sample size
All diabetic patients visiting diabetic follow-up clinics for pharmacological therapy at Hiwot Fana Specialized University Hospital, Jegol General Hospital, Dilchora General Hospital, and Sabian Primary Hospitals were considered as source population. Participants excluded from this study include patients who were below the age of 18 years, patients who were unable to provide appropriate information (such as patients with mental problems, hearing impairment, or any others serious health problems), and patients who knows their DM status at the date of the data collection or who did not start DM medication as they lack experience of DM self-care activities.
We used a single population proportion formula in OpenEpi version 3.01 23 to calculate the minimum sample size. Accordingly, 327 samples were obtained using the assumptions of 95% confidence interval (CI), 5% margin of error, 1680 total number of DM patient on follow-up, and 37.3 % of a good self-care practice from a similar study conducted in Tigray, Ethiopia. 24
Sampling with probability proportional to size (PPS) was used to select the study unit. Accordingly, the sample was allocated proportionally to each hospital based on the number of DM patients on follow-up at the said hospitals. A total of 658 patients with DM were being followed up at the clinic in Hiwot Fana Specialized University Hospital wherein 128 were selected for the study. There were 456 diabetic patients at Dilchora General Hospital where 88 selected. Two hundred and twenty patients were identified at the Sabian Primary Hospital where 43 were selected. Finally, there were 346 diabetic patients at Jegula General Hospital wherein 68 were selected. In each hospital, using a systematic random sampling technique, every fifth patient in the sampling frame was included. The first cases were selected using lottery method at each hospital. In case, the selected patients were not availed during period of data collection for any reason; could be absentee, transfer, default and/or death; patients on the next sequence registration number were considered for the study.
Data collection and measurements
Socio-demographic and clinical characteristics data were collected using pre-tested and well-structured questionnaires developed from the review of previous research literature. Standardized and validated tool, the Summary of Diabetes Self-Care Activities (SDSCA) 25 was used to measure diabetes self-care activities. This tool consists of DP, PA, MA, GM, and FC domains. 25 Two core questions in each of the domains were used to measure the overall diabetic self-care activities on the subjects. Responses to each of the items in the six domains ranged from 0 to 7 days, and responses to item-4 were reverse coded. 25 To calculate the overall diabetic self-care practice value, we took the average of the mean values in each of the domains listed above. The summary value marking 25th percentile and below represented a poor level of self-care. Values between the 25th percentile and the 75th percentile (not inclusive) represented a fair level of self-care; 75% percentile and above represented a good self-care level.
Duration of illness was measured from the time a patient was first diagnosed with DM until the date of the survey. The type of medication that a diabetic patient was taking during the time of the survey (either insulin or oral hypoglycemic agent) was referred to as current treatment. Diabetic Healthy Eating Plan refers to the diet that is high in nutrient, low in fat and added sugar, and moderate in calories. Controlled blood glucose level (or target achieved) was defined as fasting blood sugar (FBS) of 70–130 mg/dL.26,27 The data collection tool for this research study was primarily developed in English, then later translated into local languages (Amharic, Afan Oromo, and Somali languages) in consultation with local language experts. This was intended to promote collection of accurate research data. An interviewer administered face-to-face interview and record review were employed to collect data from research participants. Interviews were conducted in the local language before the end of the patients’ visit at the follow-up clinics. Data collectors were trained to conduct the face-to-face interview. Completed questionnaires were reviewed and checked daily by supervisors for accuracy.
Study variables
The dependent outcome variable was diabetic self-care activities, and the independent variables included the socio-demographic characteristics (sex, age, marital status, occupation, level of education, residence, and religion), clinical characteristics (duration of illness, co-morbidities, current treatment, and blood glucose level, DM complication).
Data quality control
Data were collected by personnel’s who had a health background and had a Bachelor of Science degree (BSc) in nursing, and supervised by a research assistant who had a master of public health (MPH). Prior to data collection, the research investigation team provided 2 days orientation to data collectors and supervisors on the objectives of the study, data collection technique, and data collection tools. To check the practicality and applicability of the questionnaire, a pre-test was conducted in a health facility other than the selected ones for the study. Data collection supervisors and the research investigation team checked the data for completeness each day, and double entry was made to validate entry and correct errors if any.
Data processing and analysis
Data were entered into Epi-Data v 3.1. STATA v 14.2 was used for data management and analysis. Both descriptive and inferential statistics were estimated to answer study objectives. A robust ordinal logistic regression, using a user written command in STATA, gologit2 was used to assess factors that are associated with DM self-care activities since this study has three order outcomes (Poor self-care, Fair self-care, and Good self-care). Gologit2 fits three special cases of the generalized ordered logit models: the proportional odds model (POM), the partial proportional odds model (PPOM), and the logistic regression model which were used for this analysis. 28 The POM assumes that predictor variables have the same effect across the categories of the ordinal dependent variable. 29 However, the POM assumptions are often violated as it is common for one or more of predictor variable coefficients vary across values of the dependent category. 28 Gologit2 fits the PPOM where some of the β coefficients can be the same for all values of the response category, while others can differ. In the PPOM, when the autofit option with gologit2 is specified in STATA, the POM assumptions are relaxed only for those variables where it is not justified. 28 We specified the autofit option at the level of significance of 0.05. All statistical tests are declared significant a p-value <0.05.
Results
Socio-demographic characteristics
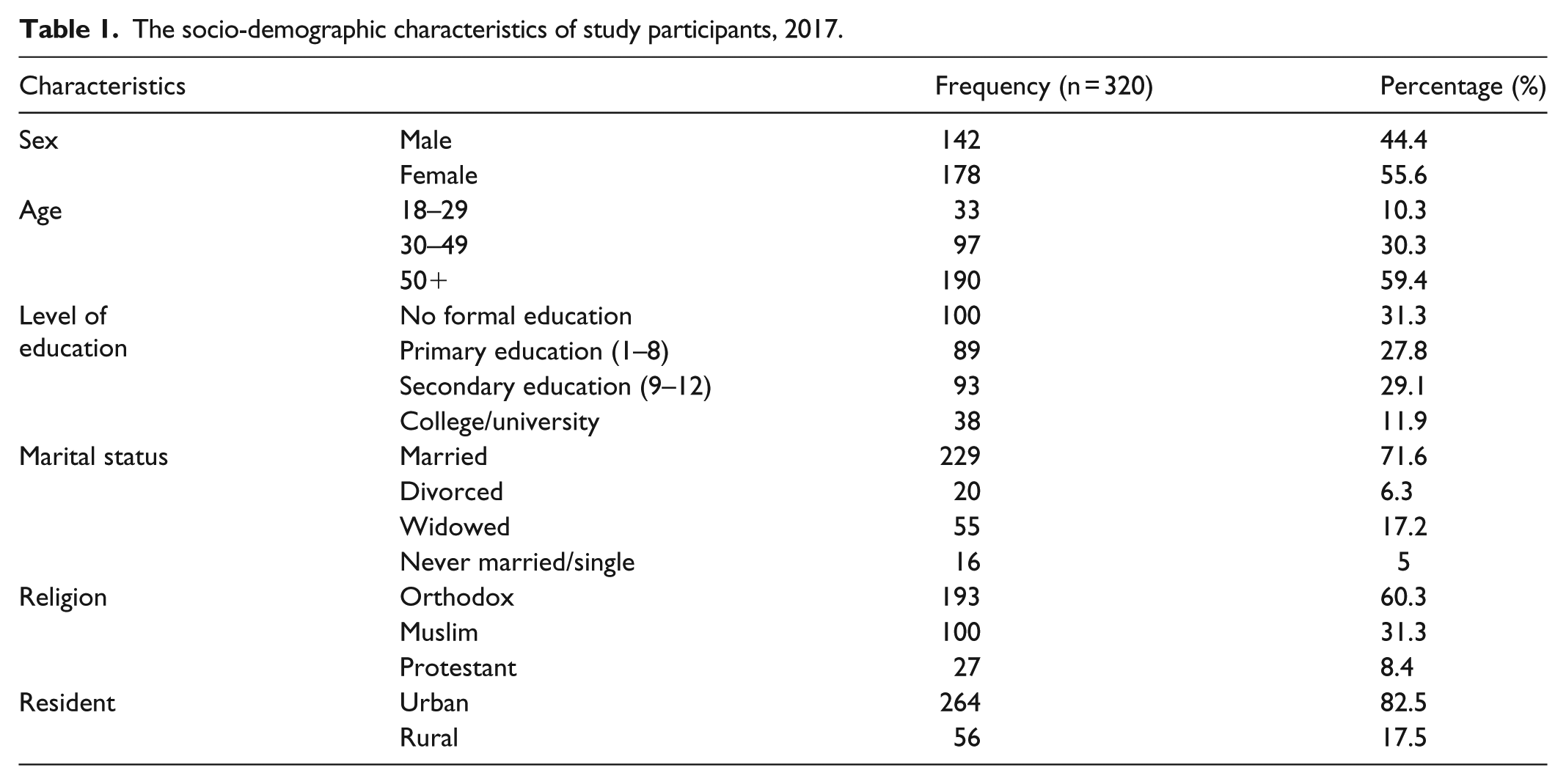
From 327 selected study participants, seven were excluded due to refusal to participate, making the response rate of 97.8%. Fifty-six percentage of the study participants were females and forty-four were males. Fifty-nine percentage of the study participants were 50 years of age or above with the mean age (±standard deviation (SD)) of 51.0 ± 15.1 years. Majority, 69.0% of the study participants attended some level of formal education (Table 1).
The socio-demographic characteristics of study participants, 2017.
Medical and behavioral characteristics
The mean number of years the study participants had been diagnosed with diabetes was 6.5 years (95% CI: 5.8, 7.2). Fifty-six percent of the study participants received oral hypoglycemic medication, while 7.0% received both oral and injectable medications. The target for blood glucose control of 70–130 mg/dL was not attained by 63.2% of the study participants. As regards to diabetic complications, 29.8% had one or more medically confirmed long-term complications (such as retinopathy, nephropathy, neuropathy, coma, hypoglycemia, foot ulcer). There was a significant association between self-care activities and DM complication (X2(df) = 34.3(4), p-value <0.001) (Tables 2 and 3).
Association of the overall DM self-care activity level with clinical characteristics of study participants, 2017.
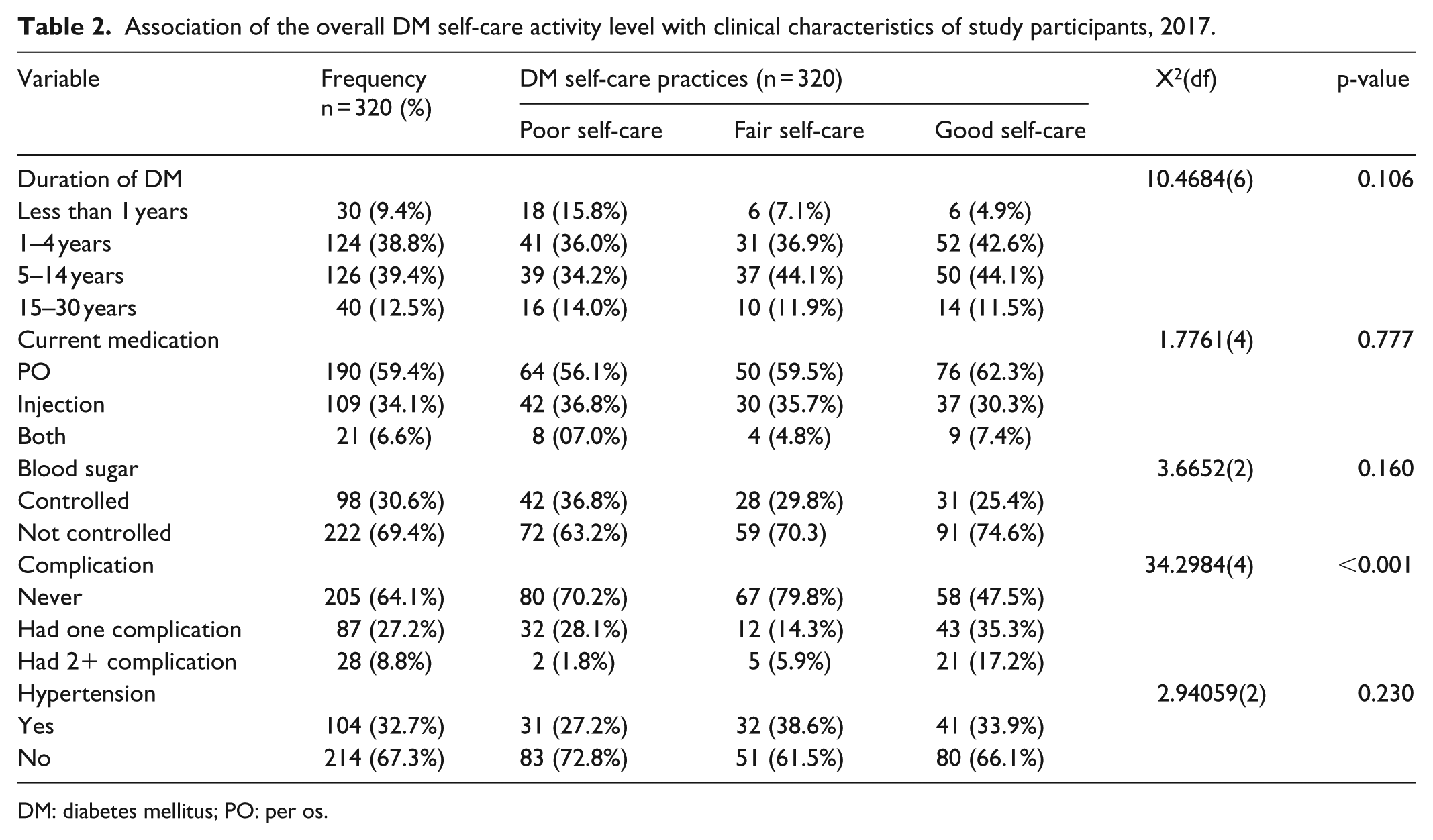
DM: diabetes mellitus; PO: per os.
Mean score of specific diabetes self-care activities among patients in diabetic follow-up clinics in Harar and Dire Dawa public hospitals, 2017.

SD: standard deviation; SE: standard error; CI: confidence interval.
Diabetic self-care activities
The overall self-care activities of the study participants were Good for 38.1% (95% CI: 32.94, 43.60), Fair for 26.3% (95% CI: 21.70, 31.37), and Poor for 35.6% (95% CI: 30.54, 41.05). The most well-attained domain-specific self-care practice was MA, where 90% (95% CI: 86.2, 92.9) of study participants took all their DM medications in the last 7 days before the survey. However, more than 50% of DM patients had Poor adherence to activities related to specific diet management, FC, and blood GM (Figure 1).

Domain-specific and the overall diabetic self-care activities of diabetes patients attending follow-up clinics in Dire Dawa and Harar public hospitals in 2017.
Factors associated with DM self-care activities
Results from the PPOM revealed that level of education, residence, blood glucose control condition, and presence of DM-related complications were significant predictors of the overall DM self-care activities (Table 4). Secondary school attendance (adjusted odds ratio (AOR) = 2.96, 95% CI: 1.51, 5.78), two or more DM complications (AOR = 4.71, 95% CI: 1.81, 12.25), and uncontrolled blood sugar level (AOR = 1.68, 95% CI: 1.02, 2.79) were positively and significantly associated with a better level of the overall DM self-care and did not differ across the outcome category. However, for a patient with only one DM-related complication, level of the overall DM self-care did not differ significantly between Poor versus any higher level of the outcome category but it differs between Poor and Fair versus Good level of the overall DM self-care (Poor vs Fair and Good, only one complication, AOR = 0.78, 95% CI: 0.44, 1.40; Poor and Fair vs Good, only one complication, AOR = 1.91 95% CI: 1.08, 3.38). DM patients who were rural residents were less likely to have either a Fair level or a Good level of the overall DM self-care activities (AOR = 0.38, 95% CI: 0.17, 0.82) with no difference on the strength of the association across the outcome category (Table 4).
Factors identified in the partial proportional odds model to have an association with diabetes self-care activities measured in three ordinal responses among patients in diabetic follow-up clinics in Harar and Dire Dawa public hospitals, 2017.
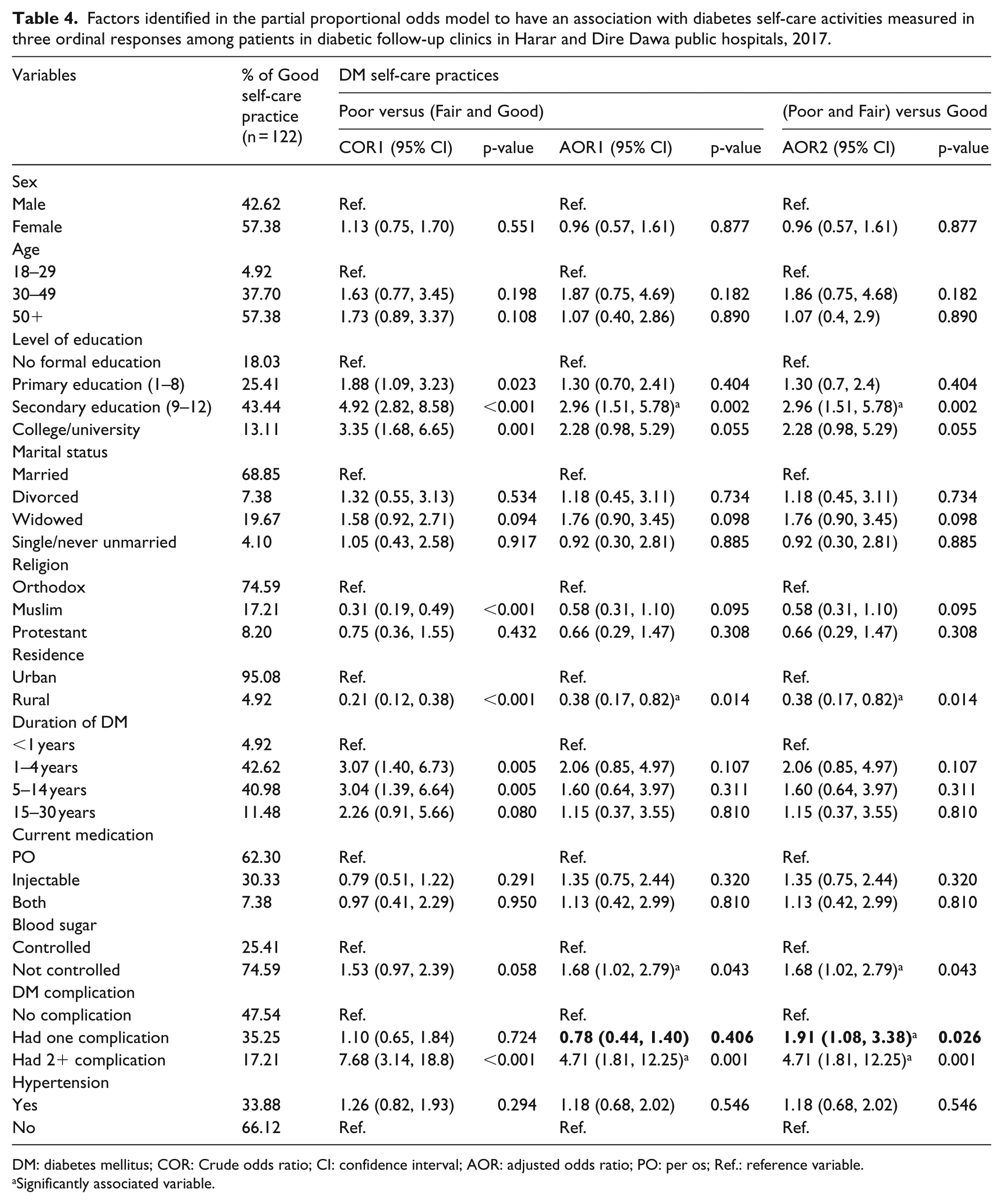
DM: diabetes mellitus; COR: Crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; PO: per os; Ref.: reference variable.
Significantly associated variable.
Discussion
Self-care activities are key components of DM care and aid in a good control of blood sugar level and reduce DM-related complications. 8 Our study measured the level of DM self-care activities and its associated factors among patients attending DM follow-up clinics. We found that only 64.4% of adult DM patients had Fair- to Good-level of the overall DM self-care activities. Covariates associated with the overall DM self-care activities include rural residence, secondary school attendance, uncontrolled blood glucose, and the presence of one or more DM complications.
A summary value of the domain-specific self-care activities (diet, PA, GM, FC, and medication) was Poor for 35.6% of participants, Fair for 26.3%, and was Good for 38.1%. Similar studies conducted in western and central Ethiopia which classified DM self-care in to Poor versus Good level, based on the mean overall DM self-care value, reported that 46% of DM patients had Poor self-care.18,30–32 However, a similar study by Abate et al. reported a higher number of Poor level self-care in Northwest Ethiopia. 13 These all four previous studies used the SDSCA tool to measure DM self-care activities.13,18,30,31 However, because they classified DM self-care level into two categories, we cannot make direct comparison as we categorized DM self-care level into three categories (Poor, Fair, and Good level) where a fair level of DM self-care in our case may be misclassified as either poor or good level of care in the case of the previous studies. Consequently, it is worth to note that Poor DM self-care was overestimated due to lack of adequate disaggregation of DM self-care level in the previous studies. We believe that by disaggregating DM self-care level into three categories, we unmasked those groups of patients that need the most attention for intervention.
The most commonly achieved domain-specific DM self-care activities in this study were MA, which is consistent with previous studies.33,34 Higher level of MA, as reported previously, could be due to the patient’s perception that taking medication is an easier way to manage their illness and essential for their survival. 34 DM patients in the current study demonstrated a poor level of monitoring their blood glucose which is also consistent with previous reports.31,34,35 However, a similar hospital-based study in India which used the SDSCA tool to measure adherence to self-care activities reported a high proportion of patients monitoring their blood sugar, 76.6%. 36 This difference could be explained by variations in the level of individual patient care that can be related to provisions of adequate information aimed at helping patients to develop enhanced self-care. Previous research findings also indicated that patients with shortage of information and had a low perceived severity of their diabetes condition had poor self-care diabetes management activities. 37 Poor domain-specific self-care practice was also common with other domains of the SDSCA in the study setting where more than 30% of DM patients did not adhere to FC, specific diet, general diet, and exercise-related practices. Previous reports indicated that Poor knowledge of DM patients and perception about the importance of self-care activities affected their level of engagement in self-care activities.38,39 For example, Chiwanga and Njelekela 40 reported that patients who received advice on FC had a significantly higher foot self-care practice.
We found that adults who attended secondary education level were more likely to practice better diabetic self-care activities compared to those who did not attend formal education. This finding was similar with studies conducted in Addis Ababa, 18 Bahir Dar, 13 South Gonder, 19 Tigray, 24 Beneshangul, 30 and Malaysia. 35 This can be related to the fact that participants with education are better informed and likely to practice acceptable standards of self-care activities than non-educated participants. In addition, Wolfe and Zuvekas identified a positive contribution of education to the efficiency of individual choice/s on health. 41 Likewise, patients with higher education have better chances to come across information about the disease and its treatment from various sources compared to uneducated patients.
This study showed that diabetic patients from rural areas were less likely to practice no higher level of self-care activities in the management of their disease. Similar findings were observed in a study conducted in Rural Sullia, Karnataka. 42 This may be related to the fact that diabetic patients in rural areas may be less literate and poorly sought help from families and friends to control their illness as suggested in other previous studies.31,43,44 Moreover, residents from rural areas have limited health services provided, limited accessibility to healthcare and less likely to accept health care compared to urban residents.45,46 Rural residents do not seek health care due to lack of awareness on the importance of seeking preventive, promotive, and curative service. 45 It is therefore inferred that emphasis should be given to assisting and providing follow-up and health services to DM patients from rural areas.
Adult diabetic patients with uncontrolled blood sugar level were more likely to practice a fair or a good level of care compared to those who had controlled blood sugar level. Patient’s self-care behavior determines improvement in blood glucose status. 47 Consequently, we hypothesize that a better self-care activity among DM patients with uncontrolled blood glucose could be due to the patient’s determination to practice better self-care behavior. Furthermore, a healthcare provider may give more emphasis to improve the health outcome of a patient with an unfavorable outcome which could influence the health-related behavior of a patient. We also argue that as behavior is mediated by cognition, 48 patient’s knowledge about his or her blood sugar control status and attitude about health outcome of adherence to a healthy behavior may influence the action toward good self-care.
Patients with DM who had one or more complications were more likely to practice and adopt Good diabetes management self-care activities compared to those without any complication in the current study. This study revealed that patients with diabetic complications managed their illness better by seeking help from their families and they adhered more to the instructions given by their physician. On the contrary, patients who have no complications may not worry much to adhere to self-care practices. Our finding on the association between DM complications and self-care is consistent with the findings reported in a study in Malaysia. 49 Diabetic patients with low diabetes complication risk perception may also have a lower level of DM self-care among those who had no complications. 50 Therefore, this study suggests that diabetic patients without complication should be targeted to improve self-care practice in order to avoid poor treatment outcomes.
Strengths of the study
The strength of this study includes the use of a standard validated tool to assess SDSCA which aided our results to be comparable due to consistency of measurements. Furthermore, the use of a robust PPOM helped us to analyze the dependent outcome variable disaggregated and graded into different categories despite violations of the proportional odds assumption. The disaggregation of the outcome variable helped us to look into the gradient of self-care practice.
Limitations of the study
While sharing the methodological limitation of cross-sectional studies, there may be a recall and social desirability biases as the self-care activities were measured based on self-reports and performance of these behaviors was not observed activities and cannot be confirmed.
Conclusion
The findings of the current study showed that only one-third of the study participants practiced a good level of DM self-care activities. Healthcare providers in the study setting should focus on diabetic patients who are less likely to demonstrate self-care activities in managing their illness, in particular adult patients with low education living in rural areas. Strategies for individualized and mass education should be well established with related support to ensure that diabetic patients develop good level of understanding to effectively practice self-care activities. It is vital to mention here that healthcare providers should teach key self-care activities to DM patients. They need to develop a practical patient learning plan where patients can share their experiences, ask questions and receive approval when able to demonstrate what they have learned in self-care management of DM. Since this study did not assess health facility-related factors or strategies that can potentially improve patient self-care practices, future studies should consider the above to develop a comprehensive intervention for patients to improve their diabetes management self-care practices.
Supplemental Material
DM_questionnaries_1 – Supplemental material for Predictors of self-care activities of outpatient diabetic residents in Harar and Dire Dawa: A hospital-based cross-sectional study
Supplemental material, DM_questionnaries_1 for Predictors of self-care activities of outpatient diabetic residents in Harar and Dire Dawa: A hospital-based cross-sectional study by Behailu Hawulte Ayele, Melkamu Merid Mengesha and Tewodros Tesfa in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Haramaya University for providing financial and administrative support for this study. Also, we would like to extend our gratitude to Dire Dawa City Administration Health Bureau and the staffs of public hospitals in Dire Dawa and Harar. More importantly, we would like to thank the data collectors, supervisors, and study participants who made this research study possible. Last, but not least, the authors appreciate Carmencita Alcantra for editing the paper.
Author contributions
B.H.A. made substantial contributions from conception of the research idea to proposal development, data collection, data management, analysis and interpretation of data, including preparation of the manuscript. M.M.M. equally engaged in conception of the research idea to proposal development, data collection, data management, analysis and interpretation of data, and preparation of the manuscript. T.T. participated in proposal development, data collection, data management, and preparation of the manuscript for publication. All authors read and approved the final version of this manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Haramaya University College of Health and Medical Sciences Institutional Health Research and Ethical Review Committee (IHRERC) with reference no. of IHRERC/116/2017. To obtain permission of the participating institutions, an official letter was sent to Hiwot Fana Specialized University Hospital, Jugal General hospitals, Dilchora General Hospital, and Sabian Primary Hospital. Personal identifiers were not included in the questionnaire to maintain confidentiality.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Haramaya University covered the cost of field activities (data collection), with the funding code HURG-2016-02-01-11. This funding institution did not have a role in study design, data collection and analysis, interpretation of data, decision to publish, or preparation of the manuscript.
Informed consent
The objectives of the study were explained to each study participants. Those volunteer and signed on the consent form was involved in the study. Written informed consent was obtained from all study participants before the study.
Supplemental material
Supplemental material (questionnaire) for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.