
Abstract
Objectives:
Our study aimed to identify the complex interplay between self-efficacy, self-care practice, and glycaemic control among people with type 2 diabetes mellitus (PWDs) to inform the design of more targeted and effective behavioural interventions in primary care.
Methods:
A cross-sectional descriptive study was performed with 294 PWDs managed in primary care. The Diabetes Management Self-Efficacy Scale (DMSES) and Summary of Diabetes Self-Care Activities (SDSCA) questionnaire measured patients’ self-efficacy and self-care practice. Multivariate logistic regression models were developed to explore how SDSCA, DMSES, and their combined effect relate to glycaemic control, adjusting for patient characteristics. Network analysis in R software examined relationships between self-efficacy and self-care dimensions across glycaemic control subgroups using a Gaussian graphical model with the extended Bayesian information criterion.
Results:
Half the PWDs (50.7%) had suboptimal glycaemic control. Better glycaemic control was consistently associated with higher self-efficacy (odds ratio (OR) = 0.76, 95% confidence (CI) (0.60, 0.97), p = 0.03), shorter duration of diabetes (OR = 1.89, 95% CI (1.08, 3.31), p = 0.03), normal waist circumference (OR = 1.76, 95% CI (1.02, 3.05), p = 0.04), absence of diabetes complications (OR = 2.09, 95% CI (1.10, 3.98), p = 0.02), and treatment with oral hypoglycaemic agents (OR = 3.05, 95% CI (1.53, 6.09), p < 0.01). Network analysis among people with well-controlled HbA1c revealed that diet adherence and self-efficacy had the most robust connection, with diet self-efficacy strongly associated with most self-efficacy dimensions. Self-efficacy in exercise, blood glucose monitoring, and foot care are the most central factors in the network structures for PWDs with suboptimal glycaemic control.
Conclusions:
Our study highlights the critical role of self-efficacy in diabetes primary care. For people with optimal glycaemic control, prioritising self-efficacy in diet adherence is crucial for sustaining glycaemic outcomes and supporting other self-care behaviours. Among those with suboptimal glycaemic control, enhancing self-efficacy in exercise, blood glucose monitoring, and foot care is essential. Targeted education programs, personalised counselling, and E-health tools can further empower patients to manage their diabetes more effectively.
Introduction
Type 2 diabetes mellitus (T2DM) has been becoming a major global health condition, especially in low- and middle-income countries. In Vietnam, the percentage of diagnosed people with type 2 diabetes mellitus (PWDs) was 2.7%, 5.4%, and 6.1% in 2002, 2012, and 2021, respectively; it is predicted to reach 7.1% in 2045.1,2 While achieving optimal glycaemic control is a primary target to delay the onset of diabetes complications and improve the quality of life for PWDs, over 60% of PWDs in Vietnam have poor glycaemic control.3,4 This higher-than-expected rise in prevalence and inadequate control of T2DM considerably impact the performance of health systems for diabetes care.
Vietnamese healthcare delivery is distributed into four levels: commune, district, provincial, and central (Figure 1). Although efforts by the Ministry of Health to shift chronic care from hospitals to primary healthcare (PHC),5,6 the response of PHC to non-communicable diseases remains insufficient. Only 53% of commune health centres (CHCs) offer T2DM services. 7 Due to inadequate workforce capacity and lack of resources at CHCs, 8 the diagnosis and initial treatment of T2DM are typically decided at the district-level and upper-level facilities, after which stable patients are referred to their CHCs for follow-up and management. Empowering PWDs and fostering collaborative care, where they are fully engaged in managing their illness condition, are the keys to an effective paradigm shift in diabetes care.9,10

Structure, class categorisation, and functions of different levels in diabetes care within the Vietnamese public healthcare system. 11
Self-efficacy and self-care practices are crucial components of the chronic care model for maintaining optimal glycaemic control. 12 Diabetes self-care refers to various day-to-day activities to optimise disease control, such as eating a healthy diet, physical exercise, medication adherence, blood glucose self-monitoring (if indicated), and foot care. 13 Perceived self-efficacy is a person’s confidence and belief in their ability to perform these specific self-care activities. The relationship between self-efficacy and self-care is considered a loop, where high self-efficacy activates patients to engage in better self-care behaviours, and successful self-care practices also boost self-efficacy, creating a dynamic cycle for optimising diabetes management.14,15 Research has consistently shown that individuals with solid self-efficacy and self-care skills tend to achieve better glycaemic control, as evidenced by lower HbA1c levels.15 –17 Unfortunately, many people with chronic illnesses lack the adequate skills and self-efficacy to manage their conditions effectively.18,19 Thus, there has been a growing number of diabetes self-management support (DSMS) programs worldwide, including in the Asia Pacific region, which have shown positive effects on glycaemic control and overall diabetes care. 20 However, there is still a significant gap in the literature on how psychological and behavioural factors interplay and contribute to optimal glycaemic control and the design of effective DSMS interventions.
Given the multifaceted nature of diabetes self-efficacy and self-care practice, the relationship and interactions among different dimensions of self-care and self-efficacy concepts may be usefully framed as a network of factors contributing to glycaemic control. The network analytic method allows us to identify the dynamics and interconnections among different dimensions of self-efficacy and self-care practice. By mapping this network, we can determine which behaviours or beliefs are most central and impactful to glycaemic control, thereby enabling the development of more targeted and effective DSMS. Due to insufficient evidence, our study aims to (1) examine the association between self-efficacy, self-care behaviours, and glycaemic control and (2) identify the specific dimensions of self-efficacy and self-care behaviours that significantly impact glycaemic control through network analysis. Results from this study may direct the primary care providers and policymakers to develop tailored DSMS programs for primary care, leading to more effective, evidence-based strategies for promoting self-care and improving diabetes care.
Methods
Study design and population
A cross-sectional descriptive study was conducted in Thua Thien Hue province (Central Vietnam) from 20 October 2021 to 28 January 2022. Data collection and interviews occurred between 1 November 2021 and 28 January 2022, during the “new-normal” period of effective COVID-19 control in Vietnam. During this time, the Ministry of Health adjusted healthcare provisions, allowing prescriptions for chronic patients to extend up to 3 months, compared to the usual monthly refills, which led to a longer duration between follow-up appointments. Importantly, Thua Thien Hue province remained COVID-19-free throughout 2020–2021, ensuring that the pandemic did not directly affect the data collection and face-to-face interviews.
The minimum sample size of 302 participants was estimated using a ratio estimation, with a 95% confidence interval (CI), a marginal error (d) of 0.1, a design coefficient (DEFF) of 3, anticipated adequate self-efficacy proportion of 52.5% (based on a previous study 19 ), and a 5% refusal rate. We employed a two-stage sampling method to ensure representation of both rural and urban populations. First, we randomly selected one rural district (Phu Vang district) and one urban district (Hue City) from the nine districts in the province using a simple random sampling technique. Two primary care clinics within these districts were identified for participant recruitment. Inclusion criteria for participants were: (1) individuals with T2DM aged between 18 and 80 years, (2) diagnosed with T2DM for at least 1 year to ensure established self-efficacy and self-care routines, and (3) having scheduled medical follow-ups during the study period. Individuals with cognitive impairments, mental disorders, or conditions affecting communication and daily lifestyle behaviours were excluded. From the electronic medical records, we identified 318 eligible participants with T2DM. Of these, 294 completed the survey during their routine clinic visits, representing a response rate of 92.5%. All participants provided written informed consent before participating.
Measurements
Participants who agreed to participate were interviewed face-to-face within their routine medical encounters with a structured questionnaire by trained research assistants. Each interview took approximately 30 min. Demographics, health conditions, medical history, and diabetic characteristics were collected from the patient booklets. Weight, height, waist–hip circumferences, and blood pressure were measured in the interview. The most recent HbA1c levels of patients, measured either at the time of data collection or no more than 3 months prior, were obtained from the electronic medical record (EMR) database. With the patients’ consent, researchers accessed the EMR daily during the data collection, based on the patient encounter ID; data were anonymised before analysis to ensure participant confidentiality. Adults with HbA1c < 7% and older people (aged ⩾ 60 years) with HbA1c < 7.5% were defined as having well-controlled or optimal glycaemic control. 21 Conversely, individuals with HbA1c levels equal to or greater than these thresholds were classified as having suboptimal glycaemic control. We also employed the EuroQOL-5 Dimensions-5 Levels (EQ-5D-5L) to measure the health-related quality of life index, which has been validated for the Vietnamese population with a score range of −0.5115 to 1.22. 22
The Summary of Diabetes Self-Care Activities (SDSCA; Supplemental material) instrument is widely used to assess diabetes self-care (DSC) among PWDs and has been translated into different languages, including Vietnamese. The SDSCA has shown sufficient internal and test-retest reliability. 23 This self-report instrument includes ten core items to assess four aspects of the diabetes regimen: diet, exercise, self-monitoring of blood glucose (SMBG), and foot care. It also contains one question on smoking behaviour and 14 optional items to address specific self-care behaviours, such as medication use. 23 For this study, we used the ten core questions and two specific questions on medication adherence, excluding the smoking question. Smoking behaviour was assessed separately as a demographic factor, as previous studies assessing self-care behaviours using SDSCA did not report smoking as a self-care behaviour. The Vietnamese version of this instrument was validated through forward and backward translation, testing, and expert panel reviews by supervisors and primary care professionals to ensure its accuracy and cultural relevance. It was piloted with 30 PWDs before the field survey. This final version included 12 items covering five DSC dimensions: diet (4 items), physical activity (2 items), SMBG (2 items), medication adherence (2 items), and foot care (2 items). Answers were recorded on a scale from 0 to 7, indicating how many days in the past week participants practised DSC. The score was inverted for the item related to consuming fat-rich foods. For PWDs who did not have any diabetes treatment or followed diet and exercise therapy only, the items of medication adherence were not used to calculate the overall DSC. Depending on the treatment, we used only 1 item of medication adherence to calculate overall DSC for PWDs having oral medication or injection. The item scores were averaged, resulting in an overall score of DSC ranging from 0 to 7.
The Diabetes Management Self-Efficacy Scale (DMSES; Supplemental material), comprising 20 items, was used to measure participant’s confidence in managing various aspects of diabetes care, including following a healthy diet (9 items), blood sugar monitoring (3 items), foot care (1 item), physical activity practice (4 items), and medication adherence (3 items). 24 The scale was originally developed by Bijl et al. 24 in the Netherlands and has been validated across multiple settings, including Australia, Belgium, Switzerland, the UK, and the USA, through the work of the International Partners in Self-Management and Empowerment (IPSE). 25 While Sturt et al. 26 revised the DMSES to a 15-item version for use in the UK, the original 20-item version remains widely used and has demonstrated reliability and validity in numerous countries, including several Asian contexts such as Taiwan, 27 Thailand, 17 and Korea. 28 In Vietnam, a previous study validated this version, demonstrating high internal consistency with an overall Cronbach’s alpha of 0.91 and domain-specific alphas ranging from 0.71 to 0.92. 29 In this instrument, participants rated themselves on an 11-point scale, where ‘zero’ indicated ‘cannot do at all’ and ‘10’ indicated ‘certainly can do’.27,29 To calculate the mean self-efficacy score, sum all item scores and divide by 20. Scores range from 0 to 10, with higher scores indicating greater self-efficacy.
Statistical analysis
The data entry and preliminary analyses were performed using Epidata 3.1 (EpiData Association, Odense, Denmark) and SPSS 22.0 software (IBM Corp., Armonk, New York, USA). Descriptive statistics were calculated, and bivariable analyses were initially conducted using Chi-square tests and independent-sample t-tests to examine relationships between the variables. Multivariate logistic regression analysis was applied to identify factors associated with glycaemic control among PWDs. Variables were included in the multivariate models if they had a p-value less than 0.2 in bivariable analysis or were previously identified as predictors of glycaemic control in the literature.4,15,30 To explore the relationship between diabetes self-care behaviours, self-efficacy, and glycaemic control, we developed three multivariate models: (1) Model 1 – Effect of self-care practices (SDSCA) on glycaemic control, adjusted for patient characteristics; (2) Model 2 – DMSES on glycaemic control, adjusted for patient characteristics; (3) Model 3 – Combined effect of SDSCA and DMSES on glycaemic control, adjusted for patient characteristics. A p-value of <0.05 was considered statistically significant.
The analyses for network structure were performed using RStudio (2021. 9. 2; RStudio, Boston, MA, USA) and R ver. 4.1.2 (The R Foundation for Statistical Computing). Several packages were used to perform the analyses, including q-graph (ver. 1.9.2; https://www.rdocumentation.org/packages/qgraph/versions/1.9.2) for network estimation and plotting, bootnet (ver. 1.5, The R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/) for network accuracy and stability analysis, and network comparison test (NCT, Version: 2.2.1) for comparison of the differences between networks. The network structure of self-care and self-efficacy domains was examined using a Gaussian graphical model with regularisation through the graphical lasso algorithm, applying the extended Bayesian information criterion (tuning parameter = 0.5). A correlation stability coefficient greater than 0.25 indicated stable node centrality indices. Bootstrapped 95% CI of edge weights were calculated to analyse the accuracy and stability of the network. We utilised three centrality indices to describe the network: strength, betweenness, and closeness. Strength reflects a node’s direct connections, revealing the most impactful self-care and self-efficacy behaviours; betweenness indicates a node’s role as a connector, showing which behaviours facilitate overall network interactions; and closeness measures the shortest edges to other nodes, highlighting behaviours that indirectly influence the network. Network characteristics such as network density, global strength, average clustering coefficient, modularity index (Q), and average shortest path length were described.
Results
Socio-demographic and clinical characteristics of participants
Table 1 provides the characteristics of the study population stratified by glycaemic control status. The average age of the participants was 64.02 (SD 10.68 years). Most participants were female, living in urban areas, and had a primary education qualification. Approximately half of the participants had suboptimal glycaemic control (50.7%), 52.2% living in urban and 48.2% in rural areas. Over two-thirds of participants had concurrent hypertension. The overall scores of participants on self-care practice and self-efficacy were low, with mean scores of 3.97 (SD 0.91) and 6.84 (SD 1.35), respectively. People with T2DM for a longer duration, having insulin in their treatment, and complication presence exhibited poorer glycaemic control than others (p < 0.05). Participants with uncontrolled HbA1c levels had slightly higher mean scores for both overall self-care of diabetes (4.05) and self-management efficacy (7.01) compared to those with controlled HbA1c levels (3.88 and 6.66, respectively).
Demographic and clinical characteristics of respondents by glycaemic control status.
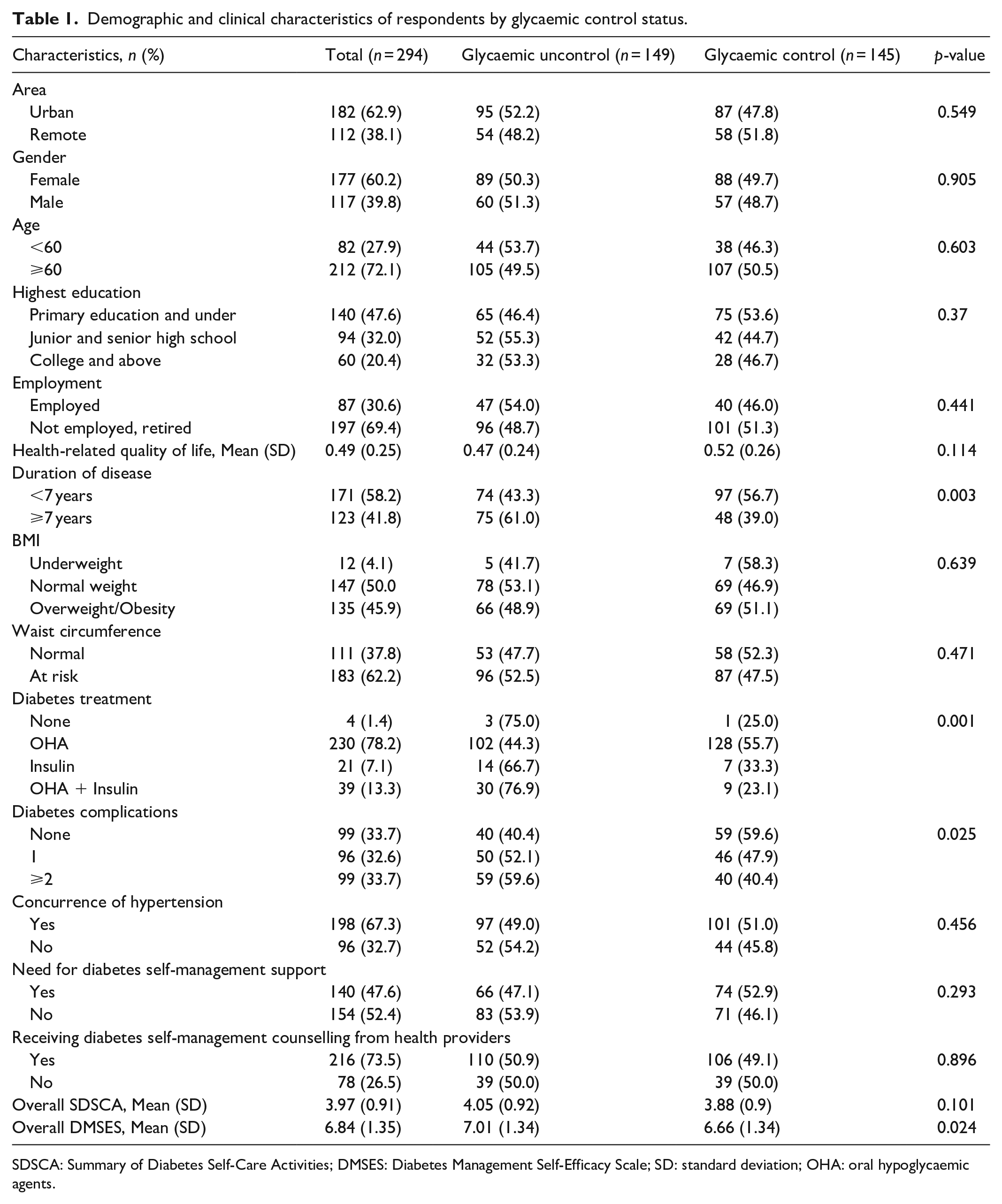
SDSCA: Summary of Diabetes Self-Care Activities; DMSES: Diabetes Management Self-Efficacy Scale; SD: standard deviation; OHA: oral hypoglycaemic agents.
Factors associated with glycaemic control: Multivariate logistic regression models
Table 2 demonstrates the multivariate logistic regression analysis of HbA1c control as the dependent variable with self-care practice, self-efficacy, and selected participants’ characteristics as independent variables. The association between diabetes management self-efficacy and glycaemic control was consistent when adjusting for diabetes self-care practices. Higher self-efficacy was significantly associated with lower odds of having suboptimal glycaemic control (Model 2: OR = 0.8, 95% CI (0.65, 0.99); Model 3: OR = 0.76, 95% CI (0.6, 0.97); p < 0.05). Meanwhile, higher self-care practices were related to lower odds of suboptimal glycaemic control (OR = 0.94, 95% CI (0.7, 1.26)) without considering self-efficacy, but higher odds (OR = 1.15, 95% CI (0.81, 1.63)) when taking self-efficacy into account. However, neither association was statistically significant. Across all three models, a normal waist circumference (p < 0.05), shorter T2DM duration (p < 0.05), absence of diabetes complication (p < 0.05), and oral hypoglycaemic agent (OHA) treatment (p < 0.01) were strongly associated with better glycaemic control among participants.
Multivariate logistic regression models of glycaemic control, self-efficacy, self-care, and participant characteristics.

Model 1: Effect of diabetes self-care practices (SDSCA) on glycaemic control, adjusted for patient characteristics.
Model 2: Effect of diabetes management self-efficacy (DMSES) on glycaemic control, adjusted for patient characteristics.
Model 3: Combined effect of SDSCA and DMSES on glycaemic control, adjusted for patient characteristics.
Patient characteristics included in all three models were age, employment status, health-related quality of life, waist circumference, diabetes duration, complications, hypertension concurrence, treatment regimen, and diabetes self-management support needs.
OR: odds ratios; 95% CI: 95% confidence intervals; OHA: oral hypoglycaemic agents; and p-values for SDSCA, DMSES, and patient characteristics were reported.
1: reference group.
Significance levels: *p < 0.05; **p < 0.01.
Network analysis of diabetes self-efficacy and self-care practices on glycaemic control
Figure 2 illustrates the relationships between different domains of SDSCA and DMSES among participants. Seven edges were identified in the total sample network (Figure 2A), with three edges showing a partial correlation (pc) greater than 0.3. The most robust connection was observed between foot care practice and self-efficacy (0.58), followed by exercise adherence and confidence (0.54) and diet adherence and self-efficacy (0.48). Figure 2B shows that exercise self-efficacy exhibited the central role with the highest nodal strength in the overall network. The closeness centrality plot showed that medication adherence had minimal or no direct or indirect connections to other nodes in the overall network.

Network structure (A) and centrality indices (B) of the total sample.
Figure 3 demonstrates the relationships among different dimensions of diabetes self-care practice and self-efficacy for individuals with good and poor glycaemic control. Among people with well-controlled HbA1c levels (Figure 3A), the strongest correlation was observed between diet adherence and confidence (weight: 0.63), followed by foot care practice and confidence (weight: 0.52) and exercise adherence and confidence (weight: 0.43). We also found moderate interconnections between diet-related self-efficacy and other domains, indicating its critical role in enhancing self-efficacy across domains to achieve optimal glycaemic control. For people with suboptimal glycaemic control (Figure 3B), the strongest correlation was observed between foot care practices and self-efficacy (weight: 0.63), followed by exercise practices and self-efficacy (weight: 0.61). Moreover, there were moderate interconnections of blood glucose monitoring self-efficacy and other self-efficacy domains, including diet (with a weight of 0.26) and exercise (with a weight of 0.18). These connections suggest that improvements or challenges in one area can influence the others.

Network structures for optimal glycaemic control (A) and suboptimal glycaemic control (B).
In the combined network of SDSCA and DMSES dimensions, self-efficacy dimensions were more central across different glycaemic control levels than SDSCA dimensions (Figure 4). For SDSCA dimensions, foot care practice had the highest nodal strength among those with poor glycaemic control, followed by exercise and diet practice. For DMSES dimensions, self-efficacy for exercise and blood glucose monitoring were the most dominant factors among those with poor glycaemic control. The change in nodal strength was most remarkable for self-efficacy in diet and blood glucose monitoring.

Nodal strength centrality indices for glycaemic control.
Discussion
Glycaemic control is critical for effective diabetes treatment and its complication management. Our study reveals a relatively high proportion of PWDs having suboptimal glycaemic control, similar to studies in Central Vietnam (48.1%), 31 Maldives (50.7%), 32 and Thailand (54.8%). 33 However, this is lower than the findings from Vietnam in 2015 (63.9%) 3 and China in 2020 (65%). 34 These variations could be attributable to different glycaemic control criteria, as these studies used the HbA1c cutoffs of <7% or <6.5% for the entire population without considering older adults specifically. The local situation of the COVID-19 pandemic and policies for rescheduling chronic care appointments may also affect these differences. Since our focus was on primary care, where patients typically have stable diabetes, our findings differ from hospital-based studies with more complex cases.
Self-care practices and management self-efficacy observed in our study participants were lower than those reported in the previous studies. The score of SDSCA was lower than that reported in Thailand 17 (4.8, SD 1.73) and India 35 (4.56, SD 2.61) during the COVID-19 pandemic. Similarly, the DMSES score found in Malaysia 15 was 7.33 (SD 2.25), and in Iran, 36 it was 7.31 (SD 1.14), compared to our study score of 6.84 (SD 1.35). Besides the cultural differences and the impact of COVID-19, these findings suggest potential gaps in effective DSMS in primary care. A systematic review in the Asian Western Pacific region indicates that group-based diabetes self-management education and support (DSMES) with hands-on sessions delivered by multidisciplinary teams improve self-management and glycaemic control. 20 Interventions focused on self-efficacy have successfully improved self-efficacy and self-management behaviours, which are essential for better glycaemic control. 37 However, little is known about DSMES implementation in Vietnam. It is strongly recommended to enhance the availability and accessibility of culturally appropriate DSMES programs in primary care to improve self-care practices and self-efficacy in managing diabetes.
Our study found a consistent association between diabetes self-efficacy and glycaemic control, aligning well with Bandura’s self-efficacy theory 38 and previous studies.15 –17 These findings collectively suggest that individuals with strong self-efficacy are more likely to engage in and maintain necessary behaviours to achieve their goals. Although the positive association between self-care practice and glycaemic control is well-documented in the literature,30,35,39,40 our study did not observe this association.41,42 Diabetes self-care behaviours are complex and require different aspects to adhere to and maintain, with motivation being a key. However, the COVID-19 pandemic disrupted many aspects of daily life, including access to healthcare, social support, and physical activity, which can negatively impact motivation and self-care behaviours.35,43 Additionally, data collection occurred during a period of numerous celebrations before the Vietnamese Lunar New Year, potentially leading to overconfidence in managing their illness without proper self-care practices. Our study highlights the need for tailored interventions to tackle the specific challenges of managing chronic conditions during festive periods and public health crises. It informs strategies for healthcare systems to better prepare for and respond to similar situations in the future. Furthermore, future studies should incorporate psychological factors to understand diabetes management better during such challenging times.
The relationships between DSC, DMSES, and glycaemic control are clearly complex and potentially influenced by various patient characteristics. Notably, our study revealed significant effects of waist circumference, diabetes duration, treatment regimen, and complications on glycaemic control, reinforcing findings from previous studies.4,30,35,44 These findings emphasise the importance of considering a patient’s specific health profile when designing and evaluating the effectiveness of DSMES on health outcomes. Patients with shorter diabetes duration or those on an OHA regimen showed significantly higher optimal glycaemic control rates than others.17,45,46 This highlights the need for additional support and resources as diabetes progresses and treatment becomes more complex to help patients maintain effective self-care and control over their condition. Similarly, previous studies found that suboptimal glycaemic control was likely observed in patients with a high risk of abdominal obesity.47,48 These findings support the importance of monitoring and maintaining a healthy waist circumference through diet and exercise to improve insulin sensitivity and optimum glycaemic control.
However, in our study, neither the need for DSM support nor reported receipt of DSM counselling was significantly associated with glycaemic control. This may indicate that while DSM support and counselling are beneficial, their impact on glycaemic control might depend more on the specific quality, consistency, and individualisation of the support rather than just access or need alone. Bandura’s self-efficacy theory identifies four primary sources of self-efficacy: mastery experiences, vicarious learning, social encouragement, and managing emotional and physical responses. 38 Mastery experiences are the most influential as they reinforce an individual's confidence through successful experiences. Building on this, practical interventions in primary care settings can focus on providing personalised, hands-on counselling during routine care and setting achievable self-management goals to allow patients to build confidence through small successes. Peer support groups enable patients to learn from others' stories, while healthcare providers can reinforce progress through motivational interviewing. Additionally, psychosocial support, such as cognitive-behavioural therapy or stress management coaching, can further support patients’ ongoing self-care and glycaemic control efforts.
As far as we know, our study is the first effort using network analysis to explore the relationships between diabetes self-care, management self-efficacy dimensions, and the strength of the impact of these factors on glycaemic control. Our findings provide a comprehensive visualisation of the interactions between various self-care practices and self-efficacy domains rather than simply identifying individual factors associated with glycaemic control. This approach offers valuable insights to inform more effective and practical self-efficacy-focused education and self-management interventions at the grassroots level. Our findings indicate that self-efficacy for foot care, exercise, and diet showed the strongest connections to self-care adherence. This result highlights the importance of regular foot care, physical activity, and diet in diabetes management to improve patient outcomes. Similar to Rucci et al., 49 we found that medication self-efficacy was isolated and disconnected from confidence in managing daily lifestyles. This disconnection suggests the need for focused interventions and tools addressing medication adherence independently from other self-care behaviours rather than being a part of a broader self-management support strategy. Healthcare providers should offer targeted education sessions or personalised counselling or integrate medication reminder applications such as mobile health and short message service (SMS) reminders, specifically focused on medication adherence and tracking.
In our study, diet adherence and confidence showed the strongest correlation among people with well-controlled HbA1c levels. According to our results and literature, 49 diet self-efficacy is interconnected with other self-efficacy domains, indicating that dietary habits play a crucial role in diabetes self-management. This, in turn, promotes individuals to engage in additional self-care behaviours. Comprehensive diabetes education programs should emphasise and begin with diabetes-specific nutrition supplements first to build a vital cornerstone for overall self-efficacy and self-care practice. Network meta-analysis results of Schwingshackl et al. 50 showed that low-carbohydrate and Mediterranean dietary approaches were highly efficacious in improving glycaemic control in T2DM patients. In Vietnam, healthcare providers should provide adequate knowledge of the nutritional composition of healthy foods and low-carbohydrate alternatives, encourage changes in shared dish habits, and call for family support to facilitate these dietary changes. Moreover, an integrated mobile application targeting educational materials and resources to self-monitor diet diaries, carbohydrate counters, exercise, and blood glucose level trends is promising to improve diabetes self-management. 51
Conversely, for those with suboptimal glycaemic control, foot care practice and self-efficacy were most strongly associated, with foot care practice having the highest nodal strength among self-care behaviours. The lack of awareness and practice of patients and healthcare providers on foot care in diabetes management has been acknowledged in the literature.52 –54 Therefore, it is strongly recommended that awareness be raised among patients and healthcare providers about the importance of integrating self-management practices, such as foot care, into routine care for T2DM, particularly for those struggling to maintain glycaemic control. Furthermore, the highest nodal strength for self-efficacy in exercise and blood glucose monitoring among DMSES dimensions highlighted their most dominant factors contributing to poor glycaemic control. Significantly, regular blood glucose monitoring is crucial for effective diabetes management, as it assists PWDs in better awareness of their glycaemic condition and timely adjustments in diet, exercise, and medication. Although guidelines for self-monitoring of blood glucose in routine care are inconclusive for those not on insulin, the marked difference in self-efficacy for blood glucose monitoring between glycaemic control subgroups in our study underscores its importance in diabetes management.
Moreover, within the digital health era, leveraging e-health tools presents an opportunity to provide continuous support beyond clinical visits. SMS, mobile health apps, and remote patient monitoring systems can provide accessible and cost-effective strategies to reinforce self-management behaviours, particularly for patients in remote areas. Digital health interventions have shown promise for lowering HbA1c levels and enhancing diabetes care, with evidence suggesting that an optimal intervention duration is 6 months or less. 55
There are several limitations to the current study. Since it is a cross-sectional descriptive study, causality cannot be established between self-efficacy, self-care practices, and glycaemic control. Additionally, the reliance on self-reported measures for assessing diabetes self-efficacy and self-care practices may introduce recall bias and potential overestimation, especially regarding perceived self-efficacy. The data collection occurred during the COVID-19 pandemic, leading to changes in healthcare delivery and patient behaviours, potentially affecting study results. Moreover, our study could not reach individuals who did not attend follow-up appointments, potentially introducing selection bias towards more engaged patients and limiting generalisability to those less active in their care. Some essential aspects of diabetes management, such as diabetes-related literacy, social and family support, and psychological issues, were not considered. Conducting a longitudinal study and overcoming these limitations would provide a deeper understanding of the causal relationships between self-care practices, self-efficacy, and glycaemic control over time. Additionally, exploring the influence of cultural factors on self-efficacy and self-care behaviours in diabetes management could provide richer insights for designing effective self-management interventions that align with cultural norms and values in Vietnam and similar settings.
Conclusions
Our study highlights the complex interplay between management self-efficacy, self-care, and glycaemic control in diabetes management in primary care. Dietary self-efficacy is central in reinforcing other self-care practices among individuals with well-controlled glycaemic levels. In contrast, self-efficacy in exercise, blood glucose monitoring, and foot care appear to be the most influential factors contributing to suboptimal glycaemic control. Targeted education programs, personalised counselling to address specific self-care needs, behavioural interventions focused on diet, foot care, and physical activity, and leveraging technology that enhances confidence in specific self-care activities are needed to support sustained self-management. These targeted approaches can improve patient confidence and foster better glycaemic outcomes, particularly in primary care settings.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241310016 – Supplemental material for Exploring the relationships between self-efficacy, self-care, and glycaemic control in primary care diabetes management
Supplemental material, sj-docx-1-smo-10.1177_20503121241310016 for Exploring the relationships between self-efficacy, self-care, and glycaemic control in primary care diabetes management by Le Ho Thi Quynh Anh, Nguyen Vu Quoc Huy, Nguyen Minh Tam, Johan Wens, Anselme Derese, Wim Peersman, Vo Ngoc Ha My, Tran Binh Thang, Nguyen Thi Phuong Anh, Tran Thi Truc Ly and Peter Pype in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to extend our thanks to the respondents, local health providers, and research team members who supported us in collecting the data, as well as all of the staff in the Family Medicine Centre, Hue University of Medicine and Pharmacy, Hue University for their support throughout this work. We also thank the VLIR Inter-University Cooperation Program with Hue University for their financial support of this study.
Author contributions
All authors contributed to the study conceptualisation and methodology. Data collection was done by Le Ho Thi Quynh Anh, Vo Ngoc Ha My, Nguyen Thi Phuong Anh, and Tran Thi Truc Ly; Le Ho Thi Quynh Anh and Tran Binh Thang analysed and interpreted data. Le Ho Thi Quynh Anh and Nguyen Vu Quoc Huy were responsible for data curation. Peter Pype, Nguyen Vu Quoc Huy, Johan Wens, and Nguyen Minh Tam administered and supervised the research activities. Le Ho Thi Quynh Anh, Peter Pype, and Nguyen Vu Quoc Huy wrote the original draft. All authors contributed to revising and editing the final version. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the VLIR Inter-University Cooperation Program (VLIR-IUC) with Hue University, Vietnam (VN2019IUC026A103). The funders had no role in data analysis, publication decisions, or manuscript preparation.
Ethical approval
This study was approved by the Ethical Committee in Biomedical Research of Hue University of Medicine and Pharmacy on 3 June 2020 (Approval number: H2020/073) and extended on 5 April 2021 (Approval number: H2021/021). Written informed consent was obtained before the interviews. All participants had the right to withdraw from the study at any time. All methods followed relevant guidelines and regulations, as well as an ethical approval statement and informed consent to participation.
Consent for publication
Our manuscript does not contain any individual person’s data in any form.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.