
Abstract
Checkpoint inhibitor immunotherapy has recently started to play a fundamental role in the management of metastatic melanoma. It is however accountable for many undesirable adverse effects involving many organ systems. Eosinophilic fasciitis is a rare immune-related adverse effect associated to checkpoint inhibitors such as pembrolizumab and nivolumab. We report the case of a 25-year-old male who received pembrolizumab as a second-line therapy for metastatic melanoma. Approximately 8 months after starting the treatment, the patient developed signs and symptoms of eosinophilic fasciitis, including edema of his hands and lower legs, as well as joint limitation. Pembrolizumab was discontinued after 15 cycles because of symptom progression. The patient experienced complete resolution of symptoms 4 months after cessation of pembrolizumab and without corticosteroids. This case illustrates the reversibility of this immune adverse effect by discontinuation of the treatment, speculating that corticotherapy may not be needed in all cases.
Introduction
Since the approval of new therapeutic agents for advanced-stage melanoma, the prognosis of metastatic melanoma has considerably improved. Immune checkpoint inhibitors have revolutionized the approach for this malignancy and were able to achieve unprecedented survival results. Indeed, the 5-year overall survival with a combination of ipilimumab and nivolumab has reached 52% in Checkmate 067 trial with a median overall survival of 60 months. 1 This survival rate compares favorably with the 6,2 months historical mean overall survival of patients with stage 4 melanoma established in a landmark meta-analysis including 42 phase II trials from cooperative groups 2 conducted before the immunotherapy era.
Although immunotherapy has prolonged overall survival rates in advanced-stage melanoma, it also carries a variety of secondary effects. Rarely, some patients will develop eosinophilic fasciitis secondary to checkpoint inhibitors. Eosinophilic fasciitis is a rare connective tissue disorder that was first documented by Shulman in 1974. 3 Patients typically present with bilateral swelling, erythema and thickening of the skin of distal extremities, with occasionally characteristic groove sign and peau d’orange appearance of the skin.3,4 Tissue biopsy classically demonstrates inflammatory infiltration of the fascia, as well as fibrosis and fascial thickening. Eosinophilic infiltration, when present, is generally transient and is not required for the diagnosis of eosinophilic fasciitis. Patients are normally treated with corticosteroids as a first-line therapy or with methotrexate as second-line therapy for patients who respond inadequately to prednisone.
Here, we present the case of a 25-year-old man with metastatic melanoma that was treated with pembrolizumab who further developed eosinophilic fasciitis in the hands and legs and who recovered without treatment.
Case
A 25-year-old male initially presented with a melanoma on the left scalp with cervical and inguinal adenopathy. After biopsy confirmed metastatic disease with BRAF V600 mutation, the treatment option was debated between targeted agents and immunotherapy. In the hope of a long-term remission, it was decided to treat with immunotherapy. As ipilimumab was the only approved agent at the time, this treatment was initiated and four cycles were completed. Two years later, the patient developed a new subcutaneous nodule on his back. The biopsy confirmed a subcutaneous metastasis and the positron emission tomography (PET) scan showed an 8 mm lesion at the surface of the spleen. Given the progression of his disease, he received a treatment of pembrolizumab at a dose of 2 mg/kg every 3 weeks, for a total of 15 cycles. The best response achieved on treatment was a partial response. At his 10th cycle of pembrolizumab, the patient presented subjective morning stiffness and edema in the legs and hands, as well as pain in both knees. The patient later experienced range of motion restriction, mainly preventing him from closing his hands. Cutaneous examination revealed erythema, edema as well as cutaneous sclerosis involving metacarpal joints and upward toward the wrist as well as distal legs up to the calves. Pitting edema was prominent on the lower legs; however, Stemmer’s sign was negative which entails pinching and tenting the dorsal tissues of the foot. There was a positive prayer sign. No groove sign was noted. No calcinosis nor telangiectasias.
Laboratory tests revealed a progressive eosinophilia over 6 months, increasing from 700 cells/mm3 to 3400 cells/mm3. Skin biopsy of the second finger of the left hand and lateral malleolus of the left ankle revealed chronic subcutaneous inflammation, fibrosis of the dermis and infiltration of the fascia with mononucleated cells, confirming the diagnosis of eosinophilic fasciitis (shown in Figure 1). The use of pembrolizumab was discontinued at that time after a total of 15 cycles. Systemic steroids were offered but declined as spontaneous resolution was already underway with drug cessation. A complete resolution of symptoms and eosinophilia was reached within 4 months without corticosteroid treatment. Despite 45 weeks of exposure to pembrolizumab, the patient still managed to reach a complete remission of the immune-related adverse effect. A radiological follow-up with PET scans was undertaken after treatment discontinuation. The disease remained stable for 18 months. Then, the patient became symptomatic due to a rapidly evolving intraabdominal relapse and was started on targeted therapy with a combination of BRAF and MEK inhibitors.
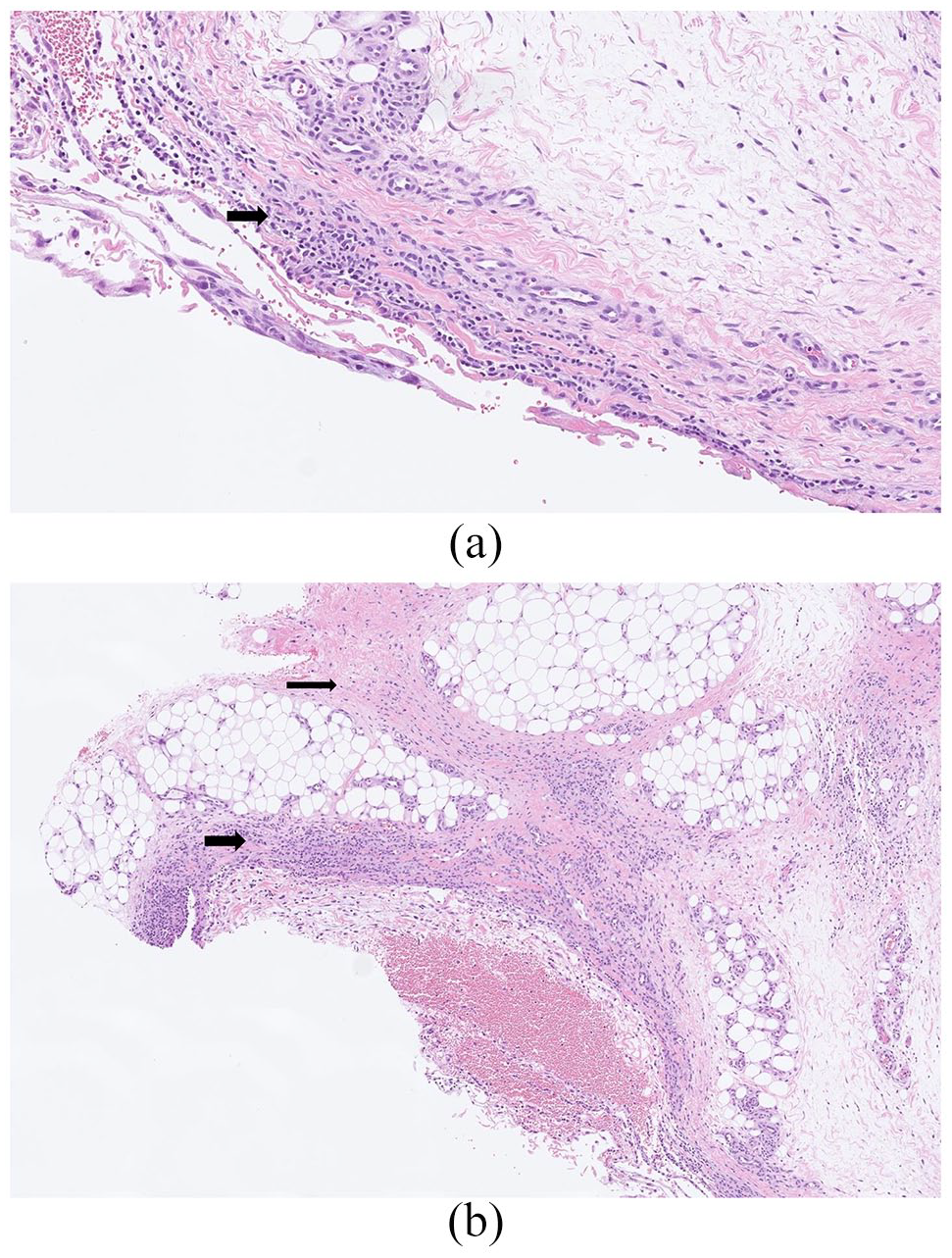
Histology of skin biopsy. (a) Fibrosis and enlargement of subcutaneous septa shown by thin arrow. Thick arrow indicates inflammatory infiltration of fascia. (b) Fascia and subcutaneous septa infiltration by mononucleated cell inflammation, such as lymphocytes. Arrow indicates inflammatory infiltration of fascia.
Discussion
The introduction of immunotherapy in the management of patients with metastatic melanoma has revolutionized the clinical evolution of this malignancy. Conventional chemotherapy such as dacarbazine or platinum agent almost never achieved neither adequate nor long-term results. However, in the last years, several studies have demonstrated that checkpoint inhibitors, such as anti-PD1 antibodies and anti-CTLA-4 antibodies, are considerably optimizing the outcome of this malignancy. In 2015, Robert et al. compared overall survival rates in patients treated with dacarbazine and patients treated with nivolumab, an anti-PD1 antibody. In the group of patients receiving nivolumab, the overall survival rate at 1 year was 72.9%, while the group of patients treated with dacarbazine was 42.1%. 5
Although immunotherapy is promising for the outcome of metastatic melanoma, it is nonetheless associated with a myriad of immune-related adverse effects. Cutaneous side effects, namely maculopapular rash, count for the majority of immune-related adverse events to immune checkpoint inhibitors and usually present as the first sign of toxicity and can develop after only a few weeks. 6 To date, a total of 15 cases of eosinophilic fasciitis induced by checkpoint inhibitors have been reported in the literature. 7 Among these, 13 were secondary to PD1 blockade and 6 specifically to pembrolizumab. The reported cases of eosinophilic fasciitis secondary to pembrolizumab showed similar symptoms as our patient, including swelling of the extremities, restricted range of motion, and thickening of the skin.
Eosinophilic fasciitis is a rare connective tissue disorder whose pathophysiology remains unknown. Apart from occurring secondarily to immunotherapy as we presented here, eosinophilic fasciitis appears in an idiopathic manner in the majority of cases. When comparing the two, we notice similarities, as well as some disparities. Both present predominantly with symmetrical swelling of the distal limbs with myalgia and limited range of motion in the affected area. Face and digit involvement are almost always absent in idiopathic eosinophilic fasciitis, while many cases of eosinophilic fasciitis associated to immunotherapy seem to have involvement of the hands, accounting for 43.7% (7 of 16 cases). 7
The vast majority of cases of eosinophilic fasciitis secondary to pembrolizumab reported in the literature were treated with long-term steroids or immunosuppressive drugs like methotrexate. 7 Specifically, eight cases were treated with a combination of prednisone and methotrexate, one case received prednisone and mycophenolate and 2 other cases were treated with methylprednisolone only. 7 Oppositely, we present a case that had a spontaneous remission of eosinophilic fasciitis following the discontinuation of immunotherapy. To our knowledge, only one other case in the literature describes a complete remission of fasciitis associated to immunotherapy without steroids or immunosuppressive drugs. Narváez et al. 8 reported a full recovery of this immune-related adverse effect with solely nonsteroidal anti-inflammatory drug (NSAID) and drug withdrawal. However, it is important to note that some aspects differentiate our patient from the case reported by Narváez et al., 8 making the two cases unique. First, they describe a patient who developed an inflammatory myositis with fasciitis in the lower extremities. Therefore, they do not specifically describe a case of spontaneous remission of eosinophilic fasciitis and consequently cannot illustrate the reversibility of eosinophilic fasciitis without systemic treatment. Second, the patient Narváez et al. described was only exposed to pembrolizumab for a total of 9 weeks, making the exposure time to the causal agent quite shorter than in our case. Therefore, this case successfully illustrates that the reversal of eosinophilic fasciitis is not solely obtained after brief exposition to immunotherapy.
Footnotes
Acknowledgements
The authors thank Alain Marion for analyzing histology of skin biopsy. Centre de formation médicale du Nouveau-Brunswick in the Acknowledgements.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was approved by the institute’s committee on human research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The authors have received the written informed consent of the subject.