
Abstract
Cerebral venous sinus thrombosis (CVST) typically presents as headache, papilledema, and seizures. A dural arteriovenous fistula (DAVF) is a rare intracranial vascular malformation, and common symptoms include headache, pulsatile tinnitus, and stroke. The occurrence of CVST as a complication of DAVF is infrequent. Moreover, optic neuropathy presenting as the initial symptom of CVST and secondary DAVF is also unusual. We present a case of a patient with optic neuropathy and persistent intracranial hypertension who underwent head magnetic resonance imaging, which indicated CVST. She received normative anticoagulant and dehydration therapy; however, a repeated lumbar puncture showed dramatically increased intracranial pressure. Further digital subtraction angiography revealed an intracranial DAVF. The patient was finally diagnosed with a DAVF and secondary CVST. This case indicates that intractable optic neuropathy could be an uncommon indicator for CVST and secondary DAVF. Early diagnosis and early treatment are essential for visual rehabilitation and prognosis improvement.
Keywords
Introduction
Two case reports involving optic neuropathy and dural arteriovenous fistula (DAVF) have been reported in the literature. Micieli et al reported a patient presenting with papilledema who was diagnosed with cerebral venous sinus thrombosis (CVST) and secondary DAVF 1 year after symptom onset. 1 Ahmed et al reported two patients with DAVF presenting with headache and papilledema caused by intracranial hypertension. 2 Neither report described underlying DAVF and secondary CVST. This report describes a patient with optic neuropathy and persistent intracranial hypertension who underwent head magnetic resonance imaging, which indicated cerebral venous sinus thrombosis. She received normative anticoagulant and dehydration therapy, and a repeat lumbar puncture showed a marked increase in intracranial pressure. Further digital subtraction angiography showed an intracranial DAVF. The patient was finally diagnosed with DAVF and secondary CVST. This case indicates that intractable optic neuropathy could be an uncommon warning for DAVF. Early diagnosis and early treatment are essential for visual rehabilitation and prognosis improvement.
Case report
The reporting of this study conforms to the CARE guidelines. 3 A 36-year-old woman presented with visual impairment and motor evoked pain in her left eye for 2 months without headache, binocular diplopia, nausea, or vomiting. An ophthalmologic evaluation revealed decreased visual acuity (right, 0.8 and left, hand movement) and papilledema in the left eye. Visual evoked potentials exhibited delayed waveforms at P100, and severe mixed myelination and axon damage were observed in the left optic pathway. A neurological examination and head computed tomography scan were negative. Then, a lumbar puncture was conducted, which revealed intracranial hypertension of an unknown cause (300 mmH2O) and negative cerebrospinal fluid (CSF) findings. Additionally, all hematological and biochemical examinations were negative. Optic nerve magnetic resonance imaging with gadolinium enhancement displayed bilateral enhancement of the optic nerve sheathes on T1 post-contrast sequences, while head magnetic resonance imaging and diffusion weighted imaging results were normal (Figure 1). Further magnetic resonance venography revealed a filling defect of the left sigmoid sinus, rear portion of the superior sagittal sinus, and internal jugular vein (Figure 1). The patient was diagnosed with CVST. Tests were conducted to identify congenital risk factors for CVST, including antithrombin deficiency, protein C and protein S deficiency, factor V Leiden mutation, and genetic prothrombotic conditions, and all results were normal.

Head magnetic resonance imaging (MRI) (a and b), diffusion weighted imaging (c), and MRI with gadolinium enhancement (d) results were normal, while magnetic resonance venography displayed cerebral venous sinus thrombosis in the left sigmoid sinus, rear of the superior sagittal sinus, and internal jugular vein (e and f, black arrows). Optic nerve MRI with gadolinium enhancement revealed hyperintensities on T2-weighted images and enhancement at the bilateral optic nerve sheath and optic disc in the orbits (g–i, white arrows).
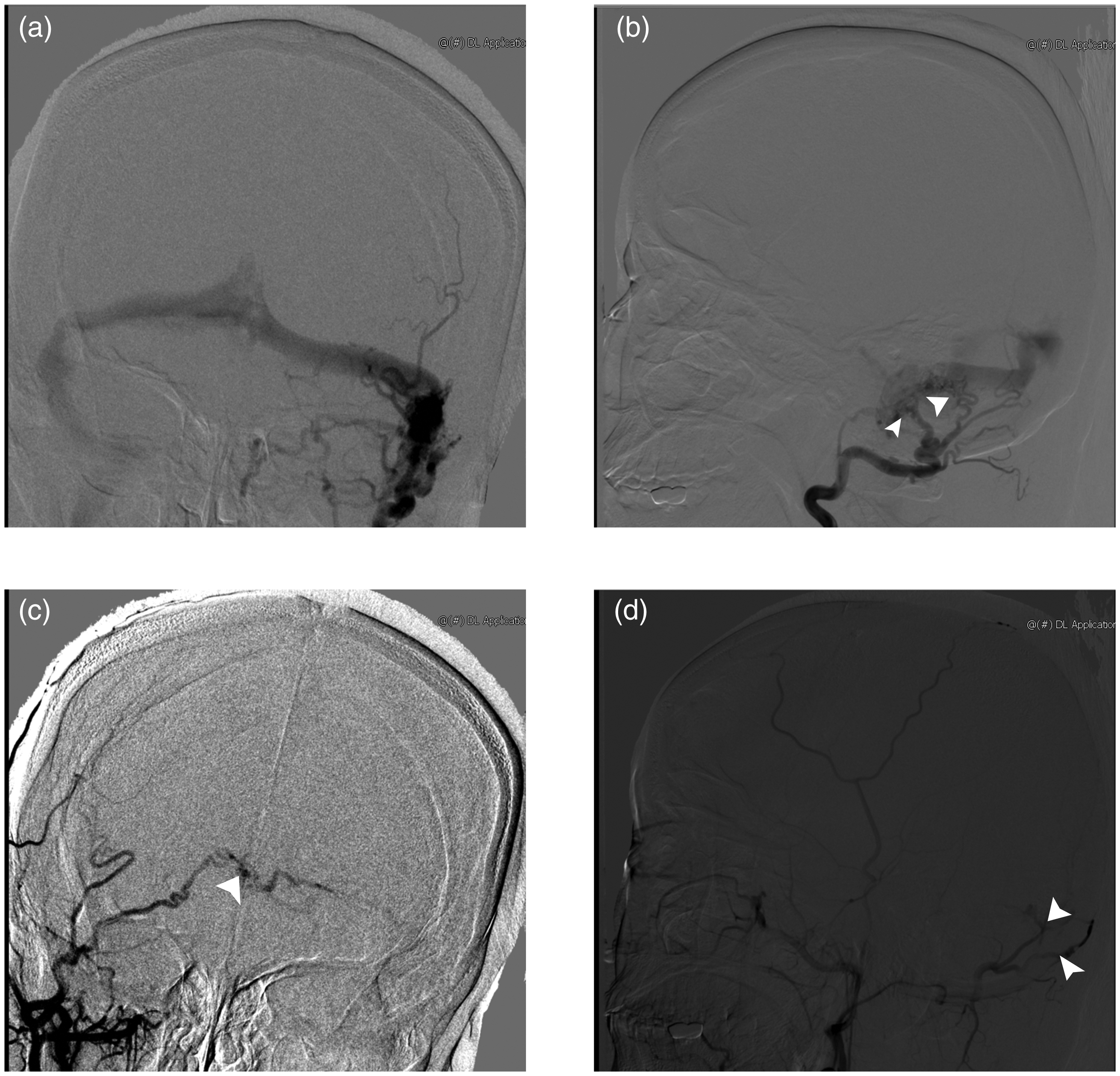
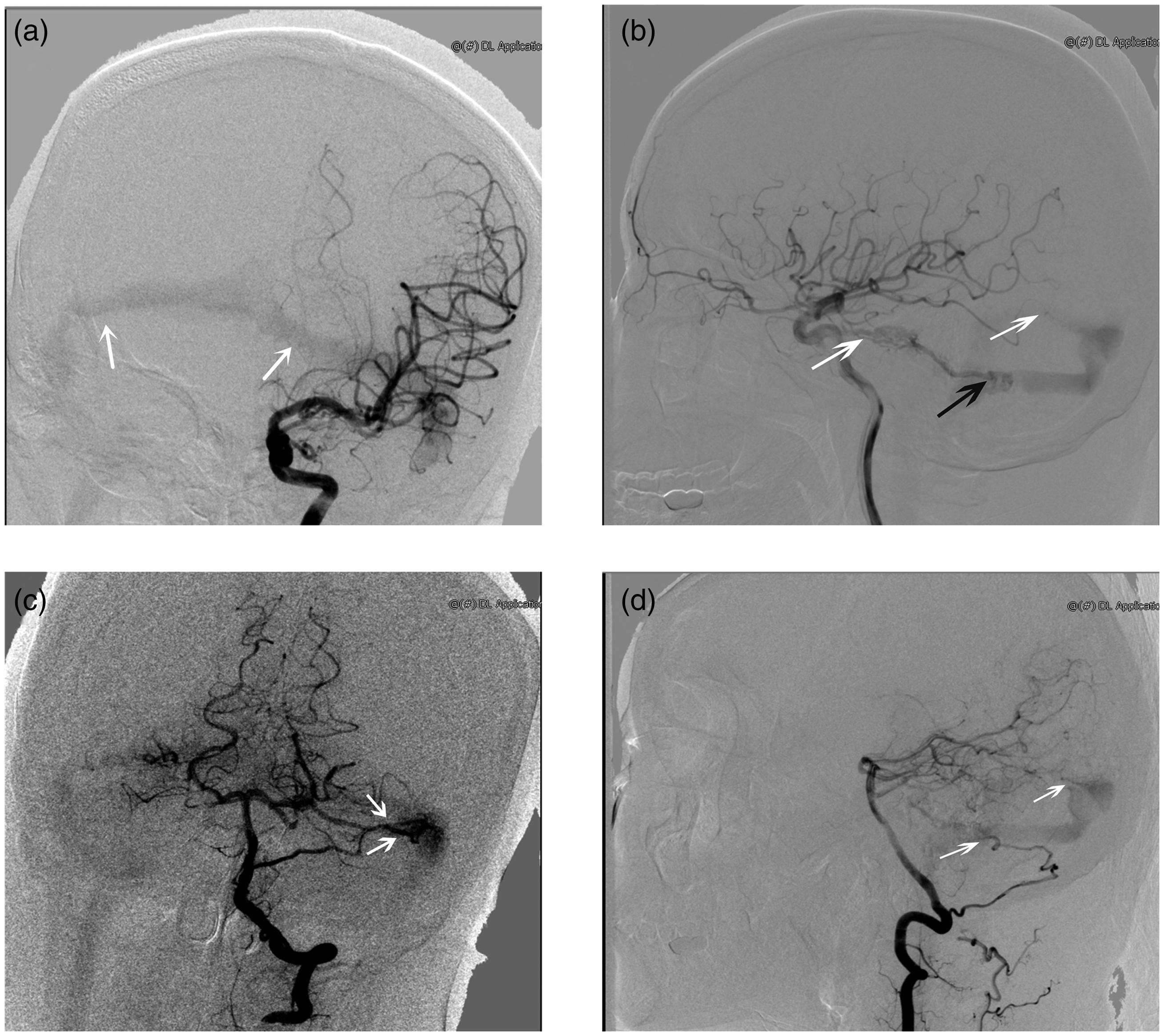
Therefore, we administered a dehydrating agent, oral acetazolamide, anticoagulant therapy, and intravenous methylprednisolone to treat the patient. Two weeks later, the patient’s symptoms had not been alleviated, and a repeat lumbar puncture showed increased intracranial pressure (400 mmH2O), although the CSF findings remained normal. Finally, cerebral digital subtraction angiography was conducted, which showed a DAVF in the left lateral sinus. The DAVF in this case was supplied by the bilateral occipital arteries, left posterior inferior cerebellar artery, and posterior cerebral artery and was drained retrogradely by the transverse sinus, sigmoid sinus, and cortical veins. It was classified as type IIa + b according to the Cognard classification (Figure 2, Figure 3). Finally, the patient underwent endovascular treatment with onyx 18. During the third month of follow-up, the intracranial pressure was normal, but the patient’s vision in the left eye remained unrecoverable.
Advanced neuroimaging evaluation with digital subtraction angiography. The dural arteriovenous fistula was situated in the left lateral sinus (a, external carotid artery, venous phase). The bilateral occipital arteries branched from the posterior cerebral artery (b–d, external carotid artery, arterial phase, white arrows).
The venous sinuses were shown previously during the arterial phase of cerebral angiography (a) internal carotid artery, arterial phase, white arrowhead). The arteriovenous malformation was located in the left posterior cranial fossa and was supplied by the anterior choroidal artery (b) internal carotid artery, arterial phase, white arrowhead), and venous drainage occurred via the transverse sinus and sigmoid sinus (b internal carotid artery, arterial phase, black arrowhead). The malformation was an accessory vascularization secondary to the dural arteriovenous fistula (DAVF) and participated in shunting superfluous blood flow volume. The dominant feeding arteries of the DAVF were the left posterior inferior cerebellar artery and the left posterior cerebral artery (c and d vertebral artery, arterial phase, white arrowhead).
Discussion
Severe headache, hemiparesis, aphasia, seizures and visual impairments are frequent symptoms of CVST. 4 Papilledema is common and results from intracranial hypertension. However, optic neuropathy is a relatively rare complication of CVST. A DAVF is characterized by abnormal arteriovenous shunts in the intracranial dura mater, which is supplied by the meningeal arteries, and the annual detection rate of DAVF is 0.29 per 100,000 adults. The clinical course of DAVF includes pulsatile tinnitus, cognitive impairment, and stroke. 5 Nearly 40% of patients with a DAVF also have CVST, primarily at the venous sinus near the DAVF and downstream venous drainage pathways. 6 Several recent cases have been reported concerning CVST and an underlying DAVF, and all patients presented with headache, hemiparesis, or decreased vision.1,7,8 However, in this case, the initial symptom of our patient was optic neuropathy.
We speculated that the “first” disorder was the DAVF, which was followed by CVST. Increased CSF pressure caused by a DAVF results in axoplasmic flow stasis in the optic nerve, which produces swelling of the nerve fibers and optic disc, which then compresses venules causing venous stasis and leading to fluid leakage, extracellular fluid and protein accumulation, optic nerve demyelination, and, eventually, vision loss. 9 The mechanism of intracranial hypertension is summarized as follows: elevated fistulous pressure increases cerebral blood volume and impairs CSF absorption, while venous hypertension obstructs venous outflow. 10 A DAVF leads to turbulent flow into the venous sinus, which injures the intima and generates luminal thrombosis. Additionally, CVST amplifies venous hypertension and further induces retrograde flow to exacerbate DAVF invasion. Delayed treatment is an important cause of poor prognosis in patients.
This report provides insights into the only reported case in which optic neuropathy was presented as the initial symptom of CVST and an underlying DAVF. Timely lumbar puncture and thorough imageological examination are critical for patients with new-onset visual symptoms. If standardized treatment shows poor therapeutic effects for CVST, further systematic examinations should be conducted as soon as possible. Vigilance regarding negative DAVF status on routine imaging studies is also required. Digital subtraction angiography is the gold standard for cerebrovascular diseases. Early diagnosis and prompt intervention help to prevent visual field impairment and optic atrophy caused by the vascular malformation.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221078071 - Supplemental material for Optic neuropathy, a warning for cerebral venous sinus thrombosis and underlying dural arteriovenous fistulae
Supplemental material, sj-pdf-1-imr-10.1177_03000605221078071 for Optic neuropathy, a warning for cerebral venous sinus thrombosis and underlying dural arteriovenous fistulae by Minjia Xiao and Xiang Huang in Journal of International Medical Research
Footnotes
Author contributions
Minjia Xiao: manuscript concept, drafting, and revision.
Xiang Huang: critical revision of the manuscript for intellectual content.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was approved by the Yueyang Central Hospital Ethics Committee. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
No financial support was received for the work reported in this paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.