
Abstract
The probability of rhabdomyosarcoma occurring in the cervix is less than 0.5% and may be associated with a pathogenic dicer 1, ribonuclease III (DICER1) gene variation. Tumour-induced hypercoagulability and high levels of cancer antigen (CA) 125 are risk factors for cerebral venous sinus thrombosis (CVST). In addition, although nonpuerperal uterine inversion is very rare and is usually caused by leiomyomas from the uterus, large cervical masses can also be the cause. This case report describes a 24-year-old woman with uterine inversion caused by an embryonic cervical rhabdomyosarcoma that presented with CVST as her first symptom. The patient underwent laparoscopic total uterus and bilateral salpingectomy, during which the uterus was found to be completely inverted. Postoperative pathology confirmed embryonic cervical rhabdomyosarcoma. The patient quickly developed lung and para-aortic lymph node metastases. Two months later, the patient died of complications. When coagulation indices in patients with tumours are abnormal, especially when the levels of D-dimer and CA125 increase, it is recommended that anticoagulant therapy is administered in a timely manner to prevent the occurrence of CVST. Furthermore, for large cervical tumours, physicians should also be alert to the occurrence of uterine inversion.
Introduction
Rhabdomyosarcoma is a malignant tumour of skeletal muscle-derived cells that usually occurs in children and adolescents. Rhabdomyosarcomas are currently divided into four histological subtypes: (i) embryonic rhabdomyosarcoma; (ii) alveolar rhabdomyosarcoma; (iii) spindle cell or sclerosing rhabdomyosarcoma; and (iv) pleomorphic rhabdomyosarcoma. 1 In addition, approximately 30% of rhabdomyosarcomas originate in the genitourinary tract in females, mainly in the vagina; less than 0.5% of cases occur in the cervix. 2 In adults, rhabdomyosarcomas of the uterine cervix are extremely rare. 2 Rhabdomyosarcoma of the female genital tract, especially uterine corpus and rarely uterine cervix, may be associated with a pathogenic dicer 1, ribonuclease III (DICER1) gene variation. 3 , 4
Cerebral venous sinus thrombosis (CVST) is a rare and fatal disease that has an incidence in adults of only 3–4 per 100 000 per year. 5 CVST is characterized by blood clotting in cerebral veins, dural sinuses or rare veins such as cortical veins. CVST occurs in the background of a hypercoagulable state caused by local factors (an infection of the head or face, surgery or trauma) or systemic factors (such as oral contraceptives, pregnancy and the puerperium, hereditary thrombotic diseases, antiphospholipid syndrome and cancer). 6 In addition, studies have shown that cancer-related CVST only accounts for 7.4% of cases and occurs more often in malignant haematological diseases than in solid tumours. 7 It is unusual for young women with embryonic cervical rhabdomyosarcoma to present first with the symptoms of CVST rather than the symptoms of rhabdomyosarcoma.
Inversion of the uterus refers to a rare and serious obstetric and gynaecological disease in which the bottom of the uterus sinks into the uterine cavity and part or all of the uterus is turned out to the cervix. 8 Uterine inversion is usually divided into two types: (i) obstetric or puerperal; and (ii) gynaecological or nonpuerperal. Inversion is a rare complication in obstetrics, but it is rarer in gynaecology and is usually due to uterine fibroids or endometrial carcinosarcoma. 9 However, gynaecological uterine inversion caused by a large embryonic cervical rhabdomyosarcoma has not been previously reported.
This current case report describes the first and only case of uterine inversion caused by an embryonic cervical rhabdomyosarcoma with CVST as the first symptom.
Case report
A 24-year-old unmarried woman was admitted to the Department of Neurology, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China because of severe unresponsiveness and twitching in October 2019. Subsequent computed tomography of the skull showed low-density shadows of the left temporal lobe and bilateral frontal lobe. Magnetic resonance imaging (MRI) of the skull and intracranial blood vessels showed direct enhancement of the cranial veins and brain. Diffusion imaging of the brain showed multiple filling defects, abnormal enhancement and diffuse signals at the distal end and branch of the superior sagittal sinus, the left transverse sinus-sigmoid sinus-internal jugular vein and the right transverse sinus. The patient’s prothrombin time was 13.4 s, prothrombin activity was 77% and D-dimer was 0.88 μg/ml. The patient was considered to have CVST with brain parenchymal damage (cerebral oedema and venous infarction). Therefore, the patient underwent whole cerebral angiography via femoral artery catheterization and catheterization thrombolysis. After the operation, the patient was given comprehensive treatments, such as thrombolysis, sedation and lowering of intracranial pressure.
The patient’s bone marrow aspiration result was verified to be normal. To identify the cause of CVST in such a young woman, a thorough medical history was taken and the patient reported a history of increased menstrual flow for 6 months, increased vaginal discharge and a peculiar smell for 1 month. Prior routine examination of leucorrhoea in the local hospital showed inflammatory changes. After taking oral anti-inflammatory drugs for 1 month, the condition did not improve. Then, the patient was given an urgent examination with uterine accessory ultrasound to prompt the following question: is this condition uterine disease? MRI of the pelvic cavity demonstrated an enlarged cervix with an irregular shape. The neurologist asked the gynaecologist for two consultations in total. The first physical examination found that there was redness and swelling at the vaginal opening and that the tumour was limited to the vaginal opening, and then a biopsy was performed. Five days later, the second physical examination showed that there was a mass of approximately 9 cm in diameter in the vagina, covered with pus and stained with blood, and the pedicle could not be touched (Figure 1a). After the patient's neurological symptoms improved, she was transferred to the Department of Gynaecology, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, China for gynaecological treatment in November 2019.

Subsequent physical examinations of a 24-year-old woman that was admitted with neurological symptoms of cerebral venous sinus thrombosis revealed a very large lump in the vagina that was observed to increase in size during consecutive examinations: (a) 9 cm in diameter; (b) 11 cm in diameter; and (c) 14 cm in diameter. The colour version of this figure is available at: http://imr.sagepub.com.
After being transferred to the Department of Gynaecology, a gynaecologist (L.M.) performed two physical examinations and found that the tumour was progressively prolapsed. The diameter had increased from 11 cm to 14 cm, of which the pedicle could not be touched (Figures 1b and 1c). The patient's cancer antigen (CA) 125 level was 36.4 U/ml. The pathological examination of the vaginal mass confirmed a tumour. Therefore, the patient was given laparoscopic total hysterectomy and bilateral salpingo-oophorectomy. During the operation, it was found that the patient's cervical tumour was approximately 15 × 15 × 15 cm, touching the thick pedicle, which was approximately 2.5 cm in diameter. What was confusing for the physicians was that the patient's uterus was found to be completely inverted and adhered to the left ovary and the front wall of the rectum, but there was no mass in the uterus. The two fallopian tubes were stuck together and the appearance of both ovaries was normal (Figures 2a and 2b). As there was no evidence of extrauterine spread of the tumour at the time of surgery, the tumour was staged as clinical group I based on the Intergroup Rhabdomyosarcoma Study (IRS)-I. 10 Finally, postoperative histology confirmed embryonic cervical rhabdomyosarcoma with a tumour size of 18 × 16 × 7 cm, which invaded the whole layer of the cervical wall, and a tumour thrombus was seen in the vessel (Figure 3). Immunohistochemistry revealed the following: CD10 (++), CD117 (–), CD34 (–), CD68 (+), CKpan (−), desmin (++), DOG1 (–), Ki-67 (90%+), LCA (–), lysozyme (–), MyoD1 (–), myogenin (+), S-100 (–), SMA (–) and vimentin (+). However, the patient declined further chemotherapy and radiotherapy, and then she was discharged.

Subsequent intraoperative examination of a 24-year-old woman that was admitted with neurological symptoms of cerebral venous sinus thrombosis revealed a large tumour of approximately 15 cm in diameter that protruded from the vulva (a). Surgical removal of the tumour and the inverted uterus (b). The colour version of this figure is available at: http://imr.sagepub.com.
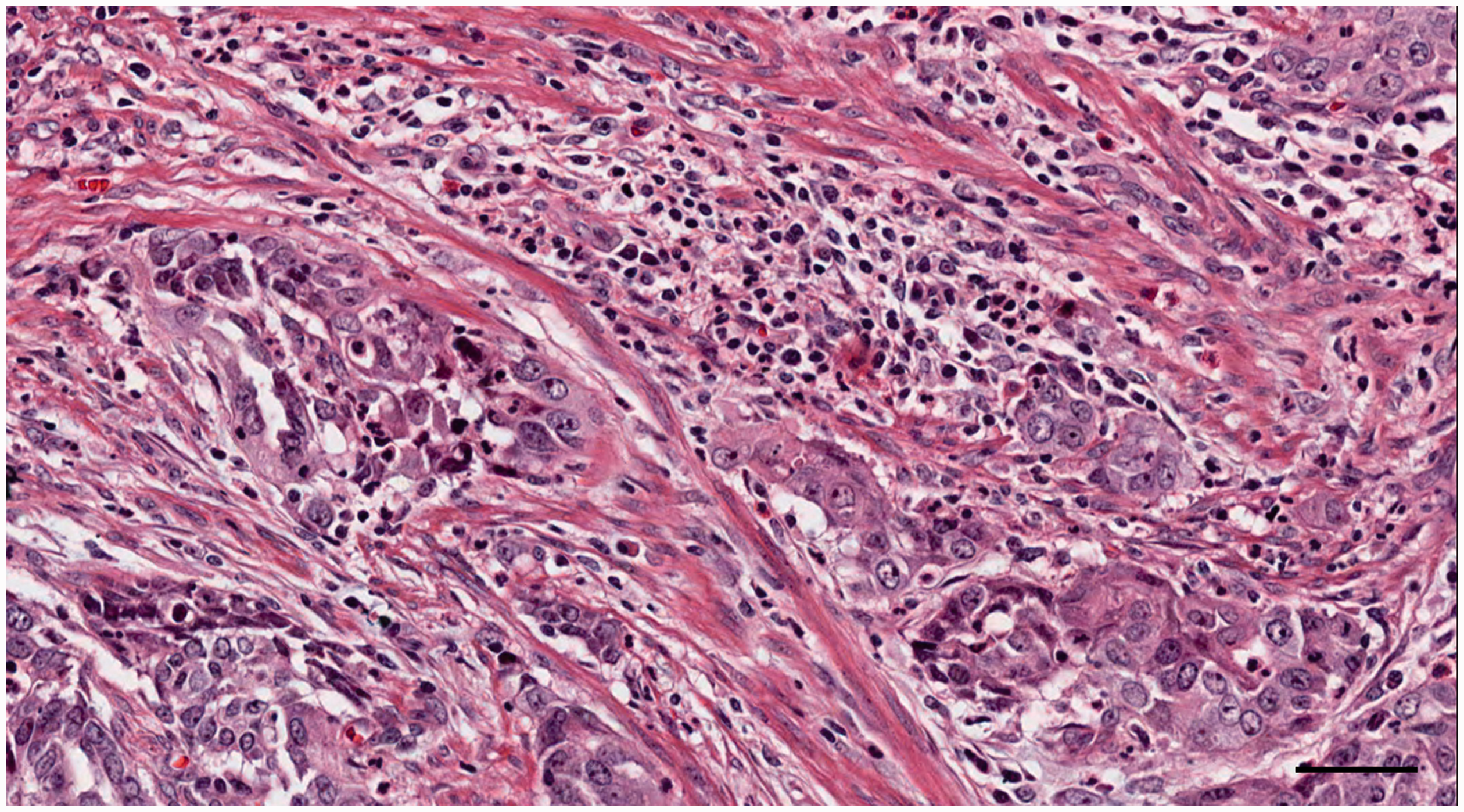
Histopathology examination of the tumour confirmed that the cervical mass was an embryonic rhabdomyosarcoma, which had invaded the whole layer of the cervical wall. A tumour thrombus was seen in a blood vessel. The tissue section was counter-stained with haematoxylin and eosin. Scale bar 100 µm. The colour version of this figure is available at: http://imr.sagepub.com.
Two months later in January 2020, the patient quickly showed signs of relapse. A physical examination revealed a mass of approximately 8 × 8 × 5 cm in the vaginal stump that was crumbly and bled when touched (Figure 4a). Based on the IRS treatment scheme, 11 adjuvant chemotherapy with vincristine, actinomycin-D and cytoxan was administered (2 mg vincristine on day 1 + 0.4 mg actinomycin-D on days 2–6 + 0.4 g cytoxan on days 2–6; intravenous infusion). As the patient’s condition progressed rapidly, the vaginal mass progressively increased to 13.53 × 9.92 × 10.74 cm in size (Figure 4b) and there were lung metastases and para-aortic lymph node metastases during the second chemotherapy session. The patient refused subsequent chemotherapy and was discharged. Two months later, the patient died of complications. The reporting of this study conforms to CARE guidelines. 12 Written informed consent was obtained from the patient to publish this case report and the patient was reassured that all of her information would be deidentified.

Subsequent physical examination of a 24-year-old woman that was admitted with neurological symptoms of cerebral venous sinus thrombosis revealed a mass of approximately 8 × 8 × 5 cm in the vaginal stump that was crumbly and bled when touched (a). The vaginal mass increased to 13.53 × 9.92 × 10.74 cm in size during the second chemotherapy session (b). The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
Although rhabdomyosarcoma is relatively common among children with vaginal sarcoma, embryonic cervical rhabdomyosarcoma is extremely rare and usually occurs in women in the second and third decade of life. 13 Among the four subtypes of rhabdomyosarcoma, the embryonic type is the most common type with a relatively good prognosis. 14 In addition, rhabdomyosarcoma of the female genital tract, especially the uterine corpus and rarely the uterine cervix, may be associated with a pathogenic DICER1 gene variation. 3 , 4 This is important because the detection of this mutation in a patient or relatives can provide the opportunity for surveillance of related conditions that might improve long-term outcomes and survival. However, this current case report describes a patient with a giant embryonic cervical rhabdomyosarcoma with CVST as the first symptom, leading to inversion of the uterus. Unlike other reports, 15 , 16 this current patient’s condition was not controlled after comprehensive treatment in accordance with the guidelines and she only survived for 4 months. Moreover, as far as we know, this is the first and only case of uterine inversion caused by a cervical tumour.
Since the first report of a case of cervical rhabdomyosarcoma in a 75-year-old woman in 1971, 24 cases in adults have been reported (Table 1).15–35 The age ranges from 19 to 75 years. The most common symptoms were vaginal bleeding and swelling. Only one case was reported for examination because of abnormal vaginal discharge, which was consistent with the current case. 31 Five patients presented with symptoms of cervical polyps, which usually occurred in sarcoma botryoides, a subtype of embryonal rhabdomyosarcoma, because it arose beneath a mucous membrane. Although the largest diameter of the mass was 10 cm among these cases,15–35 the current case was 18 cm, indicating that the patient’s condition was progressing rapidly and that her prognosis was poor. The IRS group of most patients was stage I, so the current case was no exception. There was one case of stage II disease, two cases of stage III disease and two cases of inoperable disease.

IRS, Intergroup Rhabdomyosarcoma Study; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; PPLND, pelvic and para-aortic lymph node dissection; DTIC, dacarbazine; DOXO, doxorubicin; VAC, vincristine + actinomycin-D + cytoxan; Gy, Gray; D&C, dilation and curettage; RH, radical hysterectomy; CYC, cyclophosphamide; ERT, external radiotherapy; MRH, modified radical hysterectomy; PAD, cisplatin, doxorubicin and dacarbazine; PLND, pelvic lymph node dissection; UV, upper vaginectomy; BPL, bilateral pelvic lymphadenectomy; EI, etoposide and ifosfamide; V(DOXO)I-EI, vincristine (doxorubicin) ifosfamide-etoposide and ifosfamide; V(CYC)I-EI, vincristine (cyclophosphamide) ifosfamide-etoposide and ifosfamide; RH-PPA SL, radical hysterectomy, pelvic para-aortic systematic lymphadenectomy; VA, vincristine and actinomycin-D; LEEP, loop electrosurgical excisional procedure; RTra, robotic-assisted radical trachelectomy; CVST, cerebral venous sinus thrombosis; LTH, laparoscopic total hysterectomy.
For early-stage patients, most patients can survive disease-free for more than 12 months through surgery, radiotherapy and chemotherapy. 36 In addition to the case reported here, only one patient survived less than 1 year (case 6). A previous case series described two cases of cervical rhabdomyosarcoma, both of which were treated with local surgical resection and adjuvant chemotherapy, and they remained disease-free for a long period of time. 30 Total abdominal hysterectomy and bilateral salpingo-oophorectomy are the first choices for the treatment of cervical rhabdomyosarcoma. The most widely used chemotherapy regimens include vincristine, actinomycin-D and cytoxan (VAC). 23 Research has shown that for adult rhabdomyosarcoma, surgery combined with VAC chemotherapy resulted in the overall survival of 55% of patients and 64% disease-free survival at 2 years. 37 However, unlike previous reports, 18 the current patient relapsed 2 months after the operation. During the second VAC chemotherapy, the patient developed lung metastasis and para-aortic lymph node metastasis. Reviewing her medical history, the patient was found to have had a 6-month history of abnormal leucorrhoea, but there was no formal diagnosis or treatment; only the vaginal inflammation was treated, which delayed the condition. Chemotherapy is recommended for all rhabdomyosarcoma cases at all stages. 37 In the present case, the patient refused chemotherapy after surgery and had a local, regional and metastatic relapse, which was not unexpected as she did not receive chemotherapy. Metastatic disease is known to have a very poor prognosis (<20% survival). 38 Tumour thrombi seen in the blood vessels of the primary tumour may have been a factor in the regional and metastatic relapse in the current case, so the course of the disease was not unexpected.
Although the most common cause of CVST is primary hypercoagulability (approximately 19.17% of all causes), cancer is also an important factor. 5 Previous studies have shown that among all CVST patients, approximately 7–10% are cancer patients, especially patients with haematological malignancies. 39 Among CVST-related solid tumours, lung, breast and stomach cancers are the most common; and cervical rhabdomyosarcoma is rare. 40 The cause of CVST caused by tumours may be that the tumour directly invades the blood vessels and provides the perfect conditions for thrombosis; and patients are prone to secondary opportunistic infections or poor general health. 41 The current patient’s histopathological results showed that the tumour had invaded the entire layer of the cervical wall and tumour thrombi were seen in the blood vessels, which was the cause of CVST. A recent study on the pathogenesis of somatic cancer-related CVST (n = 174) showed that high levels of D-dimer and CA125 were risk factors for CVST. The risk for CVST in the somatic cancer-related CVST group increased independently by 0.7% (odds ration [OR] 1.007; 95% confidence interval [CI] 1.000, 1.015; P = 0.047) with a 1 ng/ml increase in D-dimer levels and by 4.6% (OR 1.046; 95% CI 1.011, 1.083; P = 0.010) with a 1U/ml increased in carcinoembryonic antigen. 42 In the current case, the patient's D-dimer and CA125 levels were high. Therefore, for cancer patients, it is essential that coagulation indices are measured to prevent the occurrence of CVST.
In this current case, the most surprising finding was that the patient had a uterine inversion. The nonpuerperal type is mainly associated with uterine tumours located at the uterine fundus rather than the cervix. For example, a previous study reported that 13.6% of nonpuerperal uterine inversions were sarcomas, 71.6% were leiomyomas, 6.8% were endometrial carcinomas and 8.0% were idiopathic. 43 A previous report summarized 32 cases of uterine inversion caused by sarcoma since 1987; only three cases were rhabdomyosarcoma and they were all embryonic. 44 The main reasons for uterine inversion are as follows: (i) the tumour was extruded from the uterus; (ii) the uterine wall was thin; (iii) the cervix was dilated; (iv) the tumour size; (v) the tumour pedicle was thick; and (vi) the tumour attachment site. 45 Uterine inversion might have occurred in the current case because of the large cervical rhabdomyosarcoma, which grew into the uterine cavity, rapidly protruded outwards. During the transfer of the current patient from the Department of Neurology to the Department of Gynaecology, the uterus was compressed because of the change in position. In our opinion, uterine inversion may also be caused by a tumour in the cervix, so obstetricians and gynaecologists should also pay close attention to this finding.
In conclusion, this current case report described a 24-year-old woman diagnosed with CVST caused by a cervical tumour. Embryonic cervical rhabdomyosarcoma is a rare malignant tumour and its typical manifestations are vaginal bleeding and a pelvic mass. However, attention should also be paid to any abnormal vaginal discharge in young unmarried women. Standard physical examination and pelvic ultrasound are essential. In addition, when the coagulation indices of patients with tumours are abnormal, especially when the levels of D-dimer and CA125 increase, it is recommended to perform anticoagulation therapy and craniocerebral vascular MRI to prevent the occurrence of CVST as soon as possible. It should be noted that nonpuerperal uterine inversion can be caused by a large cervical mass in addition to the more usual uterine mass.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the innovation ability of Hebei Obstetrics and Gynaecology Clinical Medicine Research Centre (no. 20577705D).