
Abstract
Fulminant idiopathic intracranial hypertension is a rare presentation of idiopathic intracranial hypertension in which visual decline occurs within 4 weeks of initial symptom presentation. Idiopathic intracranial hypertension usually presents with headaches, visual disturbances, and in women who are overweight. We present a case of idiopathic intracranial hypertension in which a female patient presented with rapid, severe vision loss within 8 days of symptom presentation and no other idiopathic intracranial hypertension symptoms. This case highlights a rare presentation of Fulminant idiopathic intracranial hypertension and the need for a quick diagnosis and treatment to preserve vision.
Introduction
The incidence of idiopathic intracranial hypertension (IIH) is 0.5–2 individuals per 100,000, with the expectation that this will continue to increase with the obesity epidemic. The most prominent symptom of IIH is the presence of a headache (reported in 75%–94% of patients). Fifty percent or more of patients also report visual obscurations (darkening of the vision), pulsatile tinnitus, back pain, and/or dizziness. Only 32% of patients report vision loss. 1 However, a minority of patients present with declining vision. Fulminant IIH is rare presentation of this disease in which rapid, severe vision loss occurs within 4 weeks of the initial symptom diagnosis.1–4 This case hypothesized that acute IIH presentation can occur in patients who are not overweight and do not present with headaches. Written informed consent to publish this information was obtained from the patient.
Case report
A woman in her early twenties presented to her ophthalmologist with complaints of visual disturbances and “light spots” beginning to obscure her vision. The patient had a long history with this ophthalmologist for corrective lenses. Her ophthalmologist determined she had bilateral papilledema and referred her to a neuro-ophthalmologist for evaluation. The neuro-ophthalmologist saw the patient on her eighth day of symptoms. Now, “steady brightness” was blocking her view in her right eye and she experienced color desaturation. The left eye did not appear to have any visual changes. The patient had a normal BMI and reported no history of being overweight, headaches, tinnitus, or previous visual disturbances. She had a 4-month history of polycystic ovarian syndrome (PCOS) for which she was being treated with a progestin and estrogen birth control.
Upon examination, papilledema was noted in both eyes as well as a 2+ right relative afferent pupillary defect. No cranial nerve deficits were noted. The patient had a 20/20 visual acuity, and a visual field test was performed. A severe peripheral visual field deficit was noted in the right eye with a mean deviation on the Humphrey scale of −26.10 dB using a Central 24-2 Threshold Test (Figure 1(a)). The normal mean deviation should be between −1 and −2 db. 5 The left eye was at baseline. The patient was admitted to the hospital for expedited vision workup. An MRI with and without contrast showed slight dilation of the optic nerve sheath, as well as an incidental small right frontal developmental venous sinus anomaly, but otherwise unremarkable (Figure 2). No tumor or thrombosis was noted on the MRI.

(a) Initial central 24-2 threshold test, MD = −26.10 dB, PSD = 10.80 dB; (b) 1-year follow-up, MD = −8.76 dB, PSD = 7.78 dB.
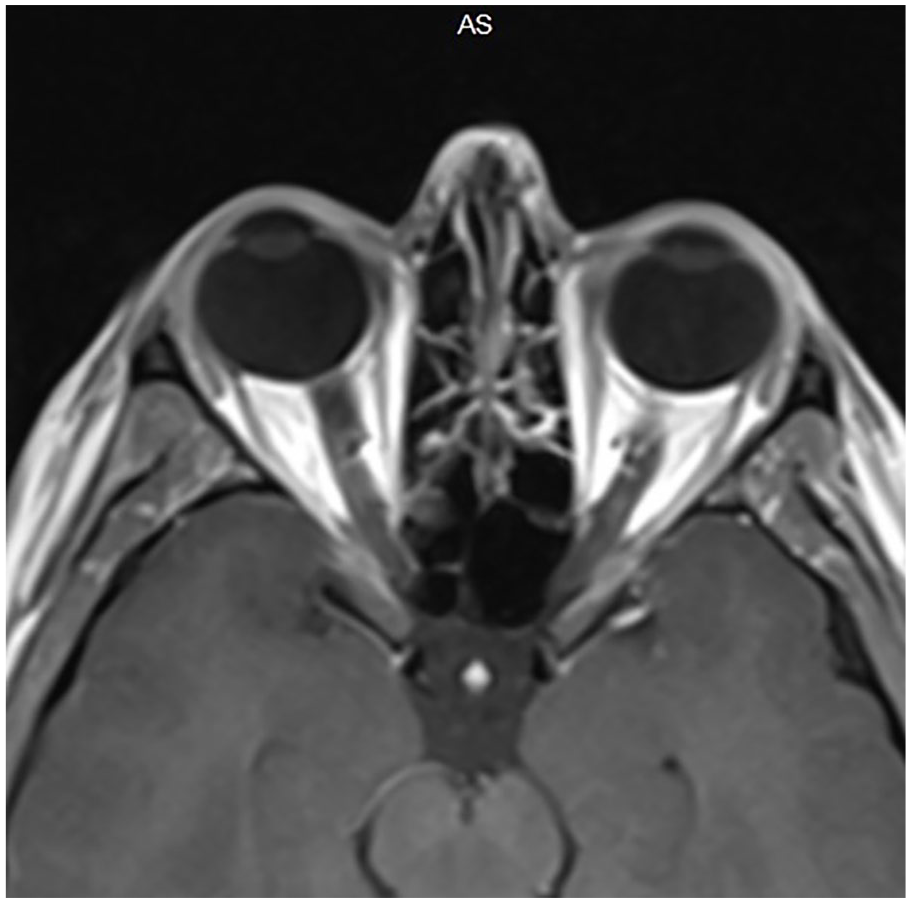
MRI with prominence of perineural CSF with mild dilation of both optic nerve sheaths.
Several tests were completed including a complete blood count, metabolic panel, routine coagulation panel, and neuro hypercoagulative panel. All results were within normal limits except for her Vitamin A which was elevated at 88 µg/dL with no known reason or dietary explanation. A lumbar puncture was performed 9 days after the initial presentation with an opening pressure of 41 cm of water. In total, 19 mL of cerebrospinal fluid (CSF) was drained and the closing pressure was 18 cm. The CSF was determined to be normal. The patient was also evaluated for systemic disorders and endocrine disorders, and all tests were negative. The patient was given the diagnosis of papilledema with secondary optic neuropathy and Vitamin A toxicity.
Discussion
To treat her diagnosis, the patient was prescribed 2 g of acetazolamide to be taken in 500-mg doses four times per day. She experienced significant vision improvements after 5 days of treatment; therefore, surgical options were placed on hold. Surgery should be performed when vision continues to deteriorate despite a lumbar puncture and medical treatment. 3 The Humphrey mean deviation changed from −26.10 to −19.97 dB in the right eye 13 days after her initial symptom presentation. Vision continued to improve with a mean deviation of −8.86 dB at a 6-month follow-up. One year later, the right eye stabilized to a mean deviation of −8.76 dB (Figure 1(b)), and the acetazolamide was decreased to 1 g per day. The left eye remained within normal limits. Although the patient does have optic neuropathy in her right eye, much of her vision was saved due to a quick diagnosis and fast treatment.
In this case, no cause of IIH was found. Although, the patient did have elevated Vitamin A levels of an unknown cause, previous work has shown Vitamin A toxicity to be an unlikely contributory factor in the causation of IIH. 6 It is likely that there is an association between IIH and her PCOS, as previous studies have inferred.1,2,7
Thambisetty et al. 3 published the largest and most comprehensive patient series on Fulminant IIH in 2007 consisting of 572 IIH cases of which approximately 2.8% of patients were given the diagnosis of Fulminant IIH. The diagnosis of Fulminant IIH must be preceded by a diagnosis of IIH based on the guidelines established by Mollan et al. 2 In addition to this diagnostic criteria, patients must also experience papilledema, have less than 4 weeks between symptom onset and severe loss of visual acuity or field, and experience rapidly worsening vision over a period of days. 4
In this study, the patient met the diagnostic criteria of Fulminant IIH with her worst vision loss reported on day 8 after initial symptom presentation. However, there were several atypical occurrences throughout this case that should be discussed. First, this patient experienced an afferent pupillary defect. The Idiopathic Intracranial Hypertension Treatment Trial (IIHTT), 4 which aimed to characterize the symptoms of IIH, reported this defect in 5.4% of IIH patients. Even more rare, is a normal BMI in IIH patients. Of the patients included in the IIHTT and a study conducted by Thambisetty et al., 3 100% were either overweight or obese, with an obesity majority. Headaches were the most common symptom in IIHTT, and in Thambisetty et al. 3 study, 100% of subjects experienced headaches. However, the patient presented here was not overweight nor did she experience headaches.
Treatment for Fulminant IIH typically involves surgery.1,3,4 Currently, the most accurate predictor for vision prognosis is vision loss at initial presentation. 8 Previous work has shown visual function improved in the majority of cases; however, all patients continued to have an abnormal visual field and 50% remained legally blind. 3 In our case study, the patient improved significantly with acetazolamide and surgery was not required. Her visual field exams, although improved, continue to remain abnormal.
This patient was fortunate to have a long-standing relationship with an ophthalmologist before her symptom presentation which allowed her to immediately present to a specialist. Unfortunately, not all patients have this ability. In a recent case study, a suspect IIH patient had to report to the Emergency Department three times in the span of 13 days before any fundoscopy exam or visual field testing was conducted. The ability to obtain accurate fundoscopy exams and visual field testing is vital in Fulminant IIH cases. 9
Conclusion
Overall, this case highlights that vision can be lost rapidly in IIH with a normal BMI and without the presence of headaches, both of which seem to be an extremely rare occurrence for Fulminant IIH. Quick diagnostics and treatment are needed for a patient who is losing vision rapidly. This case reminds us of the continued need for further research of this rare presentation.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Written informed consent to report on this case was obtained from the patient. The authors have a personal relationship with the patient.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.