
Abstract
Objective
Segmentectomy is widely performed for early-stage lung cancer. However, the effects of segmentectomy versus lobectomy on pulmonary function remain unclear. We performed a meta-analysis with the aim of comparing segmentectomy and lobectomy in terms of preservation of pulmonary function in patients with early-stage non-small-cell lung cancer (NSCLC).
Methods
We conducted a literature search of PubMed using the terms ‘pulmonary function’ AND ‘segmentectomy’ AND ‘lobectomy’. The primary outcomes of interest were the forced expiratory volume in 1 second (FEV1), FEV1 as percent of predicted (%FEV1), change in FEV1 (Δ%FEV1), and the ratio of postoperative to preoperative FEV1.
Results
Thirteen studies comprising 2027 patients met the inclusion and exclusion criteria and were included for analysis, including 787 patients in the segmentectomy group and 1240 patients in the lobectomy group. Patients in the segmentectomy group showed significantly better preservation of FEV1 and %FEV1 compared with the lobectomy group. The reduction in FEV1 after surgery was significantly less in the segmentectomy group compared with the lobectomy group, and Δ%FEV1 was significantly higher in the segmentectomy group than in the lobectomy group.
Conclusion
Segmentectomy results in better preservation of pulmonary function compared with lobectomy in patients with early-stage NSCLC.
Keywords
Introduction
Pulmonary lobectomy with systemic mediastinal lymph node dissection is a standard surgery for patients with early-stage non-small-cell lung cancer (NSCLC). A randomized trial reported by the Lung Cancer Study Group (LCSG) in 1995 comparing sublobar resection, including segmentectomy and wedge resection, suggested increased mortality and locoregional recurrence in the limited-resection group. 1 However, there were potential biases affecting the results of segmentectomy in the LCSG study, and several recent studies have suggested similar local recurrence rates following sublobar resection and lobectomy in patients with IA tumors <2 cm.2–6 Computed tomography (CT) screening allows the detection of more and earlier-stage lung cancers. 7 Anatomic segmentectomy is widely used in clinical practice because it theoretically preserves more pulmonary parenchyma, leading to better preservation of pulmonary function compared with lobectomy. However, there have been conflicting results regarding the relative advantages of segmentectomy over lobectomy in terms of pulmonary function protection.1,2,8–13 We therefore conducted a meta-analysis to compare postoperative pulmonary function between patients treated with segmentectomy and lobectomy, and to verify if segmentectomy had an advantage over lobectomy in terms of preserved pulmonary function.
Survey methodology
Study protocol
We carried out a systematic review and meta-analysis of published studies to compare pulmonary function in patients with early-stage NSCLC after segmentectomy or lobectomy. This study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Checklist. 14 Ethics approval and informed consent were not required due to the nature of this study (meta-analysis of published articles).
The protocol for this systematic review was registered on INPLASY (INPLASY202180050) and is available in full at inplasy.com (https://doi.org/10.37766/inplasy2021.8.0050).
Search strategy
We conducted a literature search of PubMed for all relevant studies published from the date of database inception to December 2020 using the following search terms in the title/abstract field: ‘pulmonary function’ AND ‘segmentectomy’ AND ‘lobectomy’. Only articles published in English were included. The reference lists of relevant review articles were checked to identify additional relevant articles.
Studies were included if they met the following criteria: direct comparison between segmentectomy and lobectomy for early-stage NSCLC; pulmonary function tests performed before and after surgery in both groups; and article in English. The exclusion criteria were: review articles; limited sublobar resection, including wedge resection; pulmonary function tests not performed during follow-up; pulmonary function determined by CT or single-photon-emission CT (SPECT), other than spirometry tests; and no detailed pulmonary function data.
Data extraction
Data were extracted independently by two authors (XW, HG). In the event of disagreement, consensus was achieved by discussion. The following data were extracted from each included article: first author, publication year, study design, patient age and sex, smoking history, operation techniques, pulmonary function parameters. Δ%FEV1 was defined as change in forced expiratory volume in 1 second (FEV1) between before and after surgery.
Quality assessment
The quality of the included studies was assessed using the Newcastle–Ottawa scale (NOS), with 9 being the highest score and a score ≥6 indicating a high-quality study. The assessments were performed independently by two authors (QH and YY), with disagreements settled by a third author (BC) if necessary.
Statistical methods
All statistical analyses were carried out using Review Manager version 5.3 (The Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity was calculated by Q-test and I2 statistics. Studies with an I2 > 50% were considered to show a high degree of heterogeneity. If heterogeneity existed, a random-effects model was adopted; otherwise, a fixed-effects model was used. Pooled analysis was performed using the inverse variance model and results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). A p value <0.05 was considered statistically significant.
Results
The literature search identified 345 studies for review. Based on the title and abstract, 28 studies were selected for full-text review. Of these, 15 studies were excluded because they measured pulmonary function using CT or SPECT (n = 6),12,13,15–18 lacked follow-up pulmonary function data (n = 4),9,11,19,20 lacked a control group of lobectomy (n = 2),21,22 did not directly compare segmentectomy and lobectomy (n = 2),23,24 or because they included surgery for benign pulmonary nodules (n = 1). 25 Thirteen studies were finally included in the meta-analysis (Figure 1).2,8,10,26–35 All studies were retrospective observational studies. The 13 studies comprised 2027 patients, including 787 patients in the segmentectomy group and 1240 patients in the lobectomy group. The patients’ baseline characteristics are summarized in Tables 1 and 2. The included studies were assessed using the NOS for quality and were all considered to be high quality (score ≥ 6), except for the study by Echavarria et al. (Table 3). Patients in 10 of the studies2,8,10,27,28,30,32–35 were classified as clinical or pathological stage I, most patients (87%–93.7%) in two other studies29,31 were classified as pathological stage I, and one study 26 did not report the precise cancer stage, but noted that all patients were clinically early-stage. There was no significant difference in the results of pulmonary function tests before surgery between the segmentectomy and lobectomy groups, except for two studies: Keenan et al. 2 and Echavarria et al. 26 showed significantly better FEV1 as percent of predicted (%FEV1) in the segmentectomy group. The average age of the patients ranged from 58.2 to 68.7 years, with no significant difference between the two groups. The percentage of females ranged from 33% to 56% in the segmentectomy group and 32.7% to 65% in the lobectomy group, with three studies having a significant difference in the percentage of females between the two groups. Five of the 13 studies provided data on smoking history, two of which showed a significant difference in smoking history between the two groups.

Flowchart of study selection.
Baseline characteristics of patients in included studies.
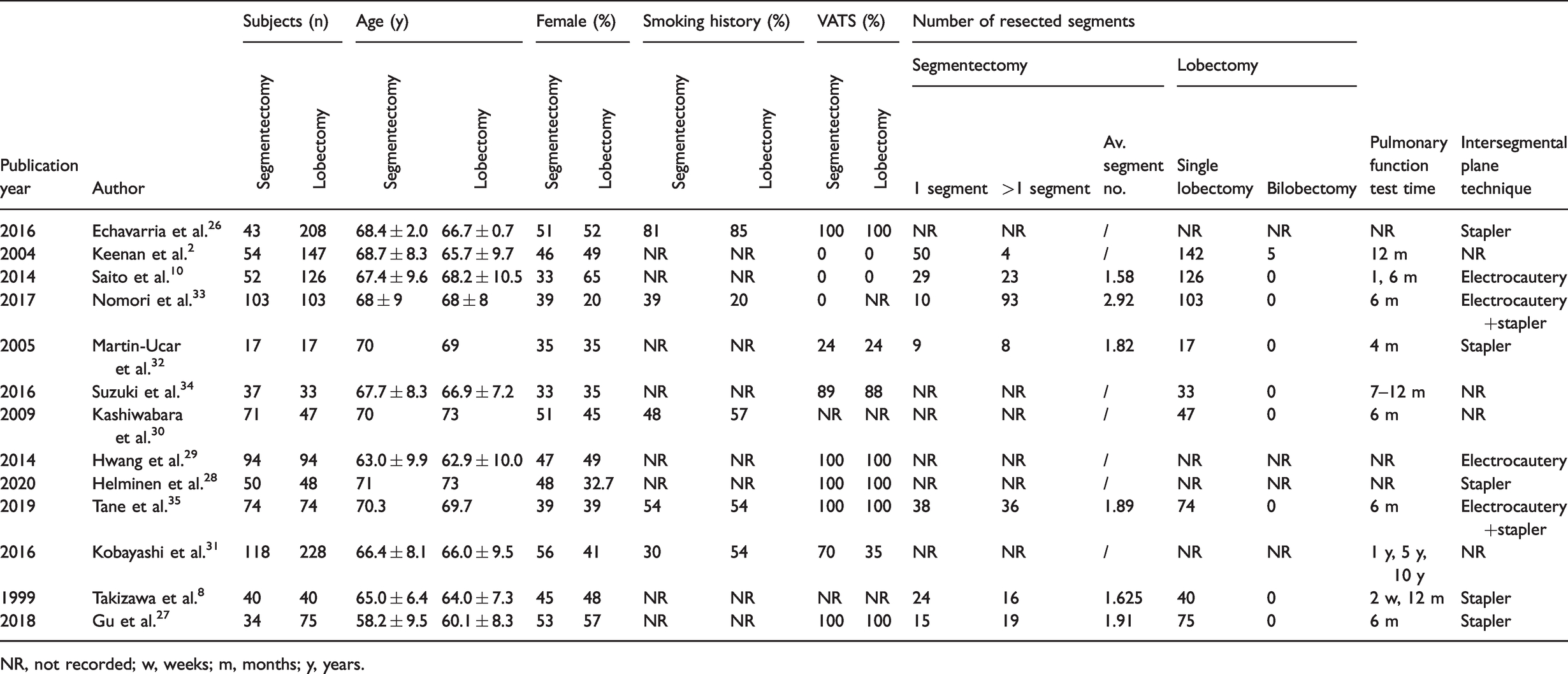
NR, not recorded; w, weeks; m, months; y, years.
Preoperative and postoperative pulmonary function in patients in included studies.

*p < 0.05 %FEV1 between segmentectomy and lobectomy.
Quality assessment of nonrandomized studies using the Newcastle–Ottawa Scale.

FEV1
Five studies8,26,27,31,35 including 933 patients provided results for postoperative pulmonary function tests, including 309 patients in the segmentectomy group and 624 patients in the lobectomy group. There was no significant difference in preoperative FEV1 between the segmentectomy and lobectomy groups in five studies, including two studies27,35 that carried out one test 6 months after surgery, one study 26 that did not mention the exact time of the test, and two studies8,31 that recorded two to three pulmonary tests during the follow-up. The maximum follow-up was 10 years after surgery in one study. To minimize the effects of the heterogeneity in terms of the timing of pulmonary tests, tests carried out 1 year after surgery were included in the analysis of these two studies. The segmentectomy group showed significantly better preservation of FEV1 compared with the lobectomy group (OR = 0.11, 95%CI, 0.00, 0.21, p = 0.05) (Figure 2). However, there was high heterogeneity (I2 = 94%) among these studies, indicating that the results need to be interpreted with caution. Three of the five studies8,27,35 provided detailed information on the number of resected segments in the segmentectomy group, and the average number of resected segments ranged from 1.63 to 1.91. Subgroup analysis of these three studies still demonstrated a significantly better FEV1 in the segmentectomy compared with the lobectomy group (OR = 0.20, 95%CI, 0.15, 0.25, p < 0.001) (Figure 2). An I2 value of 6% indicated low heterogeneity across the studies. Three of the five studies26,27,35 performed segmentectomy and lobectomy with complete video-assisted thoracoscopic surgery (VATS). Pooled analysis of these three studies indicated that FEV1 was better preserved in the segmentectomy compared with the lobectomy group (OR = 0.14, 95CI%, 0.01, 0.27, p = 0.04) (Figure 3). However, there was high heterogeneity (I2 = 97%) among these studies, indicating the need for caution. Four of five studies8,26,27,35 divided the intersegmental plane with a stapler during segmentectomy, and pooled analysis of these four studies showed better preservation of FEV1 in the segmentectomy compared with the lobectomy group (OR = 0.12, 95CI%, 0.01, 0.24, p = 0.04) (Figure 4). However, the high heterogeneity (I2 = 95%) among these studies again highlights the need for caution when interpreting the results.

Funnel plot analysis of segmentectomy versus lobectomy on postoperative FEV1.

Funnel plot analysis of segmentectomy versus lobectomy with complete video-assisted thoracoscopic surgery on FEV1.

Funnel plot analysis of segmentectomy dividing the intersegmental plane with stapler versus lobectomy on postoperative FEV1.
%FEV1
Five studies2,8,26,28,31 recorded the results of pulmonary tests in terms of %FEV1 after surgery. These studies included 976 patients, with 305 patients in the segmentectomy group and 671 patients in the lobectomy group. %FEV1 was significantly better in patients in the lobectomy group compared with the segmentectomy group according to Keenan et al. 2 and Echavarria et al., 26 but there was no significant difference between the two groups in the other three studies. Two studies26,28 did not report the exact time of the test, one study 2 did the test 12 months after surgery, and two studies8,31 included two to three tests during the follow-up period of 2 weeks to 10 years after surgery. The test carried out at 12 months after surgery was included in the analysis. Pooled analysis of these five studies concluded that there was no significant difference between the lobectomy and segmentectomy groups in terms of postoperative %FEV1 reserve (OR = −0.03, 95%CI, −10.69, 10.64) (Figure 5). After excluding the studies by Keenan et al. 2 and Echavarria et al., 26 pooled analysis of the remaining three studies demonstrated a better %FEV1 in the segmentectomy group compared with the lobectomy group (OR = 5.46, 95%CI, 2.04, 8.87, p = 0.002) (Figure 5). An I2 value of 0 indicated no potential heterogeneity across the studies.

Funnel plot analysis of segmentectomy versus lobectomy on postoperative FEV1%.
Δ%FEV1
Six studies26–30,32 including 700 patients calculated the change in FEV1 from before to after surgery. There were 259 patients in the segmentectomy group and 441 patients in the lobectomy group. There was no significant difference in FEV1 before surgery between the two groups in these six studies. Three of the six studies26,28,29 did not record the exact time of the pulmonary tests, two studies27,30 tested the FEV1 at 6 months after surgery, and one study 32 tested the FEV1 at 4 months after surgery. Pooled analysis showed a significantly smaller change in FEV1 between before and after surgery in the segmentectomy group than in the lobectomy group (OR = 7.36, 95%CI, 2.49, 12.22, p = 0.003) (Figure 6). However, there was high heterogeneity (I2 = 93%) among these studies, indicating the need for cautious interpretation.
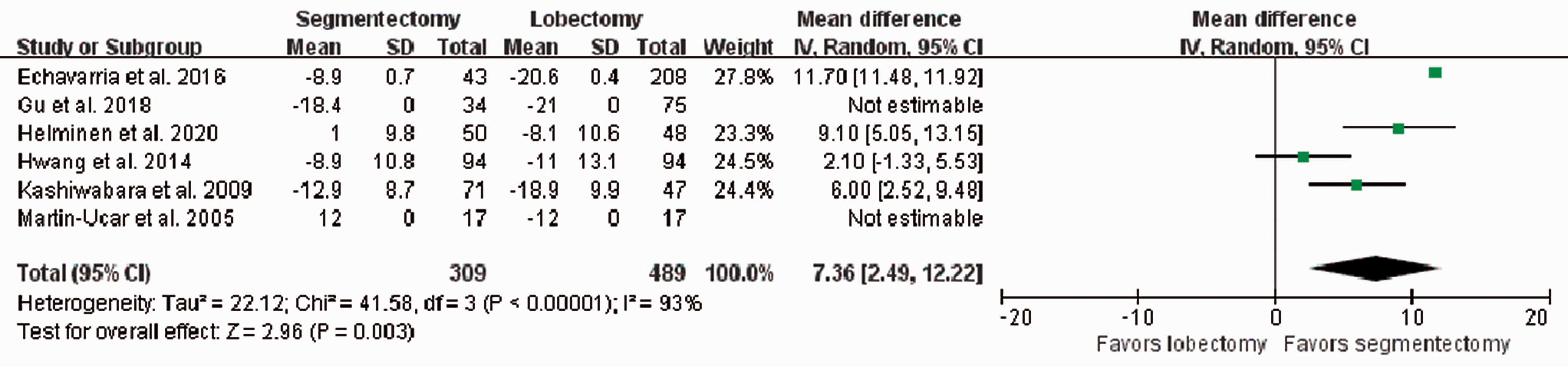
Funnel plot analysis of segmentectomy versus lobectomy on ΔFEV1%.
Ratio of postoperative to preoperative FEV1
Five studies8,10,33–35 including 682 patients calculated the ratio of postoperative to preoperative FEV1, including 306 patients in the segmentectomy group and 376 patients in the lobectomy group. There was no significant difference in preoperative FEV1 between the segmentectomy and lobectomy groups in these five studies. The timing of pulmonary tests after surgery ranged from 2 weeks to 12 months, and two of the five studies8,10 tested twice during follow-up. Tests carried out at 6 months postoperatively in one study and 12 months postoperatively in another study were included in the analysis. Pooled analysis demonstrated a significantly better postoperative to preoperative FEV1 ratio in the segmentectomy group compared with the lobectomy group (OR = 7.56, 95%CI, 5.02, 10.09, p < 0.001) (Figure 7). Four of the five studies8,10,33,35 recorded the number of resected segments in the segmentectomy group in detail, and the average number of resected segments ranged from 1.58 to 2.92. Subgroup analysis showed that the better postoperative to preoperative FEV1 ratio was preserved in the segmentectomy compared with the lobectomy group in these four studies (OR = 7.56, 95%CI, 5.02, 10.09, p < 0.001) (Figure 7). An I2 value of 0 indicated no potential heterogeneity across the studies.

Funnel plot analysis of segmentectomy versus lobectomy on ratio of postoperative to preoperative FEV1.
Discussion
Numerous retrospective studies have compared postoperative pulmonary function between patients undergoing segmentectomy and lobectomy; however, the benefits of segmentectomy in terms of preserving pulmonary function remain unclear. To the best of our knowledge, the current meta-analysis was the first to compare postoperative pulmonary function between patients treated with segmentectomy and lobectomy. A low FEV1 is an independent risk factor for complications after lung surgeries, including lobectomy and segmentectomy. 36 The current results showed that segmentectomy provided better preservation of pulmonary function in terms of FEV1, %FEV1, Δ%FEV1, and the ratio of postoperative to preoperative FEV1. A pooled analysis of five studies found no significant difference in postoperative %FEV1 between the lobectomy and segmentectomy groups; however, after excluding the studies by Keenan et al. and Echavarria et al., segmentectomy proved to be better at preserving %FEV1, possibly because preoperative %FEV1 was significantly better in the lobectomy group in these two excluded studies. The better performance of segmentectomy in protecting pulmonary function could partly be attributed to the fewer segments resected compared with lobectomy. The average number of segments resected in the included studies ranged from 1.58 to 2.92. Postoperative pulmonary function recovery differed among the measured variables. Vital capacity recovered within 1 month after surgery and FEV1 recovered within 3 months, because of surgical pain and injury.37–39 Pulmonary function then reached a stable level. 40 The pulmonary tests included in the current analysis were carried out at 6 or 12 months after surgery, and were representative of postoperative pulmonary function.
Five of the 13 included studies used a stapler to divide the intersegmental plane. Pooled analysis of these studies demonstrated that segmentectomy still preserved pulmonary function better than lobectomy in these five studies. VATS reduces the loss of pulmonary function after lobectomy as a result of decreased pain, improved chest wall mechanics, and reduced inflammation.41,42 The surgical procedures were performed with complete VATS in five of the 13 studies in this meta-analysis, and segmentectomy preserved pulmonary function significantly better than lobectomy in patients undergoing complete VATS, according to the pooled analysis. The predicted preoperative %FEV1 was >70% in all the included studies, except for one which had a mean preoperative %FEV1 of 55.3% in the segmentectomy group, which was significantly worse than the 75.1% in the lobectomy group. Kashiwabara et al. 30 suggested that segmentectomy should be considered in patients with a normal (>80%) predicted postoperative FEV1, given that patients with an estimated postoperative FEV1/predicted normal FEV1 ratio <70% gained no functional benefit from segmentectomy. However, their conclusion was based on a small sample of 50 patients and should thus be translated cautiously in clinical practice. A large-scale prospective study is needed to explore the benefits of segmentectomy in patients with poor pulmonary function. Nomori et al. 43 reported that postoperative pulmonary function after left upper division segmentectomy was similar to that after left upper lobectomy. Similarly, the function of the right middle lobe was significantly decreased after right upper lobectomy compared with that after segmentectomy of the right up lobe.18,44,45 The current study could not draw any conclusions regarding whether or not postoperative pulmonary function was affected by the location of the resected segments, because relevant detailed information was not provided by the included studies.
This study had several limitations. First, the meta-analysis may have had a publication bias because we limited the search to studies published in English. However, we were unable to analyze publication bias because of the small number of studies. Second, pulmonary function parameters were restricted to FEV1 in our analysis, because information on other potentially relevant parameters was not available in all the studies. Third, we only included studies that compared pulmonary function using spirometry tests other than CT or SPECT.
Conclusion
This was the first meta-analysis to evaluate and compare postoperative pulmonary function after segmentectomy and lobectomy in patients with early-stage NSCLC. The results suggested that segmentectomy preserved pulmonary function in these patients better than lobectomy. However, further well-designed, large-scale randomized prospective studies are needed to confirm our findings in clinical practice.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Taizhou Municipal Science and Technology Bureau (grant number 1801ky09) and the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (grant number 2019KY773).