
Abstract
Objective
We investigated the correlation of lung function parameters with increased body mass index (BMI) and waist circumference (WC) and determined the impact on health-related quality of life (HRQoL).
Methods
We conducted a cross-sectional analytical study at a teaching hospital among 173 individuals. We assessed anthropometric measurements, dynamic lung function, clinical history, and HRQoL using the Airway Questionnaire. Correlations of dynamic lung function parameters with BMI and WC were analyzed.
Results
In total, 51% were men (mean patient age 47.8 ± 10.5 years, median 48 years). The average BMI was 30.3 ± 8 kg/m2. Among 173 participants, 49% were smokers, with 16 ± 9 pack-years smoked; 80% of participants had chronic obstructive pulmonary disease (COPD). We observed compromised mid-expiratory flow (MEF), especially in young and overweight smokers. A moderately strong positive relationship was observed between WC and HRQoL scores, indicating a decline in HRQoL with increased WC.
Conclusion
In our study, HRQoL declined with increasing WC. We found a decrease in MEF among young and overweight smokers who were otherwise healthy and whose other lung function parameters were normal; this finding can be regarded as a pre-COPD marker. These individuals should be reassessed for the development of COPD. Further prospective studies are needed to verify our findings.
Keywords
Introduction
Obesity is a worldwide problem, and its prevalence is increasing steadily. Between 1980 and 2008, the prevalence of obesity exhibited a rising trend worldwide. 1 During 2009 to 2010, more than one-third of American adults were obese, with obesity more prevalent among female individuals. 2 Obesity and increased body mass index (BMI) are associated with metabolic and other health-related disorders, such as hyperlipidemia, hypertension, diabetes mellitus, ischemic cardiomyopathy, apnea hypopnea syndrome, cerebrovascular accident, death at younger ages, and bone diseases. These disorders result in a decrease in overall life quality. 3 Obesity also leads to worse outcomes of respiratory illnesses.
To examine how obesity influences the respiratory function of an individual, many researchers have used spirometry to measure lung volume.4,5 Weight influences respiratory effort and pulmonary function parameters in the form of impaired pulmonary function, small airway hyper-reactivity and compromised expiratory flow, alterations in respiratory mechanics, decreased chest wall and lung compliance, respiratory muscle weakness, decreased pulmonary gas exchange, decreased breathing effort, and compromised exercise capacity.6–9
Chronic obstructive pulmonary disease (COPD) is among the most common non-communicable health-related conditions worldwide. COPD is mostly associated with bouts of exacerbation, and these exacerbations are associated with an accelerated decline in health-related quality of life (HRQoL) and high morbidity and mortality. 10 COPD is associated with a wide range of comorbidities such as cardiovascular diseases, metabolic abnormalities, and peripheral myopathies. 11 Obesity is emerging as an increasingly prevalent comorbid condition of COPD. 12
Most patients with COPD are overweight and obese. 13 Obesity is associated with restrictive-type defects on spirometry, and patients with COPD may have both restrictive and obstructive defects. Therefore, it is difficult to evaluate and treat COPD in obese patients. 14 It is postulated that the relationship between COPD and obesity will be clarified in the future, ushering in a new era of treatment. 15
HRQoL is an important aspect to ascertain the effect of any chronic illness in the community. Assessment of HRQoL is a useful tool to determine the burden of a disease. Many HRQoL questionnaires and instruments have been formulated for clinical research. Such instruments should be simple and comprehensively cover various aspects of functional status, emotional tendencies, social interaction, and symptoms. 16 The Airway Questionnaire 20 (AQ20) has been used in studies for the assessment of HRQoL. 17 The AQ20 was formulated for patients with obstructive lung disease. 17 This instrument comprises 20 questions with scores ranging from 0 to 20; a higher score predicts poor HRQoL.1,18
In the present study, we aimed to determine the correlations between forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC) and mid-expiratory flow (MEF) with BMI and waist circumference (WC) in otherwise healthy overweight adults and in overweight patients with stable COPD as well as to compare HRQoL scores using the AQ20.
Methods
Study design
This cross-sectional analytical study was conducted in Medical Unit 2 of Civil Hospital Karachi over 6 months from May 2019 to October 2019. Approval from the DUHS Institutional Review Board was obtained in April 2019 (# IRB-1236/DUHS/Approval/2019).
The reporting of this study was according to the principles of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 20
Definitions
We defined patients with stable COPD as follows: 1) patients with known COPD diagnosed according to criteria of the Global Initiative for Obstructive Lung Disease consensus; 11 2) history of chronic cough with productive sputum, along with a history of smoking (≥2 packs/day); and 3) no history of hospitalization in the past 6 months owing to exacerbation.
Body mass was assessed using BMI, calculated as height in meters and weight in kilograms. We used BMI to define obesity, according to Asia–Pacific criteria. 21 Underweight is defined as BMI <18.5 kg/m2, normal weight as 18.5–22.9 kg/m2, overweight as 23–24.0 kg/m2, and obesity as ≥25 kg/m2. Waist circumference (WC) was measured according to the World Health Organization (WHO) protocol. 22 Study participants removed all clothing and accessories and stood straight, with feet shoulder-width apart and arms crossed over the chest. The midpoint between the lower border of the rib cage and iliac crest was used to measure WC. We used WC cutoff values for central obesity of <90 cm and ≥90 cm.
The AQ20 questionnaire is designed to measure and quantify breathing problems. The AQ20 is used to query respondents' subjective opinion regarding how their breathing problems affect their HRQoL. The questionnaire takes approximately 3 to 4 minutes to complete. 17 Scoring of the AQ20 is as follows: yes responses are scored 1 point, and responses of no and not applicable are scored 0 points. The total score ranges from 0 to 20, with higher scores indicating poorer HRQoL.
Sample collection
Smokers and current non-smokers between age 30 and 65 years who completed a basic history and physical examination and who fulfilled the inclusion criteria were enrolled in the study using random, non-probability convenience sampling. Informed signed written consent was received from all study participants. Details of all participants were anonymized to maintain privacy. In this study, we included all patients with stable COPD and BMI ≥23 kg/m2 (overweight or obese) and no other known comorbidities, along with a control group of otherwise healthy individuals with BMI ≥23 kg/m2. Potential confounders were controlled by excluding pregnant individuals, those with acute respiratory tract infection, or exacerbation of COPD. Standardization of the data collection techniques, procedures, and calibration of data collection devices were ensured to avoid biased measurements.
Sample size
Sample size was calculated using PASS version 16.0 software (NCSS, LLC; Kaysville, UT, USA), in which the prevalence of overweight and obese individuals was maintained at 20.8% and 4.8%, respectively, as specified by the WHO in 2016. 23 A sample size of 32 for the control group could achieve 95.11% power to detect a difference (P1–P0) of −0.2920 in a two-sided Z-test that uses S(P0) to estimate the standard deviation, with a significance level (alpha) of 0.05. These results assume that the population proportion under the null hypothesis (P0) is 0.50. Using the same parameters and a reported frequency of obesity in COPD of 35%, 24 the sample size for the COPD group was calculated as 139.
Data collection
Anthropometric measurements such as BMI and WC were recorded by a trained designated data collector in the Medical Department. A non-stretchable standardized tape measure was used to measure WC in all participants, according to WHO protocol. For weight and height measurement, a weight scale with built-in height measurement was used by a trained data collection technician. All measurements were recorded to one decimal place and were rounded to the nearest digit. Calculations of BMI using the recorded height and weight measurements were made on site using data collection forms.
All participants underwent dynamic lung volume testing or spirometry testing using a Spirobank II spirometer ( ). We assessed FEV1, FVC, MEF (i.e., forced expiratory flow 25% to 75%). After lung volume assessment, the AQ20 questionnaire was completed by all participants in both study groups to determine the impact of respiratory involvement on HRQoL.
Quantitative variables and statistical analysis
All data were entered into Microsoft Excel 2003 software (Microsoft Corporation, Redmond, WA, USA) and transferred to IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA) for analysis. Quantitative variables such as age, height, weight, BMI, duration of COPD, and dynamic lung function parameters are presented as mean and standard deviation as well as median with minimum and maximum values. Variables such as sex and smoking status are presented as absolute frequencies and percentages. All data of spirometric assessment and dynamic lung function (FEV1 in liters, FVC in liters, MEF in liters/second, and ratio of FEV1/FVC in percentage [FEV1%]) were documented. AQ questionnaire scores were calculated and used to assess participants' HRQoL.
The data were checked for normality assumptions (and other assumptions appropriate for the relevant statistical tests), and appropriate nonparametric equivalents were used to estimate the test statistics. Spearman rank correlation was used to measure the correlation between scale variables. The significance value was set at a 5% level.
Subgroups were created based on known cutoffs for the respective variables, and subgroup analysis was conducted. Individuals with BMI ≥23 kg/m2 were divided into groups with COPD and without COPD. Participants were grouped according to the cutoff for WC (90 cm). The sample was also grouped according to BMI as overweight (23–24.9 kg/m2) and obese (>25 kg/m2).
The chi-square test was used to compare qualitative variables between groups, Correlations were investigated between dynamic lung function parameters (FEV1, FVC, and MEF) and WC and BMI in both groups. HRQoL scores according to the AQ20 were analyzed in both groups using the Student t-test.
Results
In this study, we enrolled 173 individuals, comprising 138 (80%) overweight or obese (BMI ≥23 kg/m2) individuals with stable COPD (COPD group) and 35 (20%) overweight/obese but otherwise healthy individuals (control group). Of the total, 51% were men, and the mean patient age was 47.8 ± 10.5 years (median 48 years). The average BMI was 30.3 ± 8 kg/m2. Among participants in the COPD group, 49% were smokers, with 16 ± 9 pack-years smoked. No study participants had comorbidities apart from being overweight and having COPD. Table 1 shows the salient features of participants.
Sociodemographic characteristics, anthropometric measurements, and lifestyle habits of study participants.
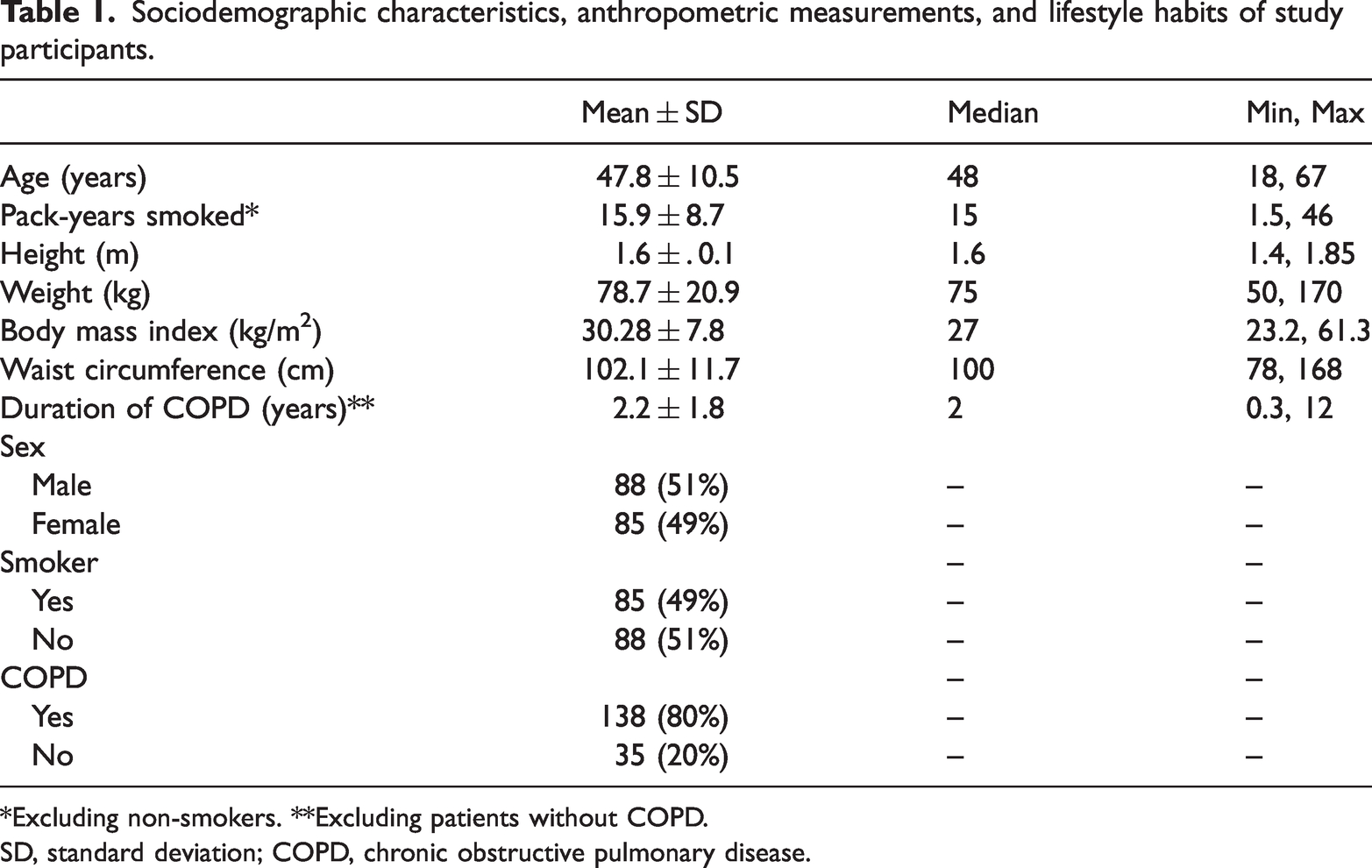
*Excluding non-smokers. **Excluding patients without COPD.
SD, standard deviation; COPD, chronic obstructive pulmonary disease.
Table 2 shows the results of subgroup analysis for comparisons of age, pack-years smoked, dynamic lung function parameters, and HRQoL scores with BMI, WC, and COPD history. HRQoL scores (AQ20) were significantly lower in people with WC ≥90 cm, compared with those who had WC <90 cm. However, there was no difference in HRQoL with respect to BMI categories. Similarly, lower HRQoL scores showed a moderately strong positive correlation with increased WC, and this correlation was stronger in women than in men (Table 3).
Subgroup analysis of pulmonary function test results, BMI, WC, and COPD (n = 173).

Note: Values in the same row and sub-table not sharing the same symbol are significantly different at p < 0.05 in a two-sided test of equality for column proportions. Cells with no symbol were not included in the test. Tests assume equal variances (i.e., tests are adjusted for all pairwise comparisons within a row in each sub-table using Bonferroni correction).
SD, standard deviation; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; HRQoL, health-related quality of life; AQ20, Airway Questionnaire 20.
Correlation matrix showing the relationship of study variables separately by sex (n = 173).

BMI, body mass index; WC, waist circumference; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; HRQoL, health-related quality of life; MEF, mid-expiratory flow.
The data characteristics and distribution of Spearman rank correlation were analyzed according to sex (Table 3). Our subgroup analysis for HRQoL with respect to COPD status revealed no significant difference for patients with BMI <25 kg/m2. However, patients with COPD and BMI ≥25 kg/m2 reported poorer HRQoL than individuals without COPD and a similar BMI. We observed decreased MEF among healthy younger and overweight smokers with otherwise normal lung function parameters. There were no significant differences in the MEF respiratory parameters between participants with and without COPD. The effect of WC was more pronounced than that of BMI, revealing its relative superior sensitivity over BMI. The duration of COPD showed a moderate positive correlation with pack-years and HRQoL in both men and women.
Discussion
The relationship of BMI and WC with dynamic lung function parameters is complex and controversial. Many past studies investigating the impact of BMI and WC on spirometric parameters have not reached consensus and have reached varying conclusions. We sought to address this issue in our study, comparing these factors in healthy overweight participants and overweight participants with COPD.
Our findings did not demonstrate any significant impact of increased BMI on dynamic lung parameters in either participant group, which contradicts the findings of Hatem et al., 25 who demonstrated a significant decline in all dynamic lung function parameters including FVC, FEV1, and MEF with increasing BMI. However, all participants in that study were healthy and did not have COPD.
We also detected a weak positive correlation between MEF and BMI. This could be owing to the positive effect of a slightly increased body weight in patients with COPD, as identified by Benslimane et al. 26 Those authors reported that a slight increase in BMI can have a positive impact on lung function parameters and improve COPD, a phenomenon known as the COPD paradox.
Our study also revealed that compared with BMI, central obesity (WC) was more strongly associated with variations in dynamic lung function parameters. Most lung function parameters in men and some in women demonstrated a negative association with WC. Our findings specifically highlighted that among dynamic lung function tests, MEF exhibited a significant negative correlation with WC. This finding negates the results of Foumani et al. 27 Svartengren et al. reported a comparable decrease in predicted FVC among participants with central obesity; however, their study analyzed patients based on their level of physical activity. 28
Our findings suggested the adverse effects of central obesity on the MEF rate. Because age is a known predictor of declining lung function, the already compromised MEF at a young age observed in our patients with COPD might be considered a predictor of COPD at an advanced age. Thus, compromised MEF could be regarded as a pre-COPD marker of small- to medium-sized airway resistance. 29 However, our current study design may not be suitable for quantifying changes in dynamic lung function over time among overweight and obese patients with and without COPD. 29 Nevertheless, the implications of our findings include the importance of intervention for central obesity in younger overweight individuals, especially those with COPD.
Not surprisingly, the duration of COPD was correlated with pack-years smoked and HRQoL scores in all male and female participants. This may be interpreted in two ways. 1) Heavy smokers develop COPD earlier in life; hence, at the time of this study, these individuals had long-standing COPD and a high number of pack-years smoked, 30 2) Smokers tend to become dependent on nicotine with time, irrespective of a deteriorating COPD status. Hence, at the time of this study, these individuals had long-standing COPD with a high number of pack-years smoked. 30 Any prolonged illness will have a negative impact on HRQoL, so an early onset of COPD will lead to worse outcomes. Regardless of how our findings are interpreted, the results are consistent with the fact that smoking harms lung health and smokers perform poorly on lung function tests.
Our data confirmed that HRQoL declines with higher WC, as well with long-standing COPD. This relationship was observed in both male and female participants. However, a similar but weak relationship was observed with BMI and HRQoL only among women in our sample. This finding is comparable to those of Benslimane et al. 26 This more marked response among female participants could be owing to women having smaller caliber airways and reduced reserved lung volume in comparison with men. 26
Limitations
This study has several limitations. First, our finding of no difference in MEF between participants with and without COPD could be owing to the confounding effects of smoking in young and overweight healthy smokers. Second, we found that all dynamic lung function parameters in men and a few in women showed a negative relationship with WC. However, the effect size was very small and did not achieve statistical significance in most instances. Owing to attrition in the sample size for subgroup analysis, we cannot confidently reach any conclusions regarding the unexpected finding of a weak positive correlation of MEF with BMI, which should be interpreted with caution. Future studies should have larger sample sizes to conduct subgroup analyses with sufficient power to clarify the relationship of dynamic lung function tests with various benchmarks (BMI/WC) of obesity and overweight.
Conclusion
WC was more closely correlated than BMI with dynamic lung function in our study participants. We found that MEF might be a good predictor of future COPD in high-risk populations might be considered a pre-COPD marker. We found that mean HRQoL scores significantly differed in individuals with WC above or below 90 cm but were not affected by normal or higher BMI values. HRQoL declined with increased WC, an indicator of central obesity, which may require prompt intervention to help prevent the onset of or progression to COPD.
Footnotes
Acknowledgement
We are extremely grateful to all the participants who gave their precious time for this research and who showed great enthusiasm for this study.
Author contributions
ZN contributed to the design, conceptualization, and data interpretation as well as the statistical analysis. MAJ made substantial contributions to the literature review and writing of the final manuscript draft. ZH helped with data collection. All authors meet the ICMJE criteria for authorship and have read and approved the final version of the manuscript.
Data availability statement
Data will be provided if needed or requested from the corresponding author.
Declaration of conflicting interest
The authors report no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.