
Abstract
Objective
To investigate the occurrence rate and risk factors of postoperative nausea and vomiting (PONV) in lung cancer patients following lobectomy and application of analgesic pumps.
Methods
This retrospective study reviewed clinical data from patients that had undergone lobectomy for lung cancer under general anaesthesia. The risk factors of PONV were analysed using binary logistic regression models.
Results
A total of 203 patients (97 females) were enrolled. The rate of PONV was 29.6% (60 of 203 patients) for all patients, 42.3% (41 of 97 patients) for female patients and 17.9% (19 of 106 patients) for male patients. Female patients undergoing thoracotomy (odds ratio [OR] 7.770, 95% confidence interval [CI] 1.747, 34.568) or having surgery durations ≥120 min (OR 4.493, 95% CI 1.502, 12.851) were significantly more susceptible to PONV. The risk of PONV in female patients that received postoperative dolasetron (100 mg, once a day) was significantly lower (OR 0.075, 95% CI 0.007, 0.834). For male patients, the risk of PONV was significantly lower in those with a body mass index ≥24 kg/m2 (OR 0.166; 95% CI 0.035, 0.782).
Conclusion
Female and male patients have different risk factors for PONV following lobectomy for lung cancer and application of analgesic pumps.
Introduction
Lung cancer is the second most commonly diagnosed cancer and it was the leading cause of cancer deaths in 2020, with 2.2 million new lung cancer cases and 1.8 million deaths, representing close to one in 10 (11.4%) cancers diagnosed and one in 5 (18.0%) deaths. 1 Surgery is the primary treatment for patients with early stage lung cancer.
Nausea is a subjective sensation of an urge to vomit in the absence of expulsive muscular movements, requiring activation of the cerebral hemispheres dealing with conscious sensations. Vomiting is the forcible expulsion through the mouth of the gastric contents, requiring a complex reflex under the control of the vomiting centre in the lateral reticular formation and the chemoreceptor trigger zone in the fourth ventricle. 2 Although nausea and vomiting are two biologically different phenomena, they often accompany each other and are highly correlated in clinical practice. Therefore, postoperative nausea and postoperative vomiting are commonly recorded together as one endpoint termed as postoperative nausea and vomiting (PONV).3–5
Postoperative nausea and vomiting is a common complication following anaesthesia and surgery, with the incidence ranging from 20–30%. 6 PONV can lead to a series of adverse events, including aspiration, wound dehiscence, bleeding, dehydration, electrolyte imbalance and an inability to begin oral medications,7,8 which can result in a prolonged hospital stay and increased healthcare costs. It is assumed that PONV has a multifactorial origin, such as patient-related factors (e.g. female sex and a negative smoking history), anaesthetic factors (e.g. volatile anaesthetics and opioids) and surgical factors (e.g. type and duration of the surgical procedure).4–7 5-Hydroxytryptamine (HT) receptor antagonists are widely used in the management of PONV. 9
For lung cancer patients treated by lobectomy, analgesic pumps supplying opioid pain-controlling medicines are widely used during post-surgical recovery as they provide consistent methods of pain management as compared with frequent analgesic injections. 10 However, this application tends to increase the incidence of PONV in patients, especially female patients. 10 The incidence and risk factors of PONV in lung cancer patients following lobectomy and postoperative application of analgesic pumps have not been well studied to date. 11 Therefore, this retrospective study investigated the occurrence rate and risk factors of PONV in this large group of patients.
Patient and methods
Study population
This retrospective study retrospectively reviewed consecutive patients that had undergone lobectomy for lung cancer under general anaesthesia at the Department of Thoracic Surgery, Sun Yat-sen University Cancer Centre, Guangzhou, Guangdong Province, China between May 2020 and December 2020. The inclusion criteria were as follows: (i) ≥18 years of age; (ii) postoperative application of analgesic pump; (iii) American Society of Anesthesiologists grade I–II. The exclusion criteria were as follows: (i) patients with a history of nausea or vomiting within 24 h prior to surgery; (ii) use of antiemetic drugs within 24 h prior to surgery. The reporting of this study conforms to STROBE guidelines. 12
The Medical Ethics Committee of Sun Yat-sen University Cancer Centre approved this study (no. B2021-252-01). All procedures performed in this study involving human participants were in accordance with the ethical standards of the Medical Ethics Committee of Sun Yat-sen University Cancer Centre, followed the 1964 Helsinki Declaration and its later amendments. Verbal informed consent to review the medical data was obtained from all patients.
Data collection
The clinical characteristics of patients including sex, age at diagnosis, body mass index (BMI), history of smoking, intraoperative anaesthesia, surgical approach, surgery duration, constituents of analgesic pump, routine postoperative administration of parecoxib, temporary postoperative administration of opioids, postoperative prophylactic administration of dolasetron, as well as PONV within 72 h postoperatively were collected.
Anaesthetic and analgesic use
All patients received general anaesthesia. Since remifentanil and cisacutronium were intraoperatively used as analgesic and muscle relaxant in all patients, intraoperative anaesthesia was determined by the types of anaesthetics. For patients receiving intravenous anaesthesia, propofol was used only as the anaesthetic. Patients receiving inhalational anaesthesia were those receiving sevoflurane or desflurane as the anaesthetic. Combined use of propofol and sevoflurane or desflurane was defined as combined anaesthesia. Surgical approaches were thoracotomy and video-assisted thoracoscopic surgery (VATS).
Analgesic pumps containing dezocine (0.02 mg/kg per h), dexmedetomidine (100 μg), flurbiprofen axetil (200 mg) and palonosetron (0.45 mg) were administrated in continuous infusion mode in all patients within 48 h postoperatively. Despite the routine application of analgesic pumps, some patients still needed additional analgesics to achieve satisfactory pain relief. Parecoxib, a cyclooxygenase-2 selective inhibitor and approved for short-term perioperative pain control, was routinely administered with the dosage of 40 mg every 12 h in certain patients. Weak or strong opioids were temporarily administered when patients suffered a sharp pain. Dolasetron, a highly selective 5-HT3 receptor antagonist, which exerts a powerful antiemetic effect by blocking 5-HT3 receptors, was prophylactically administered with the dosage of 25 mg or 100 mg once a day in certain patients based on the personal preference of doctors.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). The associations between PONV and the clinical characteristics of patients were analysed by χ2-test and binary logistic regression models. The strength of the associations was assessed according to odds ratio (OR) with 95% confidence intervals (CI). A P-value <0.05 was considered statistically significant.
Results
After applying the inclusion and exclusion criteria, this retrospective study included 203 patients (106 [52.2%] males) in the analyses. The clinical characteristics of the patients are summarized in Table 1. Patients ranged in age from 22 to 83 years, with 119 (58.6%) being younger than 60 years, which is the cut-off between middle age and old age for Chinese individuals. The BMIs of 133 (65.5%) patients were <24 kg/m2, which is the cut-off between normal and overweight physique for Chinese individuals. The majority of patients did not have a history of smoking. For intraoperative anaesthesia, 34 (16.7%), 100 (49.3%) and 69 (34.0%) patients received intravenous, inhaled and combined anaesthesia, respectively. A total of 110 (54.2%) patients underwent thoracotomy and 93 (45.8%) underwent VATS. The surgery duration of 133 (65.5%) patients was <120 min. A total of 80 (39.4%) patients received routine administration of parecoxib postoperatively. Weak and strong opioids were temporarily administrated in 35 (17.2%) and 53 (26.1%) patients, respectively. A total of 107 (52.7%) and 38 (18.7%) patients received prophylactic administration of dolasetron with the dosage of 25 mg and 100 mg once a day, respectively.
Clinical characteristics of the patients (n = 203) that had undergone lobectomy for lung cancer and were enrolled in this retrospective study to investigate the incidence and risk factors of postoperative nausea and vomiting.

Data presented as n of patients (%).
aP < 0.001 for between-group comparison, χ2-test; all other comparisons were not significant (P ≥ 0.05).
VATS, video-assisted thoracoscopic surgery.
The characteristics of BMI, intraoperative anaesthesia, surgical approach and surgery duration were comparable between male and female patients (Table 1). The proportions of male patients that were elderly, had histories of smoking, postoperatively received routine administration of parecoxib and prophylactic administration of dolasetron (100 mg, once a day) were higher than those in females. A significant difference was only found for a history of smoking (P < 0.001).
Postoperative nausea and vomiting occurred in 60 (29.6%) of 203 patients within 72 h postoperatively (Table 2). χ2-test showed that sex, history of smoking, surgical approach and postoperative prophylactic administration of dolasetron had significantly different incidences of PONV (P < 0.05 for all comparisons). PONV occurred in 41 of 97 (42.3%) female patients, while it only occurred in 19 of 106 (17.9%) male patients (P < 0.001). PONV occurred in eight of 54 (14.8%) and 52 of 149 (34.9%) of patients with and without a history of smoking, respectively (P = 0.006). It should be noted that of the 54 patients with a history of smoking, 53 were male and one was female. The rates of PONV in patients that underwent thoracotomy and VATS were 35.5% (39 of 110 patients) and 22.6% (21 of 93 patients), respectively (P = 0.045). Patients that received prophylactic dolasetron had a significantly lower rate of PONV than those that did not (P = 0.002).
Incidence of postoperative nausea and vomiting (PONV) in the patients (n = 203) that had undergone lobectomy for lung cancer and were enrolled in this retrospective study to investigate the incidence and risk factors of PONV.

Data presented as n of patients (%).
aCategorical data were analysed by χ2-test; NS, not significant (P ≥ 0.05).
VATS, video-assisted thoracoscopic surgery.
A binary logistic regression model of PONV demonstrated that female patients were significantly more likely to suffer PONV than males (OR 2.391; 95% CI 1.030, 5.551; P = 0.043) (Figure 1). Similarly, the risk of PONV in patients undergoing thoracotomy was significantly higher than that in patients undergoing VATS (OR 3.049; 95% CI 1.126, 8.259; P = 0.028). Postoperative prophylactic administration of dolasetron (100 mg, once a day) significantly lowered the risk of PONV (OR 0.179; 95% CI 0.034, 0.943: P = 0.042), while the risk of patients that were prophylactically administrated dolasetron (25 mg, once a day) was not significantly different from those patients that did not receive dolasetron (OR 1.270; 95% CI 0.445, 3.624). Age, BMI, history of smoking, intraoperative anaesthesia, surgery duration, routine postoperative administration of parecoxib and temporary postoperative administration of opioids were not significantly correlated with PONV.
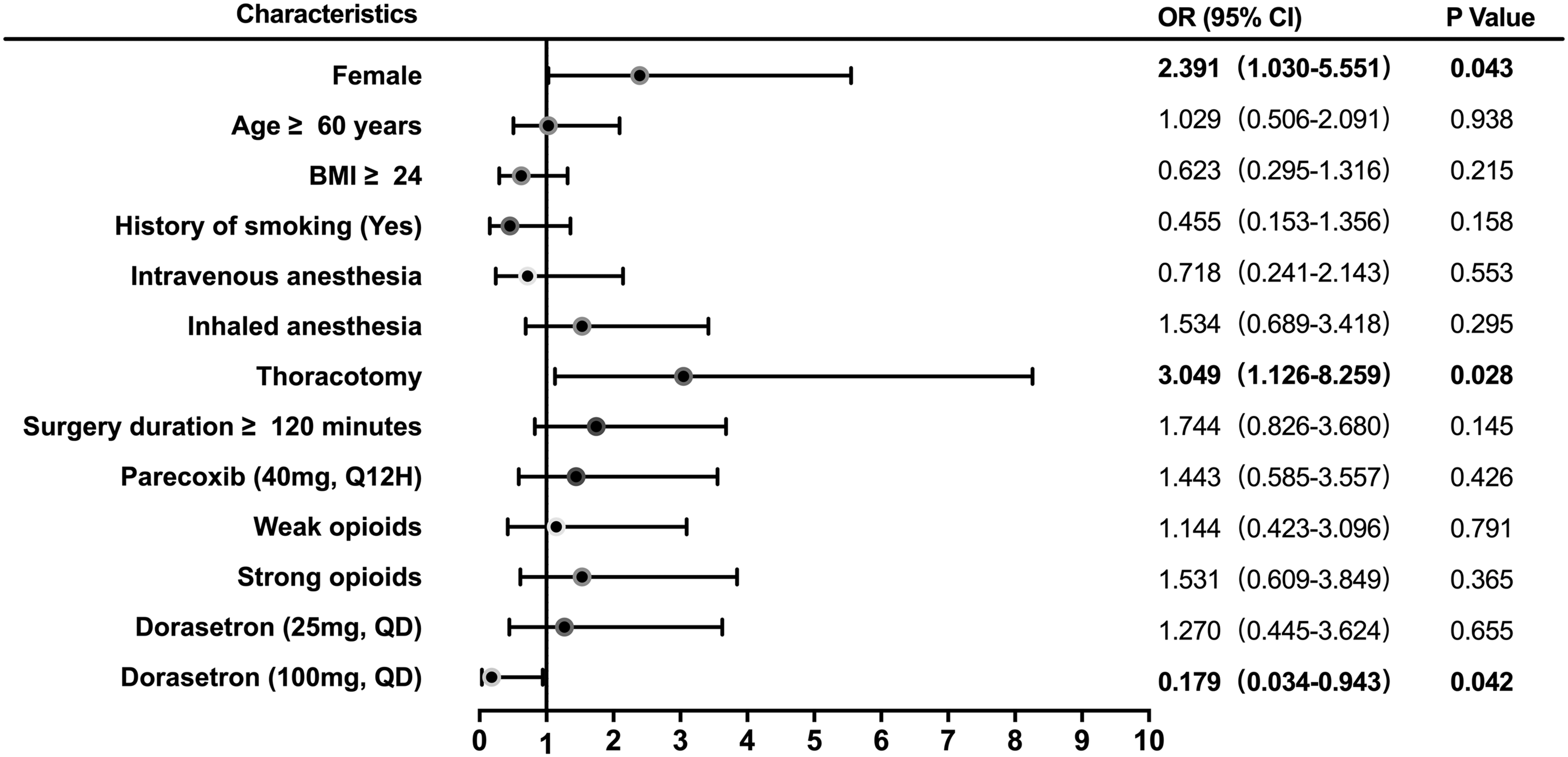
Binary logistic regression model of postoperative nausea and vomiting (PONV) in all patients (n = 203) that had undergone lobectomy for lung cancer and were enrolled in this retrospective study to investigate the incidence and risk factors of PONV. OR, odds ratio; CI, confidence interval; BMI, body mass index; Q12H, every 12 h; QD, once a day.
Given the susceptibility of female patients to PONV, the risk factors of PONV in female patients was further analysed. Since only one female patient had a history of smoking, this characteristic was not included into the binary logistic regression model. Female patients undergoing thoracotomy were significantly more susceptible to PONV than those undergoing VATS (OR 7.770; 95% CI 1.747, 34.568; P = 0.007; Figure 2). The risk of PONV was also significantly higher in female patients with surgery durations ≥120 min (OR 4.493; 95% CI 1.502, 12.851; P = 0.007). The risk of female patients that postoperatively received prophylactic administration of dolasetron (100 mg, once a day) was significantly lower than those that did not receive dolasetron (OR 0.075; 95% CI 0.007, 0.834; P = 0.035). There was no significant association between PONV and age, BMI, routine postoperative administration of parecoxib and temporary postoperative administration of opioids.

Binary logistic regression model of postoperative nausea and vomiting (PONV) in female patients (n = 97) that had undergone lobectomy for lung cancer and were enrolled in this retrospective study to investigate the incidence and risk factors of PONV. OR, odds ratio; CI, confidence interval; BMI, body mass index; Q12H, every 12 h; QD, once a day.
To compare male and female patients, the risk factors of PONV in male patients was further analysed. In the binary logistic regression model, the risk of PONV was significantly lower in male patients with a BMI ≥24 kg/m2 than in those with a BMI < 24 kg/m2 (OR 0.166; 95% CI 0.035, 0.782; P = 0.023; Figure 3). There was no significant association between PONV and any of the other clinical characteristics in male patients, including surgery approach, surgery duration and postoperative prophylactic administration of dolasetron, which were significantly correlated with PONV in female patients.

Binary logistic regression model of postoperative nausea and vomiting (PONV) in male patients (n = 106) that had undergone lobectomy for lung cancer and were enrolled in this retrospective study to investigate the incidence and risk factors of PONV. OR, odds ratio; CI, confidence interval; BMI, body mass index; Q12H, every 12 h; QD, once a day.
Discussion
The incidence of PONV ranges from 20–30% in most studies.3,6,13 Based on the postoperative application of analgesic pumps containing dezocine, dexmedetomidine, flurbiprofen and palonosetron, 29.6% of patients following lobectomy for lung cancer experienced PONV in the present study.
The formula of analgesic pumps is commonly based on opioids in order to provide powerful and continuous management of severe postoperative pain. Dezocine, a synthetic opioid agonist-antagonist that is slightly more potent than morphine but with similar adverse effects, 14 is used as the basic constituent of analgesic pumps in our centre. In addition to dezocine, dexmedetomidine, flurbiprofen and palonosetron were also added into the analgesic pumps. Both dexmedetomidine and flurbiprofen were reported to have the effects of enhancing analgesia and reducing PONV15–19 and to be used in analgesic pumps. 20 Palonosetron is a potent and highly selective serotonin 5-HT receptor antagonist that has been commonly used to prevent nausea and vomiting caused by chemotherapy or surgery. 21 Despite the routine application of analgesic pumps, some patients still needed additional analgesics to achieve satisfactory pain relief in the current study. Nevertheless, additional analgesics, including the routine administration of parecoxib and the temporary administration of opioids, did not increase the risk of PONV in the current study.
Consistent with the results reported in previous studies,5–7, 22–24 the current study found that female patients were more likely to suffer with PONV than males. The reason for the increased susceptibility of women to PONV remains unclear. It is believed that the fluctuation in oestrogen levels may be an important cause of PONV. 21 PONV increases as girls approach menarche and the incidence in postmenopausal females is similar to that of men suggesting a major hormonal influence.25,26 A previous study found that the incidence of PONV was the highest on the 5th day of menstruation and the lowest on the 18th to 20th day, which also suggests that the occurrence of PONV is related to the fluctuation of oestrogen and progesterone in the body. 27 Similarly, the onset of morning sickness is associated with fluctuations in oestradiol levels in pregnant women. 28
In addition to females having a higher rate of PONV, the current study also found that the risk factors of PONV in female patients were different to those in male patients. The risk of PONV in female patients undergoing thoracotomy or those with a surgery duration ≥120 min was higher than that in patients undergoing VATS or those with a surgery duration <120 min. Vomiting is theoretically caused by stimulating peripheral receptors with neurotransmitters such as acetylcholine, histamine, dopamine, norepinephrine, epinephrine and 5-HT.29,30 Among these neurotransmitters, the effect of 5-HT is the most significant. 31 Since mechanical stimuli were one of the factors that could lead to 5-HT exocytosis, 32 the more mechanical stimuli experienced by patients undergoing thoracotomy or a longer surgery duration might account for their higher risk of PONV compared with those undergoing VATS or those with a shorter surgery duration.
Although palonosetron, a potent 5-HT receptor antagonist, had been added to the analgesic pumps in the current study, postoperative prophylactic administration of dolasetron (100 mg, once a day) significantly reduced the risk of PONV in female patients. It is worth noting that the risk of patients prophylactically administrated dolasetron (25 mg, once a day) was not significantly different from those without administration of dolasetron. These results indicate that large doses of 5-HT receptor antagonist could be considered to protect female patients from PONV. The sex disparity in the prophylactic role of dolasetron on PONV has been reported previously. For example, in a pooled analysis of three large clinical trials, administration of dolasetron near the end of general anaesthesia effectively protected female patients from PONV within 24-h monitoring periods. 33 However, male patients did not benefit from dolasetron. 33 The sex disparity in the susceptibility to PONV may account for the distinct effect of dolasetron on prophylaxis for PONV. Moreover, previous studies also analysed the effective dolasetron dose for prevention of PONV during the initial 24 h after surgery.33–35 In female patients undergoing total abdominal hysterectomy under general anaesthesia, dolasetron 100 mg administrated 1 or 2 h before induction of anaesthesia provided more effective prophylaxis for PONV than 25 mg. 35 In female patients undergoing a variety of surgical procedures under general anaesthesia, dolasetron 12.5 mg given near the end of anaesthesia was the maximally effective dose for preventing PONV and no increased efficacy was observed with dolasetron doses higher than 12.5 mg.33,34 In the present study, dolasetron was prophylactically administered with the dosage of 25 mg or 100 mg once a day in certain patients; and only dolasetron (100 mg, once a day) significantly reduced the risk of PONV in female patients. Compared with patients reported in previous studies,33–35 all of the patients in the present study underwent pulmonary lobectomy and postoperative application of analgesic pumps. Meanwhile, PONV was monitored during the 72 h after surgery due to the application of analgesic pumps during this period. The surgical procedure and application of analgesic pumps might influence the effective dolasetron dose for preventing PONV.
In male patients, BMI was the only factor that was associated with PONV. The role of BMI on PONV remains controversial. Early studies that were mainly undertaken in Caucasians reported that BMI was positively associated with the occurrence of PONV.5,36–39 However, several studies that were carried out in East Asians have recently found the opposite results.20,40–43 A large-scale study including 103 561 patients in Korea showed that a higher-than-normal BMI reduced the risk of PONV after general anaesthesia. 41 In accordance with this result, the current study found that overweight male patients would experience less PONV than normal-BMI or underweight male patients. The mechanism underlying this phenomenon has not yet been clarified, but histamine and dopamine may play roles. As aforementioned, receptors and pathways that mediate nausea and vomiting are able to be stimulated by neurotransmitters, including histamine and dopamine.29,30 During perioperative fasting, the amount of hypothalamic histamine would be significantly reduced in overweight patients compared with patients of normal or lower weight because leptin facilitating histamine release from the hypothalamus decreased more significantly in overweight patients.44,45 Meanwhile, overweight patients have fewer dopamine receptors than those with normal BMI,46,47 indicating less effect of dopamine for PONV on overweight than normal-BMI patients.
This current study had several limitations. First, the significance was limited by the retrospective design. Secondly, only clinical factors that were recorded in the medical records were included in the analyses. Some clinical factors that were reported to be associated with PONV, such as a history of motion sickness or gastrointestinal discomfort, were not included due to incomplete records. Therefore, the risk factors determined in the binary logistic regression models were insufficient to establish a predictive model for PONV because the c-statistic of the receiver operating characteristic curve was <0.7 (data not shown). Thirdly, there was no set protocol for anaesthesia, analgesia or antiemetics in this study. Perioperative management was more varied than in a planned prospective study, which may undermine the interpretation of the current results. Meanwhile, the results in this current study were based only on the analgesic method used. The constituents of the analgesic pump usually vary from centre to centre, which may result in different incidences and risk factors of PONV. Large prospective studies are warranted to obtain more comprehensive results about PONV in lung cancer patients.
In conclusion, this current study demonstrated different rate and risk factors of PONV in female and male patients following lobectomy for lung cancer and the postoperative application of analgesic pumps. The incidence of PONV in female patients was significantly higher than that in male patients. Thoracotomy and a surgery duration ≥120 min significantly increased the risk of PONV in female patients, while prophylactic administration of dolasetron (100 mg, once a day) significantly lowered the risk. For male patients, the risk of PONV was significantly lower in patients with a BMI ≥ 24 kg/m2 than in those with a BMI < 24 kg/m2. These results will facilitate the development of personalized treatment management to protect patients from this frequent and debilitating symptom.
Footnotes
Acknowledgement
We thank the patients and their families for their participation and contribution to the project.
Author contributions
S.W., C.G. and X.H. collated and analysed the data, and drafted the paper. D.J., Y.X., F.M., Y.L. and Y.H. collated data. H.D. and P.L. contributed to the study design and ethics committee submission. All authors approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Guangdong Basic and Applied Basic Research Foundation (no. 2020A1515110069).