
Abstract
Objectives
This study aimed to evaluate the effects of external diaphragmatic pacing (EDP) on patients with chronic cor pulmonale (CCP).
Methods
Fifty patients with CCP were enrolled in Kashgar Prefecture Second People’s Hospital in Xinjiang Uygur Autonomous Region of China from 2016 to 2017. The patients were randomized into a group that received anti-CCP therapy (negative control group) or a group that received additional EDP treatment (EDP group). We recorded and compared maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC, and the 6-minute walking test between the two groups on the first and tenth days of treatment.
Results
Ten days after treatment began, MIP, FVC, and the 6-minute walking test were significantly improved in both groups. Importantly, MIP and FVC were significantly higher in the EDP group compared with the control group on the tenth day.
Conclusion
In addition to treatment for CCP, these patients can obtain extra benefit by using EDP treatment.
Keywords
Introduction
Chronic cor pulmonale (CCP) is a major public health problem globally. Pulmonary hypertension (PH) is the underlying mechanism of CCP, which leads to heart failure. 1 Meyer et al. 2 found inspiratory and expiratory muscle weakness in patients with PH, and the maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) were significantly reduced owing to PH. A reduction in MIP in heart failure is common and is an independent predictor of death related to CCP. 3
The diaphragm is the major respiratory muscle. However, de Man 4 et al. found weakness of diaphragm muscle fibers in patients with PH. In intubated patients, diaphragmatic thickness decreases over time and a low diaphragmatic contractile activity is associated with rapid decreasing. 5 These findings suggest that physical activity can strengthen the diaphragm, similar to the function of exercise on skeletal muscle. In several conditions, patients can achieve a benefit from diaphragmatic pacing. An example of one of these conditions is that a patient with life-threatening PH achieved satisfactory ventilation after inserting an intradiaphragmatic phrenic nerve stimulator. 6 Diaphragmatic pacing can provide long-term and stable respiratory support in patients with respiratory failure caused by high spinal cord injury. 7 Additionally, this pacing improves periodic breathing, gas exchange, sleep architecture, and quality of life in patients with atrial fibrillation and Cheyne–Stokes respiration. 8
Although an implanted diaphragmatic pacemaker is effective, it is invasive and expensive, and leads to a high risk of infection, dislocation, scarring, shoulder pain, and chronic use of analgesics. External diaphragmatic pacing (EDP) is an alternative to stimulate the diaphragm. EDP is a non-invasive procedure to avoid the risk of surgical implantation and is a more effective way of breathing muscle training because the diaphragm contracts and relaxes regularly after EDP. This clinical study aimed to evaluate the effects of EDP on patients with CCP.
Methods
Design
This study was a randomized, controlled trial, which followed the principles of the Declaration of Helsinki. This study was approved by the institutional Review Board of Kashgar Prefecture Second People’s Hospital (serial number: 2016-09-07). All patients received detailed information and provided written informed consent by themselves or from their immediate family members if patients were not able to provide informed consent. The trial registration number was NCT02976324 (registered on November 24, 2016; https://clinicaltrials.gov/ct2/show/NCT02976324?term=NCT02976324&draw=2&rank=1).
Participants, therapists, and centers
Eighty patients of Uighur nationality who were diagnosed with CCP in the Second People’s Hospital in Kashgar Prefecture, Xinjiang Uygur Autonomous Region of China (2016-2017) were selected for our study. The patients were randomly allocated by using a number system (odd numbers in the EDP group and even numbers in the negative control [NC] group). Thirty patients were excluded because they were unable to tolerate the treatment for CCP.
The diagnosis of CCP was based on the following criteria: 1) chronic pulmonary disease or pulmonary vascular disease, mainly based on medical history, physical signs, an electrocardiogram (ECG), X-ray, radioisotopes, echocardiography, and pulmonary function; 2) right heart dysfunction, such as engorgement of the jugular vein, severe swelling of the liver, positive hepatojugular reflux sign, lower extremity edema, and increased venous pressure; and 3) right ventricular enlargement according to physical signs, X-ray, echocardiography, ECG, or a radioisotope examination. PH was diagnosed by echocardiography using the following criteria. If the patient’s right ventricle was not enlarged and the estimated pulmonary artery systolic pressure was equal to the tricuspid regurgitation pressure difference plus 8 mmHg, which was greater than 30 mmHg, the patient was diagnosed with PH. If the patient’s right ventricle was enlarged and the estimated pulmonary artery pressure was equal to the tricuspid regurgitation pressure difference plus 10 mmHg, which was greater than 30 mmHg, the patient was diagnosed with PH. Adult patients (aged between 18 and 70 years) who met the above-mentioned diagnosis and required hospitalization were finally enrolled in this study.
The exclusion criteria included the following: 1) pneumothorax or mediastinal emphysema; 2) active tuberculosis; 3) pacemakers were installed; 4) presence of acute cardiovascular and cerebrovascular events, such as acute myocardial infarction, acute myocarditis, severe arrhythmia, and severe cerebrovascular accidents; 5) pregnancy; and 6) end-stage patients (e.g., patients with advanced malignant tumors).
Intervention
For the EDP group, in addition to usual standard treatment and care, the patients received electrode patches for EDP that were attached to the patient’s neck and chest according to the product manual of EDP that we used (Guangzhou Arahelio Biotechnology, HLO-GJ13A).
Briefly, regarding the procedure, after cleaning the skin, a small electrode was attached to the distal one third of the outer edge of the sternocleidomastoid muscle. A large electrode was attached to the second intercostal space along the middle clavicular line. The diaphragm was paced nine times per minute with a stimulus frequency of 40 Hz for 30 minutes each time, twice a day. The stimulation intensity was set as high as possible if the patient could tolerate it.
For the NC group, the patients received standard treatment, including oxygen, diuretics, anticoagulant and calcium antagonists, and other treatment prescribed by the clinical attending physician on the basis of clinical norms and the corresponding diagnosis and treatment guidelines.
Outcome measures
Data of MIP, MEP, forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC, and the 6-minute walking test (6MWT) were recorded on the first and tenth days of treatment by the attending physicians.
Data analysis
Study variables are shown as mean ± standard deviation. Comparisons of the outcomes between the intervention and control groups and between the first and tenth days of treatment were made using the Student’s t test or chi-square test using SPSS for Windows, version 16.0 (SPSS Inc., Chicago, IL, USA). Only P values <0.01 were considered significant.
Results
Participants, therapists, and centers in the study
Fifty patients were eligible for the study. Among them, 26 patients were enrolled in the EDP group and 24 in the control group. A flowchart of the study is shown in Figure 1.

Flowchart of participating patients in the study.
There were no significant differences in sex, age, body mass index (BMI), MIP, MEP, FEV1, FVC, FEV1/FVC, and the 6MWT distance at the first day of treatment (Table 1).
Patients’ information in the EDP and NC groups.

Data are shown as mean ± standard deviation.
EDP, external diaphragmatic pacing; NC, negative control; BMI, body mass index; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; 6MWT, 6-minute walking test.
Comparison of patients’ outcomes between days 1 and 10 of treatment within the groups
In the NC group 10 days after beginning treatment, MIP, FEV1, FVC, and the 6MWT distance were significantly increased compared with those on the first day (all P < 0.01). However, MEP and FEV1/FVC were not significantly different between 1 and 10 days of treatment (Table 2).
Comparison of variables between the first and tenth days in the negative control group.

Data are shown as mean ± standard deviation.
MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; 6MWT, 6-minute walking test.
Similar to the NC group, in the EDP group, MIP, FEV1, FVC, and the 6MWT distance were significantly increased at 10 days of treatment compared with those on the first day (all P < 0.01). There were no significant differences in MEP and FEV1/FVC between 1 and 10 days of treatment (Table 3).
Comparison of variables between the first and tenth days in the external diaphragmatic pacing group.

Data are shown as mean ± standard deviation.
MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; 6MWT, 6-minute walking test.
Comparison of patients’ outcomes between the two groups
At 10 days of treatment, we found that MIP and FVC were significantly higher in the EDP group compared with the NC group (both P < 0.001). There were no significant differences in MEP, FEV1, FEV1/FVC, and the 6MWT distance at 10 days of treatment between the two groups (Table 4).
Comparison of the change in variables between the tenth and first days between the EDP and NC groups.
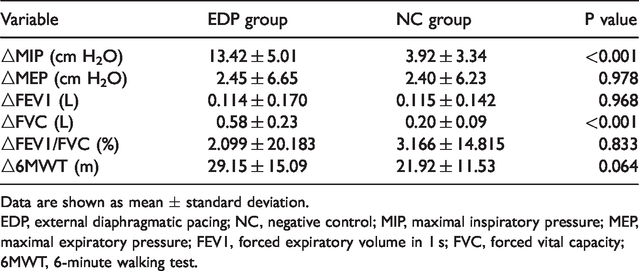
Data are shown as mean ± standard deviation.
EDP, external diaphragmatic pacing; NC, negative control; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; 6MWT, 6-minute walking test.
Discussion
Diaphragmatic pacing therapy is mostly used in patients with cervical spinal cord injury by an invasive surgery, and patients can obtain satisfactory outcomes to some extent. 9 Although respiratory muscle function is significantly impaired in patients with PH,2,4 few reports have focused on non-invasive EDP treatment in those patients. 10 Our clinical trial suggests that patients with CCP can obtain extra benefits from EDP.
To examine potential bias in patients with CCP at baseline, we compared age, sex, BMI, MIP, MEP, FEV1, FVC, FEV1/FVC, and the 6MWT between the EDP and NC groups. We did not find any significant differences in these measures between the groups at baseline (Table 1). MIP and MEP are the most commonly used clinical measures for assessing respiratory muscle strength 11 , 12 in accordance with the protocol issued by the American Thoracic Society/European Respiratory Society.13,14 In the EDP and NC groups, similar significant improvements were found in MIP, FVC, and the 6MWT (Tables 2 and 3). These results indicated that standard treatment and EDP were effective for patients with CCP. We were not able to examine the effectiveness of EDP independently from standard medical treatment for patients with CCP because of ethical reasons. We believe that EDP should be performed in addition to standard medical treatment for patients with CCP.
Several randomized trials have shown that, even for elderly intubated patients, who are mechanically ventilated for at least 48 hours, inspiratory muscle training improves their MIP,15–17 and even increases patients’ quality of life. 18 To understand the therapeutic effects of EDP therapy on patients with CCP, we compared various parameters between the two groups 10 days after the beginning of treatment. We found that MIP and FVC in the EDP group were more significantly improved than in the NC group (Table 4). This finding suggests that EDP improves part of the patient’s respiratory function as a result of basic anti-CCP treatment, and patients can have extra benefits from using EDP. The underlying mechanism of this finding could be that short periods of daily electrical stimulation of the phrenic nerve can significantly improve patients’ tidal volume. 19 In the case of respiratory muscle fatigue, enhancement of diaphragmatic function can partially resist the weakness of other respiratory muscles. 20
With regard to the safety of the electronic device for EDP, inspiratory muscle training achieved by a threshold device attached to the tracheostomy for intubated patients causes almost no adverse outcomes. 21 The device that we used in this trial is noninvasive, and it does not affect the electronic device in the intensive care unit when functioning. There is no obvious damage to the skin because the electrodes can be removed after EDP treatment. Additionally, EDP does not significantly affect hemodynamic stability and inspiration of patients. The patients can sustain stable physiological parameters in response to training under this treatment. Importantly, this external device causes little discomfort. However, for patients with pneumothorax and active tuberculosis, EDP is not recommended. Patients with a cardiac pacemaker also cannot receive EDP treatment because of the potential risk of arrhythmia.
There are several limitations in this study. First, we were unable to determine the underlying mechanism of EDP’s effects on patients because similar studies have suggested that the diaphragmatic pacemaker protects the diaphragm from metabolic disturbances, decreases oxidative stress levels, and upregulates autophagy.22,23 Second, we did not test the feasibility of EDP on patients who were inserted with a cardiac pacemaker because there could be cross-talk inhibition between diaphragmatic and cardiac pacemakers. However, despite electrical inference from repetitive diaphragmatic pacing, cardiac pacemaker functions are unaffected.24,25
Conclusions
This study suggests that EDP is a noninvasive procedure that can stimulate the phrenic nerve to strengthen the diaphragm to improve respiratory function in patients with CCP compared with standard anti-CCP treatment. The study demonstrates that patients with CCP can obtain extra benefits by using EDP treatment.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the National Natural Science Foundation of China (Grant nos: 81702842 and 81871540), the Shanghai Sail Plan for Talents Development (Grant no: 17YF1415000), the Construction Plan of Important and Weak Disciplines of Shanghai Health Commission (Grant no: 2016ZB0204-01), and the Shanghai Science and Technology Development Funds (Grant no: 18RZ1429500).