
Abstract
Objective
The number of patients with metastatic bone tumors of the pelvis (MBTP) has increased, and the risk of metastasis and recurrence in the pelvic bones is difficult to assess. Therefore, we investigated the clinical features and oncological outcomes of patients with MBTP.
Methods
We analyzed the clinical features and oncological outcomes of MBTP in 72 patients (42 men, 30 women; mean age, 50.5 years) from 2008 to 2017. Recurrence in the pelvic bones and survival rates were analyzed with regard to patients’ potential contributing factors.
Results
Enneking region I was the area most commonly containing MBTP (47.3%). Low- and high-grade tumors were identified in 40 and 32 patients, respectively. The most common pathological type was adenomatous carcinoma (34.7%), and the most common primary lesion was lung cancer (20.8%). The 3-year overall recurrence rate within the pelvic bones was 34.7%, and the 5-year overall survival rate was 29.2%.
Conclusion
Patients with MBTP have a high risk of recurrence in the pelvic bones and poor survival after multimodal treatment. Pelvic recurrence might be affected by the metastatic involvement, tumor grade, surgical margins, and type of surgery, whereas the survival rate tends to be associated with the tumor grade.
Introduction
The number of patients with metastatic bone tumors of the pelvis (MBTP) is rising with advances in multimodal treatment of primary lesions.1,2 MBTP are one of the most common metastases after spinal metastases. 1 MBTP usually produce significant pain, severe disability, and poor quality of life as a result of pathologic fractures, anemia, and hypercalcemia. Destruction of the pelvic bones by metastases is a common problem encountered in clinical oncology. 2 Involvement of multiple pelvic bones is often seen; however, published articles concerning MBTP are still controversial. Additionally, recurrence in the pelvic bones remains a difficult and unpredictable problem in clinical oncology.3,4 In the present study, we examined the clinical features, oncological outcomes, and factors contributing to recurrence in the pelvic bones and survival of patients.
Patients and methods
Patients
Records of patients with metastatic bone tumors were retrospectively reviewed in the Bone Tumor Research Institute of Shanghai. The records of patients with MBTP from January 2008 to March 2017 were included in the present study. All patients’ primary lesions were in remission after multimodal treatment. Clinical information including age, sex, pelvic metastatic sites, tumor size, tumor histology, tumor grade, primary lesions, radiographic findings, treatment, and oncological outcomes was collected. To construct a homogeneous study series, the following exclusion criteria were applied: remote history of cancer with bone metastasis, pelvic metastasis as the initial symptom, insufficient information from the medical record, and treatment for primary lesions. Seventy-two patients with MBTP were included in the present study.
This study was approved by the Ethical Committee of Qingpu Branch of Zhongshan Hospital affiliated to Fudan University (ECQBZH No. 2007-15) (Shanghai, P.R. China). The requirement for informed consent was waived by the board.
Methods
MBTP were diagnosed with consideration of the patients’ primary lesion history, clinical presentation, radiological findings, and pathological analysis, which were retrieved from the registry of the Bone Tumor Research Institute of Shanghai. All patients’ primary lesions were in remission. The clinical presentation of MBTP included patients’ symptoms and decreased range of motion. All patients’ imaging findings, including X-ray, computed tomography, and magnetic resonance imaging, were obtained.
Pathological results were also obtained, including hematoxylin-and-eosin-stained specimens, tumor size, and tumor grade. Specimens gained by biopsy or surgical excision were stained with hematoxylin and eosin. The size of MBTP was calculated according to Bieling et al. 5 The tumor grade was determined based on the four-point grading system for bone tumors. 6 Grade 1 and 2 tumors were considered low-grade, and grade 3 and 4 tumors were considered high-grade. The types of surgery were classified as curettage, marginal resection, and wide en bloc resection. 7 Using previously described methods, surgical margins were classified as adequate, inadequate, or intralesional 8 and as R0, R1, or R2. 9 Recurrence in the pelvic bones and survival rates were analyzed with regard to patients’ potential contributing factors.
The Eastern Cooperative Oncology Group performance status (ECOG-PS) scores, which were used to evaluate the functional outcomes of patients with MBTP, were also retrieved. 10
Statistical analysis
The chi-square test or Fisher’s exact test was performed for comparisons of proportions. Mantel–Haenszel analysis was performed for comparison of ranked variables. Kaplan–Meier analysis was used to describe survival among the study population. The above tests were used for univariate analysis, and multivariate analysis was performed as follows: logistic regression was used to identify the risk factors for recurrence in the pelvic bones at 3 years, and Cox regression was performed to identify factors associated with the 5-year survival rate. All statistical analyses were performed using SAS version 9.1 (SAS Institute, Cary, NC, USA). A P value of <0.01 was considered to indicate a statistically significant difference.
Results
Patients and pathology
Seventy-two patients with MBTP were identified among 530 patients with bone metastases, accounting for 13.6% (Table 1). The patients comprised 42 men and 30 women with a mean age of 50.5 years (range, 14–73 years). The most commonly involved site was the ilium (n = 35, 48.6%), which is defined as Enneking region I. 11 There were 66 (94.6%) patients with solitary MBTP and 6 (5.4%) patients with multiple MBTP.
Characteristics of patients with metastatic bone tumors of the pelvis.
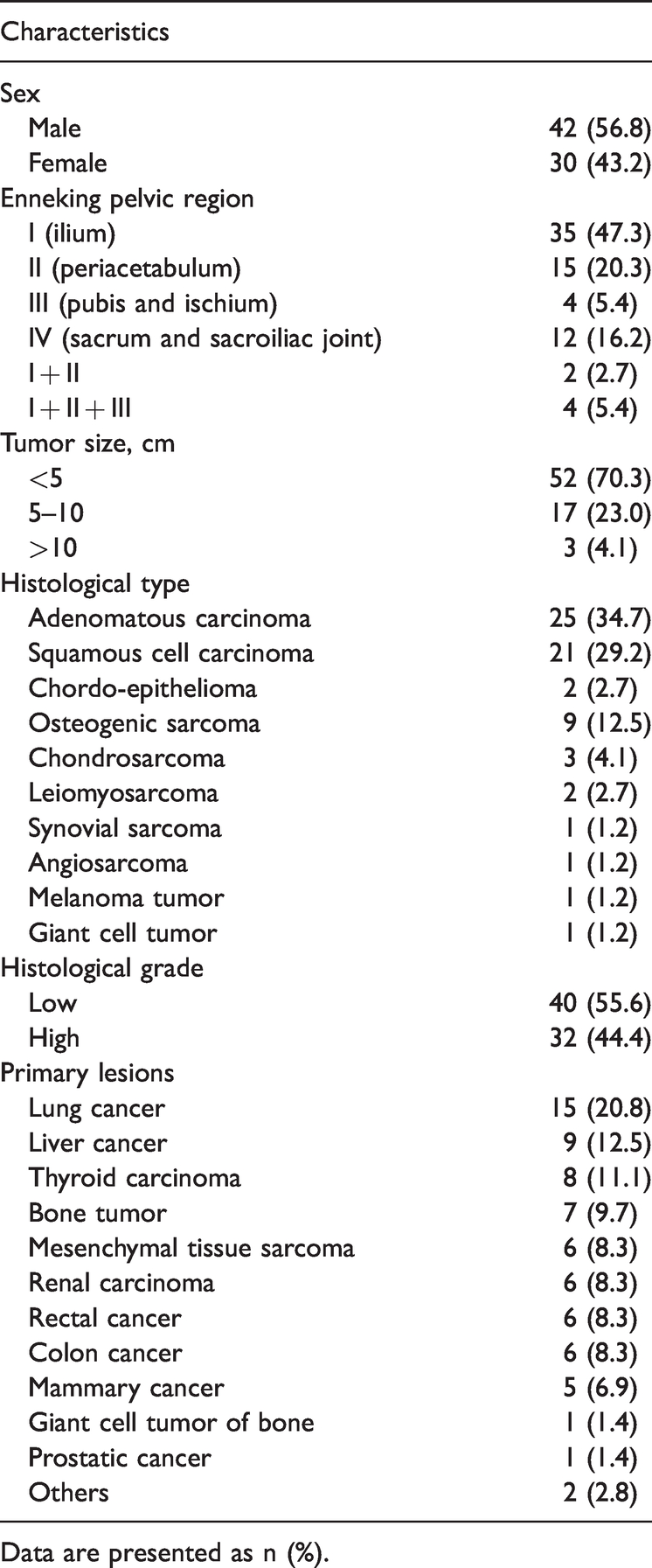
Data are presented as n (%).
All 72 patients’ pathological grades and types were identified. Low-grade tumors were found in 40 (55.6%) patients, and high-grade tumors were found in 32 (44.4%). The most common pathological type was adenomatous carcinoma (n = 25, 34.7%), followed by squamous cell carcinoma (n = 21, 29.2%) and osteogenic sarcoma (n = 9, 12.5%). The most common primary lesions were from the lung (n = 15, 20.8%), followed by the liver (n = 9, 12.5%) and thyroid (n = 8, 11.1%).
Treatment and follow-up
Surgical treatment was performed in 44 (61.1%) patients with consideration of the patients’ general condition, tumor characteristics, and predicted benefits (Table 2). The preferred type of surgery was curettage/marginal resection in 17 (38.6%) of 44 patients and wide en bloc resection in 27 (61.4%) patients. During the surgery, reconstruction was performed in 14 (31.8%) of 44 patients and semi-pelvis replacement in 4 (9.1%) patients. The surgical margin status was R0, R1, and R2 in 27, 16, and 1 patient, respectively, which was verified to be consistent with the type of surgery. For inadequate margins (R1 and R2), radiotherapy (n = 7) and chemotherapy (n = 9) were indicated to decrease the high risk of recurrence in the pelvic bones.
Clinical outcomes of metastatic bone tumor of pelvis.

Data are presented as n (%).
ECOG-PS: Eastern Cooperative Oncology Group performance status.
The remaining 28 patients were treated conservatively. Twenty-two patients received chemotherapy according to the NECO-95J protocol, 12 and six patients received radiotherapy as a palliative treatment. 13
The mean follow-up was 5.6 years (range, 2–8 years). In total, 71 and 21 patients were alive at 6 months and 5 years, respectively. After initial treatment, all patients achieved remission. At 6 months, the ECOG-PS scores were 1, 2, 3, and 4 in 32, 28, 10, and 1 patient, respectively. At 5 years, however, the ECOG-PS scores were 1, 2, and 3 in 2, 9, and 10 patients, respectively.
Recurrence in pelvic bones
Radiography, computed tomography, and magnetic resonance imaging showed that 25 of 72 patients developed recurrence in the pelvic bones for a 3-year overall recurrence rate of 34.7%

Recurrence in the pelvic bones in different groups with regard to metastatic involvement (M: multiple, S: solitary), tumor grade (L: low, H: high), type of surgery (W: wide en bloc resection, C/M: curettage/marginal resection), and margins (R0, R1, R2) at 3 years. Significant differences were found in the recurrence rate of M (83.3%) vs. S (43.5%), C/M (88.2%) vs. W (37.0%), and R1 (87.5%) + R2 (100%) vs. R0 (37.0%) (P < 0.01).
The clinical results revealed recurrence in the pelvic bones in 10 (37.0%) patients with R0 resection, 14 (87.5%) patients with R1 resection, and 1 (100%) patient with R2 resection at 3 years. The recurrence rate in the pelvic bones was higher with R1 and R2 resection than with R0 resection (DF = 1, Value = 6.7292, P < 0.01).
Eighteen (56.3%) of 32 patients with high-grade tumors developed recurrence in the pelvic bones at 3 years, whereas 7 (17.5%) of 40 patients with low-grade tumors developed recurrence. Statistical analysis revealed that the difference between these two groups was significant (DF = 1, Value = 11.7774, P < 0.01) (Table 2).
Recurrence in the pelvic bones was compared between patients who underwent wide en bloc resection and those who underwent curettage/marginal resection. The result showed that the 3-year rate of recurrence in the pelvic bones was 88.2% after wide en bloc resection and 37.0% after curettage/marginal resection (DF = 1, Value = 11.1451, P < 0.001).
The above factors were found to be significantly different in the univariate analysis; the others were not significant. However, no factor showed a significant difference in the logistic regression analysis.
Survival
The overall survival rate for the whole series was 29.2%, and 21 patients remained alive at 5 years.
The 5-year survival rate was 56.3% in patients with low-grade tumors and 12.0% in patients with high-grade tumors, with a significant difference (DF = 1, Value = 11.8105, P < 0.001). However, survival was not significantly different between patients with multiple pelvic bone metastases (0.0%) and those with solitary metastases (31.8%) (DF = 1, Value = 2.6952). The 5-year survival rate was 55.6% in patients treated with wide en bloc resection and 35.3% in those treated with curettage/marginal resection, but the difference was not statistically significant (DF = 1, Value = 1.7166) (Figure 2
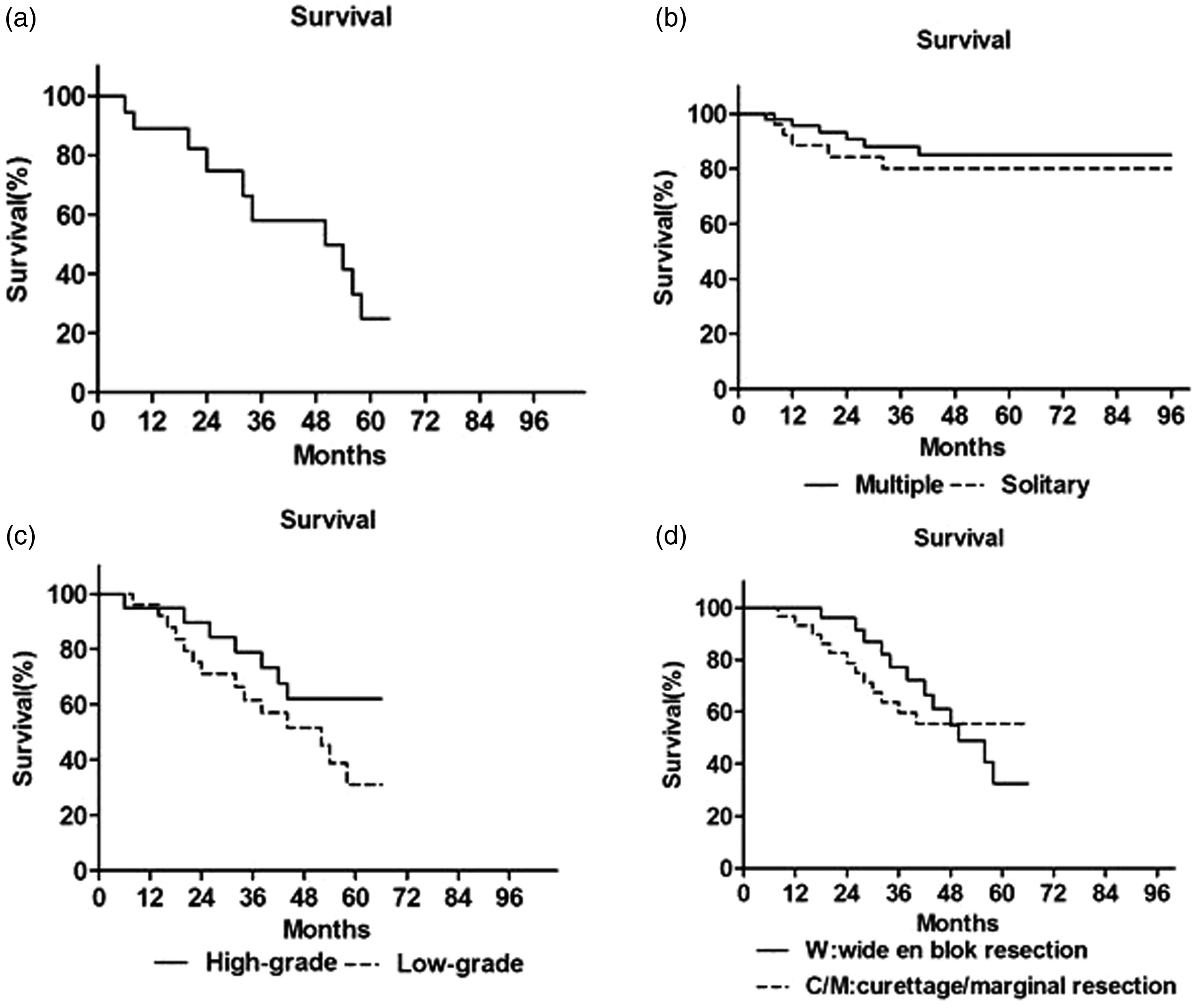
(a) The overall survival rate for the whole series was 29.2% at 5 years. (b) No significant difference was observed in patients with multiple metastases (0.0%) vs. solitary metastases (31.8%) at 5 years. (c) The survival rate differed significantly between patients with low-grade (56.3%) and high-grade (12.0%) pelvic bone metastases (P < 0.001). (d) No difference was found in the 5-year survival rate between wide en bloc resection and curettage/marginal resection.
Discussion
Clinical outcomes of patients with MBTP have improved with the development of multimodal treatment and persistent investigations. In the present study, we determined the clinical features and oncological outcomes of patients with MBTP, especially recurrence in the pelvic bones and patient survival rates.
The incidence rate of MBTP in this study was 13.6%, which is slightly lower than 18.8% 1 and 20.0% 2 in previous studies. The most commonly involved site of the pelvis was Enneking region I (48.6%), followed by Enneking region II (20.8%). These results are similar to those in a study by Picci et al. 1 Solitary metastases accounted for >90% and were the most common pelvic lesions in our study, while multiple metastases accounted for only 8.1%.
The three major pathological types were adenomatous carcinoma (34.7%), squamous cell carcinoma (29.2%), and osteogenic sarcoma (12.5%), which were helpful to find the source of the primary lesions and choose the most appropriate treatment. This factor was not associated with recurrence in the pelvic bones or survival of patients in the present study.
As reported previously,2,14 lung cancer was the most common primary lesion. Its incidence was 20.8% in the present study, which was lower than that in a study by Kim et al. (46.4%). 14
The primary functional goal of surgical treatment is to allow immediate weight-bearing. 15 Surgical treatment is recommended for patients with Capanna classes 1, 2, and 3. 16 Patients with MBTP reportedly benefit from surgical treatment in terms of pain relief, maintenance of function, and improvement in quality of life.17,18 In the present study, 44 patients underwent surgery with curettage, marginal resection, or wide en bloc resection. At the same time, pelvic reconstruction or semi-pelvis replacement was performed to ensure the integrity of the pelvic ring and allow for immediate weight-bearing. The ECOG-PS scores reflected the good results of surgical treatment. In addition, wide en bloc resection was found to have a good effect on the patients’ prognosis in this study.
Optimal outcomes in patients with MBTP still rely on multimodal treatment. We administered radiotherapy to six patients as a palliative treatment and to seven patients with inadequate surgical margins, and this treatment was quite effective in providing relief from painful bone metastasis.7,16 In our study, 9 patients received adjuvant chemotherapy before surgery 19 and 14 received chemotherapy according to the therapeutic schedule outlined in the NECO-95J protocol. 12 No complications associated with chemotherapy were observed. Additionally, interventional therapy was preferred when chemotherapy and radiotherapy failed. 20 Functional outcomes were evaluated using the ECOG-PS scores, which revealed good results at 6 months and poor results at 5 years.
The reported recurrence rate in the pelvic bones ranges from 18.8% to 47.0%.16,21–23 The recurrence rate in the present study was 34.7%, which falls within the above-mentioned range. Patients with multiple metastases had a higher rate of recurrence in the pelvic bones than those with solitary metastases; however, there was no difference in the survival rate between these two groups. Achieving adequate surgical margins is an important component of surgical treatment. 24 Surgical margins are reportedly associated with recurrence17,25; however, contrasting results have also been reported.22,23 In the present study, inadequate surgical margins (R1 and R2) resulted in a much higher (>80%) recurrence rate in the pelvic bones than did adequate surgical margins (R0). The pathological grade was also found to be a risk factor for recurrence in the pelvic bones. Patients with high-grade pelvic metastases had a higher recurrence rate in the pelvic bones than did patients with low-grade pelvic metastases. Finally, the type of surgery had an effect on the recurrence rate in the pelvic bones. Patients treated with curettage or marginal resection had a higher recurrence rate than those treated with wide en bloc resection. This result is not consistent with a previous report. 23
The overall survival rate for the whole series of patients was 29.2% at 5 years, which is higher than the previously reported rate of 13.0% 24 and approaches the previously reported rate of 36.4%.14,22 Neither multiple nor solitary metastases affected the survival rate in this study. Our study also showed no association between the type of surgery and the survival rate, which is consistent with previous reports25–27; however, some other authors found such an association.22,23 In addition, Hansen et al. 18 suggested that wide resection and reconstruction was preferred for patients with a good prognosis and that simpler surgical techniques were preferred for patients with a poor prognosis. The pathological grade was also found to be associated with the survival rate; patients with high-grade pelvic metastases had a poorer survival rate than patients with low-grade metastases.
Our study had certain limitations. First, this was a retrospective study, and the number of patients was not large enough for further statistical analysis. Second, the primary lesions, local interfering factors (muscles, fascia, vessels, and lymph nodes), and individual conditions were not fully considered in the present study. Third, the variety of metastases might have affected the final results.
In conclusion, patients with MBTP have a high risk of recurrence in the pelvic bones and poor survival after multimodal treatment. Recurrence in the pelvic bones might be affected by the metastatic involvement, tumor grade, surgical margins, and type of surgery, whereas the survival rate tends to be associated with the tumor grade.
Footnotes
Acknowledgment
We gratefully acknowledge the assistance of Professor Zhengdong Cai and Yingqi Hua from Shanghai Bone Tumor Research Institute in preparing the photomicrographs and research consultation.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was supported by Qingpu District Hospital New Star (W2019-02).