
Abstract
Cervical radiculopathy, with an incidence of approximately 85 per 100,000 individuals annually, is characterized by pain originating from cervical nerve root disruption. Accurate diagnosis is challenging because of the absence of a universally accepted gold standard, necessitating reliance on patient history, clinical examination, and diagnostic tests. Brachial plexus metastasis is a rare but clinically significant condition that can mimic common musculoskeletal disorders, such as cervical radiculopathy. Its nonspecific presentation often results in delayed diagnosis, particularly in patients with cancer presenting with persistent upper-limb pain. This case report explored the underdiagnosis of supraclavicular brachial plexus metastasis, initially misinterpreted as cervical disc herniation in a 62-year-old man with a history of lung cancer. Despite undergoing cervical-Racz catheter neuroplasty and other treatments, the patient’s persistent right arm pain prompted further investigations. Chest computed tomography and positron emission tomography computed tomography ultimately revealed metastatic squamous cell carcinoma extending to the brachial plexus. This case underscores the critical need for comprehensive diagnostic evaluations and the consideration of metastatic neoplasms in patients with a history of cancer. It also highlights the rarity and clinical significance of brachial plexus metastasis. It emphasizes the importance of an integrated approach to care, addressing both oncological and musculoskeletal issues to improve patient outcomes.
Keywords
Introduction
Cervical radiculopathy, with an annual incidence of approximately 85 per 100,000 individuals, 1 is characterized by pathological disruption affecting the cervical nerve root. This condition arises from encroachment and ensuing inflammation near the cervical neural foramen, causing cervical radicular pain that radiates from the neck to the arm due to irritation of a cervical spinal nerve or its roots. Diagnostic errors occasionally arise when patients present with symptoms suggestive of cervical radiculopathy, as an alternative underlying pathology can mimic this condition. 2
Clinical reports and previous studies indicate that brachial plexopathy caused by metastatic disease, although uncommon, can be a serious complication in patients with lung cancer. 3 Pancoast tumors, or superior sulcus tumors, may invade adjacent structures such as the brachial plexus, sympathetic chain, and vertebral bodies, leading to pain or weakness in the shoulder, upper extremity, and spine, and in some cases, Horner’s syndrome. Because of overlapping clinical features, these tumors are often misdiagnosed as benign musculoskeletal conditions, including cervical disc herniation or radiculopathy. 4 Shoulder pain is commonly the initial symptom, which may delay accurate diagnosis and appropriate treatment. 5
It becomes imperative to reassess the diagnosis and treatment plan if there is a lack of response to the initial treatment for cervical disc herniation. We present a case of a patient with persistent right arm pain, initially misdiagnosed as cervical radiculopathy, who was later found to have metastatic lung cancer extending to the brachial plexus. This case underscores the need for vigilance and comprehensive diagnostic evaluation when conventional treatment outcomes are insufficient. Persistent cervicobrachial pain unresponsive to conventional therapies should prompt clinicians to evaluate for potential metastatic causes.
Case report
The reporting of this study conforms to Case Report (CARE) guidelines.6,7 The patient provided verbal informed consent for publication of this case. We have deidentified all patient details.
A man in his early 60s presented to the pain clinic in October 2022, reporting persistent right arm pain that had begun 3 months earlier without any preceding trauma. His medical history was notable for hypertension, diabetes mellitus, liver cirrhosis, and previously treated lung cancer (squamous cell carcinoma). He had a left lower lobe lobectomy 4 years ago, followed by adjuvant chemoradiotherapy sessions, totally two times for 2 years. After chemoradiotherapy, polyneuropathy developed in him but he continued his prescribed medications and underwent regular follow-ups, during which no progression or new findings related to his lung cancer were observed.
Three months before his visit to our clinic, the patient experienced a sudden exacerbation of pain, from the right posterior neck to the shoulder and the whole right arm. Describing severe discomfort with an intensity of 8 out of 10 on the numeric rating scale (NRS). The pain originated in the right shoulder and radiated down to the forearm. In search of relief, he consulted a traditional Korean medicine clinic and sought the expertise of a local orthopedic surgeon, receiving treatments including shoulder and neck injections for the diagnosis of rotator cuff tear and shoulder impingement; however, his pain persisted.
Neurologic examination revealed altered pain sensation along the right upper extremity corresponding to the C5–C8 dermatomes, with hypoesthesia noted at the fingertips of the right hand. Motor strength was graded 3–4 out of 5 in finger flexion, whereas arm abduction, elbow flexion, wrist extension, and elbow extension were preserved at 5 out of 5.
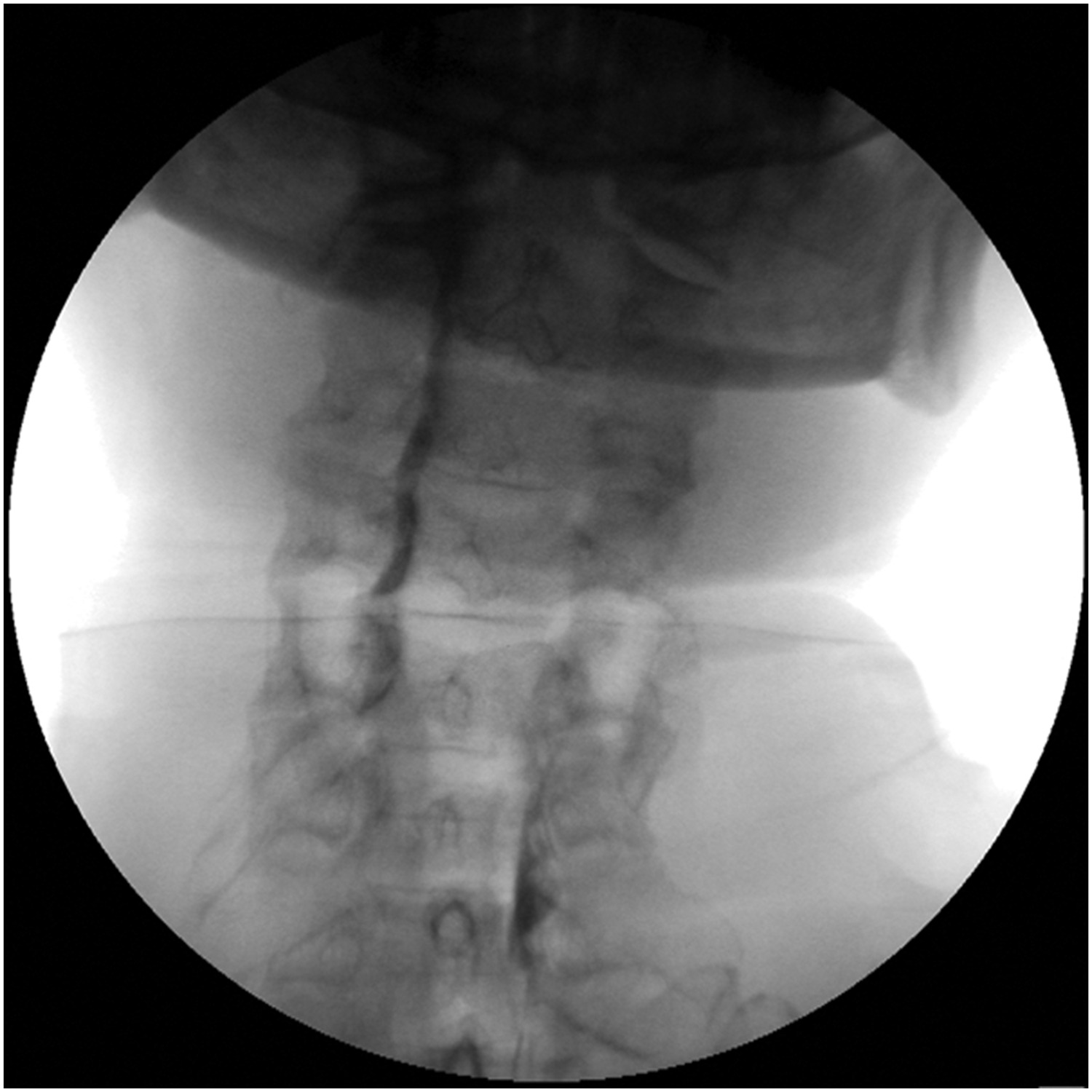
Subsequently, a bone scintigraphy was conducted for further evaluation, revealing enthesopathy in the coracoid processes of both scapulae, with more activity observed on the right side (Figure 1). An external cervical spine magnetic resonance imaging (MRI) was also performed, revealing centrally protruded discs at the C4–C7 levels (Figure 2). Given the ineffectiveness of previous treatments and the findings of the MRI and bone scintigraphy, with a diagnosis of cervical herniated disc-related radiculopathy, C5–C6 epidural block was performed (Figure 3).

Whole-body bone scintigraphy showing an increased radiotracer uptake in the right coracoid process compared with the left, indicating active enthesopathy. No evidence of metastatic bone lesions was detected.

Midsagittal T2-weighted cervical spine MRI demonstrating minimal right central disc protrusion and diffuse disc bulging at C3–C4 and C4–C5 levels. Mild right foraminal stenosis is noted at C5–C6, without significant spinal cord compression. MRI: magnetic resonance imaging.

Fluoroscopic lateral cervical spine image obtained during cervical epidural block at the C5–C6 level. The needle placement was performed under real-time imaging guidance for accurate drug delivery.
With the provisional diagnosis of cervical disc herniation, the cervical-Racz catheter (C-Racz) neuroplasty procedure was scheduled 1 week later. However, on the eve of his admission, the patient experienced a significant exacerbation of pain, prompting a visit to the hospital’s outpatient department. There, he was administered 50 mg of intravenous tramadol, after which his symptoms ameliorated, allowing for his discharge.
Upon admission, the patient underwent the insertion of a C-Racz catheter (EPIMED, VERSA-KATH, 21 g, 12 in (30.5 cm)) and a neuroplasty procedure targeting the right C4–C7 levels (Figure 4). The procedure transpired without any complications or remarkable findings. Despite this, there was no improvement in the patient’s symptoms, necessitating the initiation of a morphine fluid infusion at a dosage of 20 mg/day. In pursuit of elucidating the root cause of the persistent pain, consultations with the general surgery and neurology departments were arranged to exclude the possibilities of peripheral vascular disease and peripheral nerve disease, respectively. Nevertheless, these consultations yielded no specific findings.
Anteroposterior fluoroscopic view showing the insertion of a C-Racz (EPIMED, VERSA-KATH, 21 G × 12 in) targeting the right C4–C7 epidural space for neuroplasty. The procedure was uneventful but did not lead to clinical improvement. C-Racz: cervical-Racz catheter.
One week after discharge, the patient returned to the outpatient clinic, complaining of severe pain. He said that the effect of C-Racz neuroplasty lasted only for approximately 1 week, and he returned 1 week later with pain in his right arm. A regimen of intravenous tridol (tramadol) 50 mg as before was immediately administered, alongside a meticulously tailored oral medication protocol that included zanapam (alprazolam) 0.25 mg, 1.5 tablets three times a day (tid), stablon (tianeptine) 12.5 mg tid, and lyrica (pregabalin) 75 mg two times a day. In a concerted effort to alleviate his distress, injecting a lidocaine supraclavicular brachial plexus block on the right side was proposed. However, as the procedure unfolded during the ultrasound examination, the brachial plexus eluded clear visualization, hinting at underlying neurologic complexities. This unforeseen challenge led to the decision against proceeding with the injection.
Upon observing the patient’s unrelenting pain, we coordinated a referral to the thoracic surgery department and proceeded with a chest computed tomography (CT) and positron emission tomography (PET) CT scan to ascertain the potential recurrence of lung cancer and investigate the likelihood of metastasis (Figure 5). The CT scan unveiled a new, sizable soft tissue mass in the right supraclavicular area, accompanied by adjacent right axillary lymphadenopathy. The possibilities considered were a malignant mass indicative of metastasis or an inflammatory mass. To assess these findings, the patient was admitted for a comprehensive evaluation and tailored management strategy.

FDG PET/CT image illustrating hypermetabolic activity in the right supraclavicular region, consistent with viable metastatic lymph nodes. Progression is evident compared with imaging from 3 years prior, involving right cervical level V and axillary levels II and III. CT: computed tomography; FDG: 18F-Fluorodeoxyglucose; PET: positron emission tomography.
Following his admission to the thoracic surgery department, an ultrasound-guided biopsy was conducted, culminating in the diagnosis of metastatic squamous cell carcinoma. In response, palliative radiation therapy was meticulously targeted to the right supraclavicular area and the right axilla. Concurrently, chemotherapy was initiated, forming a pivotal component of the patient’s treatment regimen. This multifaceted approach led to a significant reduction in the patient’s pain, with his score declining to 3 out of 10 on the NRS, marking a considerable improvement in his quality of life amid challenging circumstances.
Discussion
Shoulder and arm pain is a common complaint among patients and can be caused by various underlying conditions. Cervical spine disc herniation is a frequent cause of cervical radiculopathy. In Rochester, Minnesota, the yearly occurrence of cervical disc herniations is 18.6 per 100,000 residents, with the highest incidence observed in individuals in their sixth decade of life. 8 Symptomatic herniation in the cervical spine most frequently occurs at the C6–C7 disc level, leading to compression of the C7 root. Typical symptoms include pain in the back of the upper arm, weakness in the triceps, wrist drop, and tingling sensations in the fingertips of the middle fingers. The next most commonly affected roots are C6 and C8, typically from issues at the C5–C6 disc and the C7–T1 disc, respectively. 9
Neoplastic invasion of the brachial plexus, although rare, can mimic symptoms of common upper-limb neuropathies, leading to potential misdiagnosis. It is more prevalent in individuals with a history of malignant disease, with common causes including lung cancer (Pancoast tumor), breast carcinoma, and lymphoma.3,10
Lung cancer is one of the most common tumors that can metastasize to the brachial plexus, along with breast cancer and lymphoma. The exact mode of spread is often lymphatic, with tumor cells reaching the area drained by the lateral–axillary lymph nodes near the brachial plexus. Pancoast tumors, which arise in the superior pulmonary sulcus of the lung, can directly invade and compress the lower trunk (C8–T1) and medial cord (C7) of the brachial plexus.5,11 This can cause severe pain, muscle weakness, and Horner’s syndrome on the affected side. In some cases, metastatic brachial plexopathy can be the initial manifestation of lung cancer, preceding the diagnosis of the primary tumor.5,12
Patients with a history of cancer-related plexopathy should be closely monitored for new lesions during ultrasound examinations of the brachial plexus. 4 Ultrasound, as well as additional imaging techniques such as MRI or 18F-fluorodeoxyglucose-PET/CT, should be used with care in patients with cancer to distinguish metastatic lesions. Ultrasound emerges as a simple, noninvasive, and cost-effective method for identifying metastatic lesions. 4 Also, gamma-scintigraphic imaging of areas with abnormal osteogenesis associated specifically with malignant bone lesions is achieved by the administration of hydroxyethylene-diphosphonate (HDP) labeled with 99mTc. 13 Traditional planar bone scintigraphy using 99mTc-labeled radiopharmaceuticals, like 99mTc-HDP), remains the most commonly used method for detecting bone metastases. 14 MRI is considered the gold standard for imaging the brachial plexus, but CT, PET/CT, and ultrasound can also aid in diagnosis and staging. 5
Metastatic infiltration of a peripheral plexus, also named metastatic plexopathy, often results in severe pain and muscular weakness. This rather rare event may have a dramatic impact on the quality of life of patients affected by cancer. 5 MRI plays a central role in identifying and precisely characterizing malignant lesions originating in the brachial plexus, as well as determining their extent and the condition of nearby structures due to its exceptional ability to capture detailed anatomical information. 11
This reported case describes a patient with metastatic squamous cell carcinoma of the lung presenting initially with brachial plexopathy, which was misdiagnosed as cervical disc herniation until imaging revealed a right supraclavicular mass.
The nature of severe, persistent pain did not entirely align with cervical disc findings as initially thought. In this situation, if symptoms and examination findings related to the neck, shoulder, and/or upper extremities remain unexplained by cervical spine MRI, it might be appropriate to consider thoracic and/or brachial plexus MRI as the next diagnostic steps. 15 Fortunately, the attempt to alleviate the patient’s pain with a brachial plexus block, guided by ultrasound observation, provided the most crucial clue for differential diagnosis and revealed a lung metastatic lesion causing severe pain. Lung cancer presenting with musculoskeletal symptoms should be considered, particularly in patients with risk factors such as male sex, age in the 60s, a history of smoking, suggestive clinical presentation, and abnormal imaging findings. 16 This case highlights the need for clinicians to re-evaluate initial assumptions and expand the differential diagnosis when symptoms persist despite appropriate treatment.
Conclusion
Persistent cervicobrachial pain unresponsive to treatment should prompt clinicians to consider neoplastic brachial plexopathy, particularly in patients with a history of malignancy. Even if treatment has been administered based on the pain’s characteristics, the diagnosis can still be altered. The patient’s history is also very important, especially for those who have had a history of cancer. Even though patients complain about musculoskeletal related symptoms, metastatic cancer should be in mind for differential diagnosis. Both musculoskeletal ultrasound and MRI play important roles in the evaluation of nontraumatic brachial plexopathies, including those of compressive, neoplastic, or inflammatory origin. In particular, musculoskeletal ultrasound can serve as a practical alternative when MRI is contraindicated or poorly tolerated by patients.
Footnotes
Acknowledgments
We thank all those who contributed to this work.
Author contributions
So Young Kwon contributed to study conception, design, and data acquisition. Eun Hwa Jun contributed to writing the original draft. So Young Kwon provided editorial support. All authors contributed to the interpretation and analysis of literature search as well as carefully and critically revising and approving the final manuscript.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Ethics and consent
The patient provided verbal informed consent for publication of this case. This case report was approved by the Institutional Ethics Committee of St. Vincent’s Hospital, Republic of Korea (approval no. VC24ZISI0043). This study has been reported according to the CARE guidelines established by the EQUATOR Network. The CARE checklist has been completed and submitted along with this manuscript. All patient details have been de-identified to ensure anonymity.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.