
Abstract
This report presents a rare case of bronchogenic adenocarcinoma with initial metastasis in the external auditory canal. The patient, a 64-year-old man with a history of bladder urothelial carcinoma, initially presented with a persistent right otitis externa. Otoscopic examination revealed a mass obstructing the right external auditory canal. The temporal bone computed tomography scan revealed a mass that completely obstructed the right external auditory canal and extended into the middle ear. A biopsy showed a poorly differentiated adenocarcinoma of bronchogenic origin, confirmed by positive immunohistochemical staining for cytokeratin 7 and Thyroid transcription factor-1. Further imaging revealed a large tumor mass in the lung involving the mediastinum and parenchyma, along with carcinomatous lymphangitis and cerebral metastasis. Histopathological examination of the primary lung tumor confirmed a poorly differentiated adenocarcinoma with similar features to the metastasis in the external auditory canal. The tumor was staged as T4N2M1c, and the patient underwent local external-beam radiation therapy with chemotherapy.
Introduction
Malignant lesions in the external auditory canal (EAC) are very uncommon, accounting for less than 0.2% of all head and neck cancers. 1 Metastatic tumors to the EAC are extremely rare and usually occur in advanced stages. There are only a few documented case reports in the literature, documenting a diverse range of primary tumor sites.2,3 To the best of our knowledge, there have been only two reported cases of metastatic lung cancer to the EAC: Hain et al. 4 reported a case of a 73-year-old man with metastatic small-cell lung cancer in the bony EAC where biopsy confirmed histological similarities between the metastasis and the primary tumor. The second case was reported by Vasileiadis et al. 2 and involved a 62-year-old woman with bronchogenic adenocarcinoma, which was revealed by a metastatic mass in the EAC. Therefore, our case represents the third reported case in the literature of EAC metastasis from lung cancer, and it is the second case in which an auricular mass was the sole symptom revealing a bronchogenic adenocarcinoma.
Case report
A 64-year-old man, a former smoker of 40 pack per years, presented with failed conservative treatment for persistent right otitis externa. The patient had a medical history of bladder urothelial carcinoma. The patient had a medical history of bladder urothelial carcinoma without any other comorbidities. The bladder carcinoma was diagnosed 12 years ago following the onset of hematuria and pollakiuria, which led the patient to seek medical attention. A cystoscopy with biopsies was performed, and the histological examination confirmed a transitional cell carcinoma, and the tumor was classified as cT2bN0M0. The patient had a bladder preservation protocol, which involved receiving four cycles of MVAC polychemotherapy (Methotrexate, Vinblastine, doxorubicin (Adriamycin), Cisplatin), followed by radiotherapy, spread out over a 6-week period. The patient was consistently monitored for a period of 10 years, during which follow-up cystoscopies and urological computed tomography (CT) scans revealed no signs of tumor recurrence. However, he subsequently discontinued regular follow-up care.
The patient presented with right-sided ear pain, bloody ear discharge, and a noticeable hearing loss that had been ongoing for 1 month. Initially diagnosed as otitis externa, the condition did not improve despite treatment with antibiotics. The patient denied experiencing any tinnitus or vertigo.
Upon otoscopic examination, a friable, polypoid mass with surface bleeding was observed, completely obstructing the right EAC. The rest of the ear, nose, and throat examination, including cranial nerves and nasoendoscopy, showed no remarkable findings.
A temporal bone CT scan revealed extensive soft tissue density mass totally obstructing the right EAC, extending into the hypotympanum of the middle ear. There was no evidence of ossicular chain disruption, but significant bony erosion of the tympanic bone was observed (Figure 1).
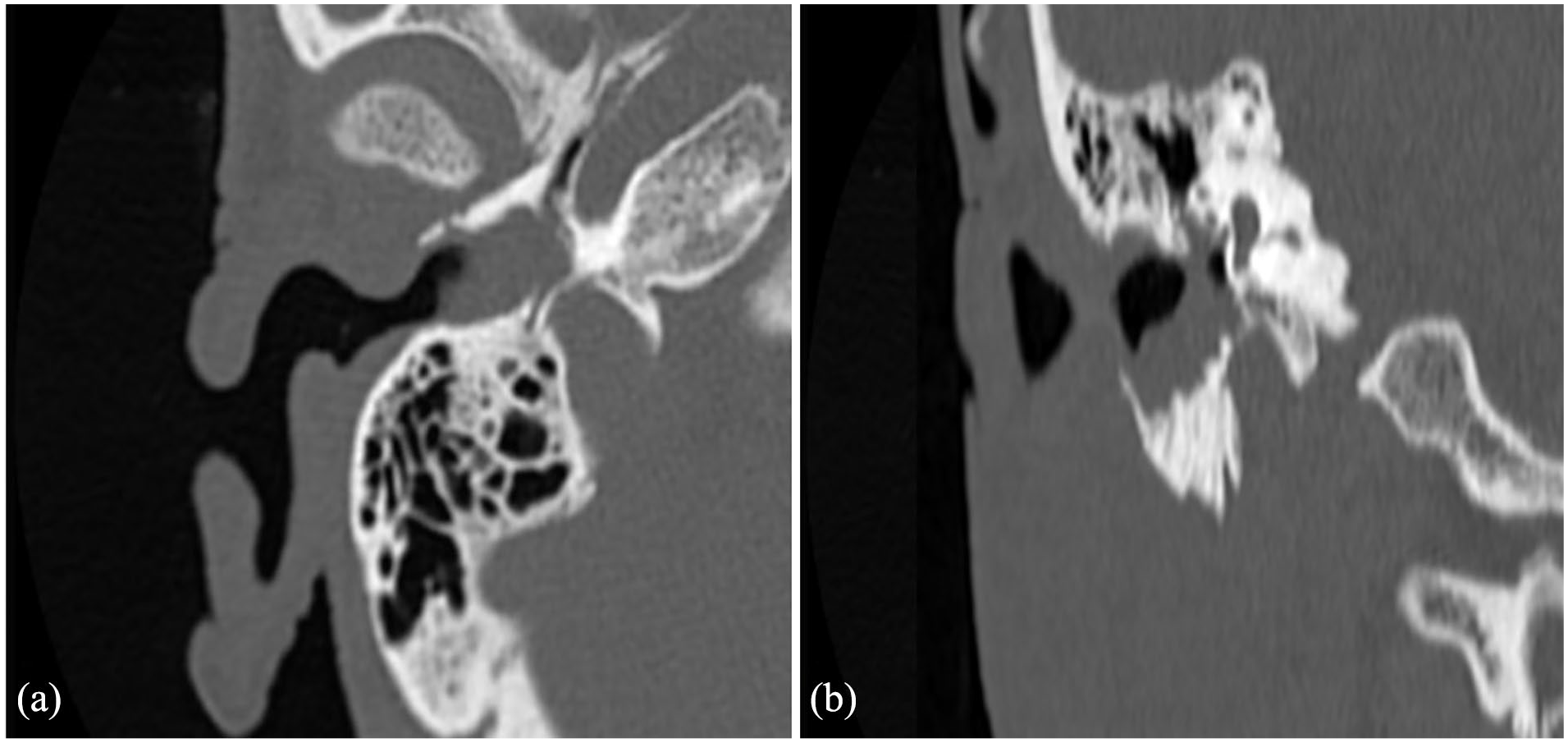
Axial (a) and coronal (b) views of computed tomography of petrous temporal bones showing an erosive mass of the right external auditory canal (EAC), extending into the middle ear with erosion of the anterior and inferior EAC walls.
An excisional biopsy was performed under general anesthesia. The histopathological examination showed carcinoma cells exhibiting nuclear atypia, separated by a fibrous and well-vascularized stroma. These findings were consistent with poorly differentiated adenocarcinoma. The bronchogenic origin of the tumor was established based on positive immunohistochemical (IHC) staining for cytokeratin 7 and Thyroid transcription factor-1 (TTF1), while staining for p63 protein and Trans-acting T-cell-specific transcription factor GATA-3 was negative. This ruled out a urothelial origin for this metastatic lesion (Figure 2).

Histological findings: (a) and (b). Proliferation of clusters of cubocylindrical cells with densely atypical nuclei within a fibro-inflammatory stroma (blue asterisk). This proliferation elevates a surface squamous epithelium lining of the EAC (red asterisk) (HE ×400). (c) Positive immunostaining for Thyroid transcription factor-1 (×400). (d) Positive immunostaining for cytokeratin 7 (×400).
An extension assessment was then conducted to investigate the primary tumor and identify any other distant metastases. A cervico-thoraco-abdomino-pelvic CT scan revealed a massive tumor mass in the apical and dorsal region of the right upper lobe of the lung, accompanied by carcinomatous lymphangitis in the dorsal segment. Additionally, a few centimeter-sized lymph nodes were observed in the right pulmonary hilar and peritracheal regions (Figure 3(a) and (b)). An enhanced brain CT scan exhibited a well-defined, homogeneous expansive process in direct contact with the left side of the cerebellar tent, suggestive of a secondary brain localization (Figure 3(c)).

Sagittal (a) and axial (b) views of contrast-enhanced thoracic computed tomography (CT) revealing a massive tumor mass in the apicodorsal region of the right upper lobe of the lung. Axial (c) view of contrastenhanced cerebral CT revealing a well-defined, homogeneous process that avidly enhances, surrounded by a prelesional hypodensity zone, in direct contact with the left side of the cerebellar tent (red arrow).
A CT scan-guided biopsy of the primary lung tumor was performed. Histopathological examination concluded a widely necrotic, poorly differentiated mixed-type primary adenocarcinoma, which exhibited similar histopathological and IHC features to the metastasis in the EAC.
The tumor was staged as T4N2M1c. The patient received local external-beam radiation therapy for both EAC and cerebral metastatic lesions, with a total dose of 30 Gray administered over 10 fractions (3 Gray/fraction). Following radiation therapy, he received 4 cycles of chemotherapy consisting of cisplatin at a dose of 80 mg/m² on day 1 and day 22, as well as gemcitabine at a dose of 1250 mg/m² on day 1, day 8, and day 22. Unfortunately, the patient died due to deteriorating general condition.
Discussion
Lung cancer is one of the deadliest cancers, representing a leading cause of cancer-related deaths in both men and women worldwide. 5 The majority of lung cancers are diagnosed at an advanced stage, with over half of them being metastatic at the time of diagnosis. 5
The most common sites of lung cancer metastases include the brain (39%), bones (34%), liver (20%), respiratory system (18%), and adrenal glands (8%). 6 Metastases to the head and neck region are very rare, accounting for only approximately 3% of lung metastatic sites. 7 The majority of these metastases are localized in the lymph nodes, although they can occur in any anatomical area of the head and neck. 7
In the temporal bone, metastases are most commonly found in the petrous portion, internal auditory canal, or mastoid process, and are extremely rare in the EAC. 2 A review of the English literature from January 1990 to October 2023 identified 18 cases of metastases from various primary tumors in the EAC (Table 1). Our review excluded cases of metastases at sites other than the EAC within the temporal bone, cases of metastases originating from cutaneous tumors, as well as cases where the metastasis spread to the EAC from an adjacent structure. In four cases (22.2%), the primary tumor was colorectal, in three cases (16.7%) it was breast cancer, and in two cases (11.1%) each it was lung, kidney, esophageal, and prostate cancer, and in one case (5.6%) each it was liver, brain, and nasopharynx cancer.2–4,8–22 Metastases to the EAC were metachronous to the primary tumors in 11 cases (61.1%) and synchronous in 7 cases (38.9%) (Table 1).
A summary of the reported cases in the English literature of metastases from various primary tumors in the external auditory canal since 1990.

CT: chemotherapy; EAC: ear auditory canal; F: female; M: male; NA: not available; RT: radiotherapy.
Primary cancer of the EAC and metastatic cancer to the EAC share similar clinical presentation. Commonly reported symptoms include hearing loss, otalgia, ear discharge, bleeding, or the presence of a swelling in the EAC.2–4,8–22 However, none of these symptoms are specific to malignancy and can also occur in benign conditions such as EAC cholesteatoma or necrotizing external otitis.3,10 This similarity makes it challenging to clinically distinguish between benign and malignant conditions, leading to potential delays in diagnosis. However, a short duration of otologic symptoms and a history negative for previous inflammatory ear disease in adults between 50 and 60 years of age should raise suspicion for malignant diseases. 2
In our case, the CT of the temporal bone revealed a complete obstruction of the EAC by a mass with soft tissue density extending into the middle ear, along with bone erosion of the tympanic bone. The diagnosis of malignancy was considered due to the large mass in the EAC, its extensive and irregular bone destruction of the EAC walls, and its invasion of adjacent anatomical structures. Magnetic resonance imaging (MRI) of the temporal bone would be useful in cases of diagnostic uncertainty, particularly in differentiating an EAC cholesteatoma. 3 However, neither CT nor MRI could differentiate between a primary or secondary tumor of the EAC.
The definitive and accurate diagnosis is made from findings of excisional biopsy. The combination of histopathological examination and IHC study is essential for distinguishing between a primary EAC cancer and a metastatic lesion and determining the primary tumor of the metastatic lesion. In our case, the positive immunostaining for cytokeratin 7 and TTF1 strongly suggested a bronchogenic origin. The similarity of the IHC profile between the metastasis and the primary tumor provided evidence supporting a common origin for these two lesions.
Due to the limited number of reported cases with metastasis in the EAC, there are currently no established guidelines for their management. The treatment approaches have been non-consensual and varied across different cases, taking into consideration factors such as the primary tumor site and histological type, tumor staging, overall patient health and comorbidities, as well as the presence of other metastatic lesions.2–4,8–22 Treatment options included surgical resection, radiotherapy, chemotherapy, hormonal therapy, or a combination of some of these approaches.
The available data on the prognosis and overall survival of patients with metastasis in the EAC are limited. However, it is widely recognized that lung cancer has a poor prognosis. The 5-year survival rate for lung cancer is approximately 15%, but this drastically drops to less than 1% in cases of metastatic tumors. 23 A multidisciplinary approach is essential for improving the survival and quality of life of patients with metastatic lung cancer. Recent advancements in treatment modalities, particularly targeted biological drugs that target specific genetic mutations like epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase, and ROS1 proto-oncogene tyrosine kinase, have shown promise in enhancing outcomes. 24 EGFR inhibitors, for instance, have demonstrated superior response rates and progression-free survival compared to standard chemotherapy. 24 Unfortunately, access to these drugs and genetic mutation testing remains limited in our country.
Conclusion
We reported an exceptionally rare case of bronchogenic adenocarcinoma metastasis to the EAC, highlighting the importance of considering such uncommon clinical entities in the differential diagnosis of EAC masses. Imaging aid in the evaluation, but definitive diagnosis relies on histopathological examination and IHC analysis. The management of these cases remains challenging and lacks consensus due to the limited number of reported cases.
Footnotes
Acknowledgements
All authors approved the final version and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accura.
Author contributions
A.S., research and writing of the manuscript; W.O., research and writing of the manuscript; K.R., research and writing of the manuscript; B.A.M., research and writing of the manuscript; H.B., co-supervisor; C.A., co-supervisor; C.I., co-supervisor.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a patient’s legally authorized representative(s) for anonymized patient information to be published in this article.