
Abstract
Objective
To examine the pain-reducing effects of intra-articular oxygen–ozone (O2O3) injections and mechanical focal vibration (mFV) versus O2O3 injections alone in patients with knee osteoarthritis.
Methods
Patients with chronic pain (>6 weeks) due to knee osteoarthritis (II–III on the Kellgren–Lawrence scale) were consecutively enrolled and divided into two groups: O2O3 (n = 25) and O2O3-mFV (n = 24). The visual analog scale (VAS), Knee Injury and Osteoarthritis Outcome Score (KOOS), and Medical Research Council (MRC) Manual Muscle Testing scale were administered at baseline (before treatment), after 3 weeks of treatment, and 1 month after the end of treatment. Patients received three once-weekly intra-articular injections of O2O3 into the knee (20 mL O3, 20 μg/mL). The O2O3-mFV group also underwent nine sessions of mFV (three sessions per week).
Results
The VAS score, KOOS, and MRC score were significantly better in the O2O3-mFV than O2O3 group. The within-group analysis showed that all scores improved over time compared with baseline and were maintained even 1 month after treatment. No adverse events occurred.
Conclusion
An integrated rehabilitation protocol involving O2O3 injections and mFV for 3 weeks reduces pain, increases autonomy in daily life activities, and strengthens the quadriceps femoris.
Keywords
Introduction
Patients with knee osteoarthritis (KOA) develop avoidance behaviors (kinesiophobia) to evade the onset of pain, especially in the acute phase, limiting their compliance with effective rehabilitation strategies such as regular exercises.1–3 Thus, other conservative treatments, such as intra-articular injections of corticosteroids, 4 hyaluronic acid, or oxygen–ozone (O2O3), can be useful for reducing pain and represent excellent alternatives in the rehabilitation of KOA.5–8 Moreover, an integrated rehabilitation approach can allow patients with KOA to minimize their intake of oral or systemic pain medications (e.g., nonsteroidal anti-inflammatory drugs), thus decreasing the adverse effects of these medications.9–11
Intra-articular injections of O2O3 for KOA relieve pain, reduce effusion, improve the mobility of the knee joint, and have good efficacy, especially during the exacerbation of stage І to ІІ pain on the Kellgren–Lawrence (KL) scale.12–14 Intra-articular O2O3 injections are safe and have encouraging short- and medium-term effects on pain control and functional recovery in patients with KOA.15,16 Injections of O2O3 inhibit proinflammatory cytokines, such as prostaglandin E2, in favor of anti-inflammatory cytokines, such as interleukin 10, transforming growth factor β, and interleukin 4; antioxidant enzymes; and angiogenesis. These components cooperate to repair the articular joint by stimulating fibroblasts, chondrocytes, and stem cells. 9
Considering the benefits of an integrated rehabilitative approach for patients with KOA, proprioceptive exercises should be widely recommended. 17 Patients with KOA commonly experience weakness during extension of the knee, which often contributes to the progressive reduction in muscle mass with age. As age increases, the number of motor units of the muscle decreases, causing changes in the ability of the muscle tissue to generate strength.18,19 This aging-related phenomenon is exacerbated at the age of >65 years (similar to the phenomenon that occurs in patients with KOA), inducing greater involvement of the muscles of the lower limbs (particularly the femoral muscle of the quadriceps). 20
During rehabilitation, mechanical focal vibration (mFV) is used to stimulate individual muscle groups and selectively activate the Ia and IIb fibers and the Golgi tendon organs, depending on the frequency of stimulation [in Hertz (Hz)]; the effect of mFV is to improve muscle strength and proprioception. 21 In a recent review, Aboutorabi et al. 22 studied the use of mFV for postural control and gait in elderly patients. In particular, the application of vibrating insoles and localized vibrations to the ankle and foot has had good efficacy. mFV therapy provides mechanical signals to the bone and muscle–tendon system, imitating movement and exercise and positively influencing muscle function and coordination.23,24 In contrast, no studies have been performed to assess the effect of mFV in patients with KOA and the association of mFV with intra-articular O2O3 injections.
Our working hypothesis is based on the fact that the infiltration of O2O3 into the knee joint of patients with KOA can be used as adjunctive therapy in rehabilitation treatment; specifically, we consider that O2O3 injections can reduce pain through the ability of O2O3 to limit the release of inflammatory mediators and activate the micro-circulation. Thus, the present study was performed to examine the effects of the combination of mFV and intra-articular injections of O2O3 into the knee with respect to reducing pain and thus strengthening muscles and improving knee proprioception, considering the reduction in pain as the primary outcome and the recovery of knee function as a secondary outcome.
Materials and methods
Patients of both sexes with KOA who were attending the outpatient rehabilitative unit of G. d’Annunzio University of Chieti-Pescara from September 2018 to May 2019 were enrolled in this study. The diagnosis of KOA was based on clinical and radiographic criteria established by the American College of Rheumatology for KOA. 25
The inclusion criteria were an age of 40 to 70 years, diagnosis of chronic pain (>6 weeks) due to KOA (II–III on the KL scale), 10-cm visual analog scale (VAS) 26 score of 3 to 8 (or 4–9 if the patient had taken pain relievers) during the 48 hours prior to the screening visit, and discontinuation of analgesics (except paracetamol) within 2 weeks of the first visit. 27
The exclusion criteria were grade I and IV KOA on the KL scale 28 ; knee joint instability (anterior cruciate ligament lesion, decreased muscle strength); pain in the contralateral knee (VAS score of ≥1); previous open or arthroscopic knee surgery; a history of systemic or local infectious, neoplastic, or rheumatic disease; a pacemaker; hematological disease; bleeding disorders; pregnancy; patient refusal or noncompliance; being a candidate for knee joint replacement; any intra-articular injection during the last year; addiction to opioid drugs; thrombocytopenia; use of anticoagulants or antiplatelet drugs; and recent myocardial infarction or stroke.
Clinical data were collected before treatment (T0, baseline), after 3 weeks of treatment (T1), and 1 month after the end of treatment(T2). Adverse events were also registered during the follow-up.
This study was performed in accordance with the Helsinki Declaration on human experimentation. The study was approved by the Departmental Committee of Medical, Oral and Biotechnological Sciences of G. d’Annunzio University of Chieti (Italy) (No. 219/2019) and the Ethic Committee of the Institute for Treatment, Care and Research, IRCCS Centro Neurolesi “Bonino Pulejo,” Messina, Italy (Protocol Number 06-2020). All patients gave written informed consent to undergo the treatment after receiving detailed information regarding the procedures. 29
Study design
This prospective, observational case–control study was conducted in accordance with the STROBE guidelines. 30 Patients were consecutively enrolled and divided into two groups: the O2O3 group (patients who underwent treatment with intra-articular injections of O2O3 into the knee) and the O2O3-mFV group (patients who received the same O2O3 injections in addition to mFV for rehabilitation).
To reduce bias, the rehabilitation physician who administered the rating scales was blinded to the patient’s group assignment, and the researcher who analyzed the data was blinded to the therapy.
Clinical evaluation scales
A 10-cm VAS (0 cm, no pain; 10 cm, worst imaginable pain) was used to assess knee pain experienced during the previous 24 hours. 26 The Knee Injury and Osteoarthritis Outcome Score (KOOS)31,32 was also administered. The KOOS is a questionnaire that assesses short-term and long-term patient-relevant outcomes of knee injury or KOA. The KOOS is self-administered and evaluates five outcomes: pain, symptoms, activities of daily living (ADL), sport and recreational function, and knee-related quality of life. Finally, a physiatrist performed a clinical evaluation of the range of motion of the knee (flexion/extension) and assessed the strength of the femoral quadriceps using the Medical Research Council (MRC) Manual Muscle Testing scale, the score of which ranges from 0 to 5 (0, no movement; 5, movement possible against maximum resistance). 33
Infiltrative treatment
All patients received three once-weekly intra-articular O2O3 injections into the knee (20 mL O3, 20 μg/mL). 34 All injections were performed by the same physician who specialized in physical and rehabilitation medicine and was trained in intra-articular infiltration. The anterior access was used, with the patient supine or sitting on the edge of the bed with the knee flexed at 90 degrees. Common disinfection standards were ensured. An 18G needle was used. After each infiltrative therapy, the patient applied ice to the painful region for at least 10 minutes. 27
Rehabilitative treatment
The patients in the O2O3-mFV group also underwent nine sessions of mFV therapy (three sessions per week). Each session involved mFV at a frequency of 300 Hz for 15 minutes and was administered by an expert physiotherapist who specialized in physical therapy. The rectus femoris, tensor fasciae, and vastus medialis muscles were treated (Figure 1(a)). During the mFV treatment, the patient was asked to perform isometric muscle contractions that had been previously illustrated by the physiotherapist. At the end of the treatment, the patients underwent a 1-month follow-up period without treatment.

Mechanical focal vibration. (a) Positioning of the Vibration Sound System® (ViSS) transducers on the treated muscles. 1, tensor fasciae muscle; 2, rectus femoris muscle; 3, vastus medialis muscle. (b1, b2) ViSS transducers of different shapes and sizes.
The mFV was applied using a Vibration Sound System® (ViSS) physical therapy device (European patent: Ep1824439–CE 1936, Certificate of Conformity: No. HD 60114019; Unibell, Calco, Lecco, Italy). The transducers had cups with a diameter of 80 mm, were rectangle-like with a length of 140 mm, and were composed of acrylonitrile butadiene styrene (a common thermoplastic polymer with mechanical properties, such as impact and heat resistance and toughness), whereas the lateral bearing was made of a thermoplastic vulcanizate (Santoprene™; ExxonMobil Chemical, Houston, TX, USA) (Figure 1(b)). The ViSS system comprises a 32,000-revolution turbine with a flow rate of 35 m3/hour that generates air waves with a pressure of up to 250 mbar and a flow modulator that vibrates air with a pressure of up to 630 mbar and a frequency of up to 980 Hz (however, a frequency of up to 300 Hz is recommended) to produce mechanoacoustic waves. 35
Statistical analysis
Sample size
Based on the results of a previous study, 36 a target sample size of 40 patients (20 in each group) was calculated to ensure at least 90% power to detect a difference of 1.7 points with a 1.3-point standard deviation in the VAS scores between the two treatment groups using a two-sided test and α = 0.01 (anticipating an early discontinuation rate of 20%). Results are expressed as median (range) for continuous variables. The baseline demographic and clinical data were age, body mass index (BMI), and sex (female or male). Differences in baseline characteristics between the two treatment groups were analyzed by Fisher’s exact test or the Mann–Whitney U test, as appropriate. Time differences between the two groups were analyzed by the Friedman test for repeated measures to determine if there were differences in evaluation times. Pairwise comparison was performed for each parameter with Bonferroni correction. The Mann–Whitney U test was used for all parameters to evaluate time differences between groups, and variations (Δ) in the VAS score and KOOS between T0 and T1, T1 and T2, and T2 and T0 were compared between the two groups. A p value of <0.05 was considered significant. Statistical analyses were performed using PASW Statistics for Windows, Version 18.0 (SPSS Inc, Chicago, IL, USA).
Results
Of 55 patients, the data of 49 patients were analyzed. The O2O3-mFV group comprised 25 patients (6 men, 19 women), and the O2O3 group comprised 24 patients (5 men, 19 women) (Figure 2).

Study flow chart in line with the STROBE statement. O2O3, oxygen–ozone; mFV, mechanical focal vibration.
Six patients were excluded: two patients in the O2O3 group did not complete the treatment (one because of an accidental fall with a resultant femoral fracture and one because of commencement of another physiotherapy treatment), and four patients in the O2O3-mFV group failed to attend a minimum of eight sessions of mFV. No patients took analgesics during the infiltrative treatment. No adverse events were reported during the infiltrative treatment or observation period. Descriptive statistics for age, BMI, and sex were analyzed. Compared with baseline, the two groups were homogeneous and matched for age (mean age in O2O3-mFV group, 64.48 ± 5.49 years; mean age in O2O3 group, 59.3 ± 11.60 years) but not BMI (mean BMI in O2O3-mFV group, 25.54 ± 3.29 kg/m2; mean BMI in O2O3 group, 28.84 ± 2.37 kg/m2; p = 0.006) (Table 1).
Descriptive statistics for age, weight, height, and BMI in the two groups (median, minimum, and maximum, mean± standard deviation).
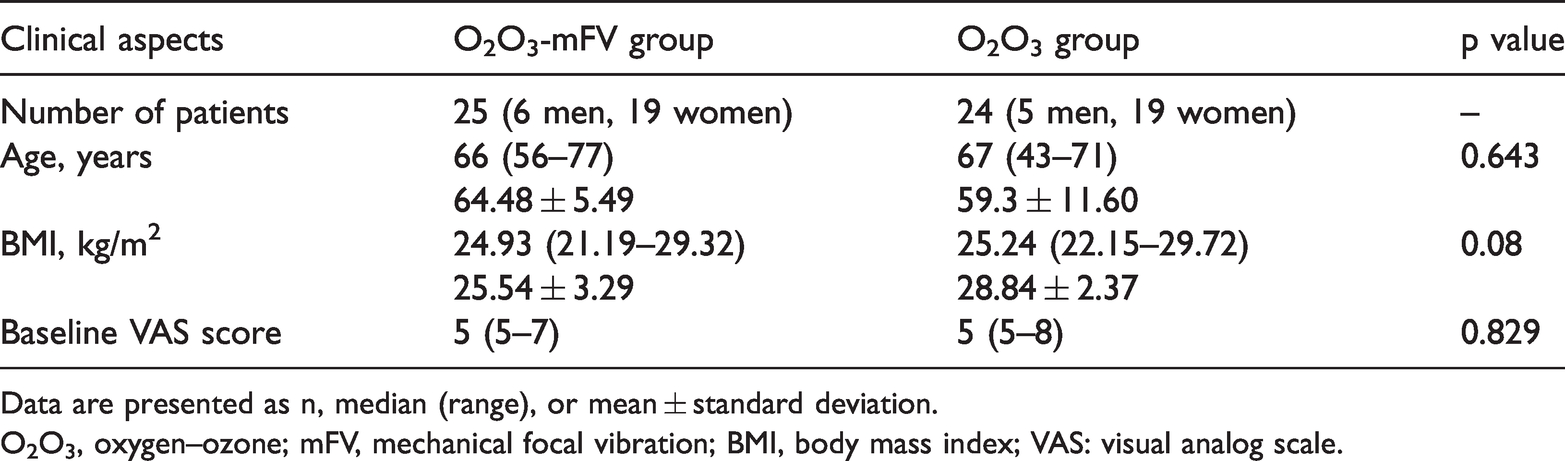
Data are presented as n, median (range), or mean ± standard deviation.
O2O3, oxygen–ozone; mFV, mechanical focal vibration; BMI, body mass index; VAS: visual analog scale.
The VAS score, KOOS, and MRC score were significantly better in the O2O3-mFV group than O2O3 group (Table 2).
Time difference (Δ) between the two groups with respect to treatment.

Boldface p values are statistically significant.
O2O3, oxygen–ozone; mFV, mechanical focal vibration; VAS, visual analog scale; KOOS, Knee Injury and Osteoarthritis Outcome Score; MRC, Medical Research Council; ADL, activities of daily living; T0, before treatment (baseline); T1, end of 3-week treatment; T2, 1 month after end of treatment.
The within-group analysis showed an improvement in the VAS score, KOOS, MRC score, and KOOS-ADL score over time compared with baseline, with good values being maintained even at T2 (Table 3).
Post-hoc within-group analyses over time.
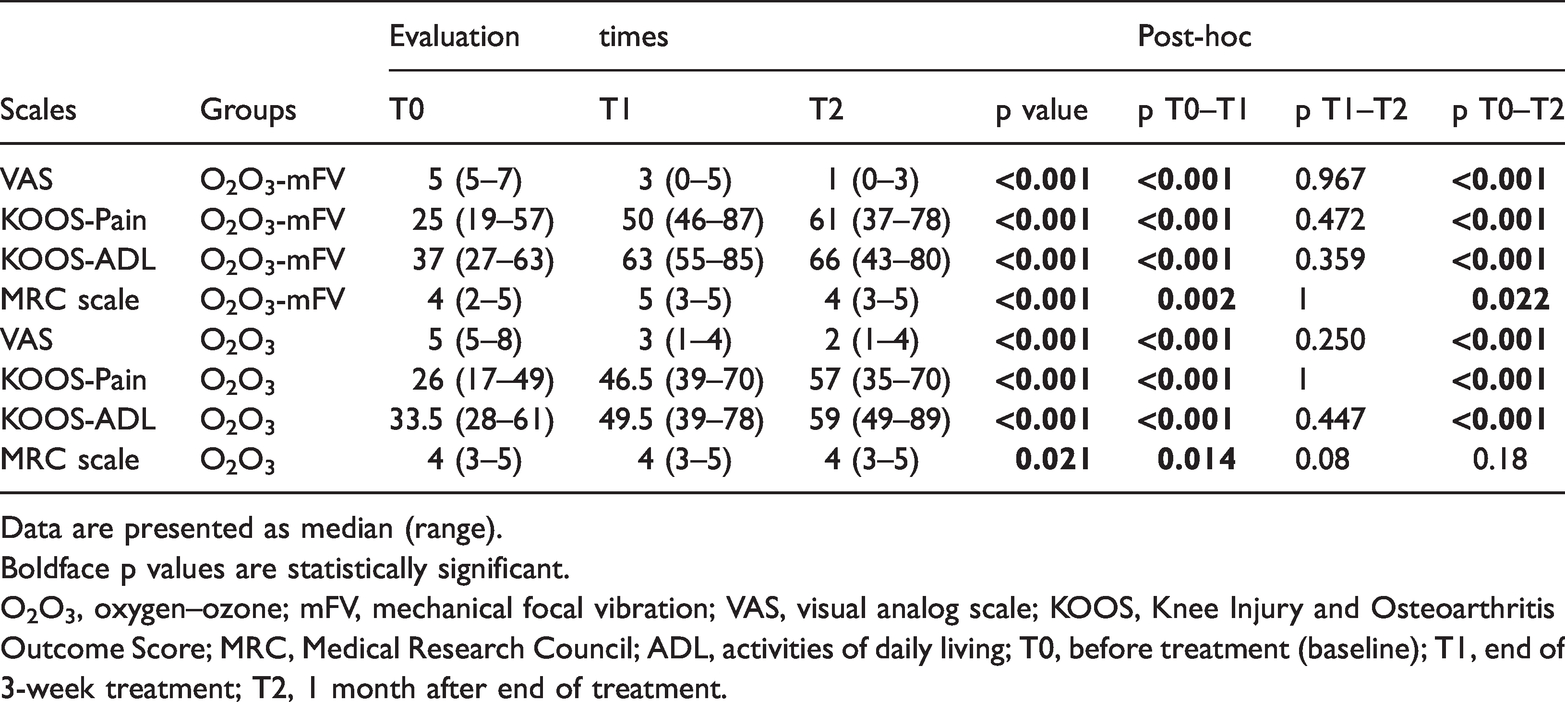
Data are presented as median (range).
Boldface p values are statistically significant.
O2O3, oxygen–ozone; mFV, mechanical focal vibration; VAS, visual analog scale; KOOS, Knee Injury and Osteoarthritis Outcome Score; MRC, Medical Research Council; ADL, activities of daily living; T0, before treatment (baseline); T1, end of 3-week treatment; T2, 1 month after end of treatment.
No adverse events were reported.
Discussion
This study was performed to verify the effects of an integrated rehabilitation protocol in patients with KOA involving a short protocol of infiltrations with three once-weekly O2O3 injections in combination with mFV. The study results are encouraging in this regard, with a statistically significant difference in favor of O2O3-mFV for pain and function. Additionally, the intra-articular injections of O2O3 relieved pain as reflected by the improvement in the autonomy of ADL, with good maintenance of the results even at follow-up. Both groups showed positive trends, but the improvement in pain in the O2O3-mFV group was greater and more stable over time.
There is evidence of the effectiveness of O2O3 infiltrations in musculoskeletal diseases, but no uniform treatment protocol has been established.34,37,38 An O3 concentration of 20 μg/mL (10 mL) was suggested by de Jesus et al. 39 for intra-articular injections of the knee, with a protocol of eight once-weekly infiltrations. This differs from our protocol, which involved three once-weekly infiltrations of 20 μg/mL (20 mL).
During the past several years, O2O3 therapy has been successfully used to treat low back pain in patients with lumbar hernias; it has also been helpful in reducing pain after the failure of other conservative treatments.37,38,40,41 Although rare, adverse effects of O2O3 therapy include sweating, a drop in blood pressure, dizziness, palpitations, and redness of the face accompanied by headaches.42–44 Thus, patients should not be discharged immediately after O2O3 infiltration and should instead be monitored for a safe period. In our protocol, 20 minutes was sufficient to rule out the onset of these adverse effects.
The mechanism of action of O2O3 is attributed to its downregulation of the synthesis of proinflammatory prostaglandins and oxidative stress through the induction of antioxidant enzymes (superoxide dismutase, glutathione peroxidase, and catalase). In addition, O2O3 improves the supply of O2 to tissues through vasodilatation and the stimulation of angiogenesis. 45 O3 acts as a hormonal prodrug:46,47 the use of a low-level agent, harmful at high levels, induces an adaptive and beneficial response. Thus, an appropriate dose of O3 upregulates antioxidant defenses and reverses chronic oxidative stress.
Intra-articular O2O3 injections (40 μg/mL) attenuate synovitis in rats with rheumatoid arthritis by inhibiting tumor necrosis factor (TNF)-α and antibodies to TNF receptor II and enhancing TNFR I activity against the articular synovium. Additionally, O2O3 appears to interact with cytokines, generating an anti-inflammatory response that might improve symptoms.48,49
Our results suggest that an integrated approach to KOA involving intra-articular O2O3 infiltration into the knee in association with mFV has greater effects in pain relief (Tables 2 and 3) and improves the strength of the extensor muscle in the knee. In the field of rehabilitation, there is much evidence that mFV improves muscle strength and proprioception using various protocols depending on the medical device.21–23 Although there is no universal consensus on the ideal protocol, the transmission of high- and low-intensity mechanical signals simulates the physiological stimuli that the human body encounters in daily life, ensuring safer effects than those of mild training programs.50,51 Several groups have shown that mFV consistently alters the interaction between the vibrated muscle and its antagonists and increases motor coordination, thus likely improving joint performance.52,53 Furthermore, the onset of the effects of mFV occurs as soon as 60 minutes after the end of the intervention.54–56 Thus, mFV should be a valid strategy in rehabilitation programs for patients with KOA.
Strengths and weaknesses
This study has some points of strengths. No previous studies have examined an integrated rehabilitation protocol that combines intra-articular infiltrations of O2O3 and instrument-based physical therapy (mFV), which generated good results for symptomatic KOA in the present study. The clinical implications of this study can be summarized as follows: (i) O2O3 infiltration into the painful knees of patients with KOA has a beneficial effect and can serve as a good adjunct to other rehabilitation therapies (in our case, mFV) or be used in the preparatory phase for rehabilitative therapeutic exercises, and (ii) the adoption of this altogether short protocol has low costs for the patient.
This study also has three main limitations. First, it was a prospective observational study, not a clinical randomized controlled study (such as a randomized controlled trial). Second, it did not include a third group of control patients who underwent no treatment. Finally, a longer follow-up period would have been preferable. Future studies should ideally include four groups: placebo, O2O3, mFV + O2O3, and mFV.
Conclusion
A 3-week integrated rehabilitation protocol of three once-weekly infiltrations of O2O3 and mFV reduces pain, improves autonomy in ADL, and recovers the strength of the quadriceps femoris. This study is the first attempt to document the effects of mFV with injections of O2O3 into the knees of patients with KOA, and the data will serve as a useful reference in common clinical rehabilitation practice. Future clinical trials are suggested to further develop our results and provide evidence of long-term efficacy.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520986705 - Supplemental material for Integration of focal vibration and intra-articular oxygen–ozone therapy in rehabilitation of painful knee osteoarthritis
Supplemental material, sj-pdf-1-imr-10.1177_0300060520986705 for Integration of focal vibration and intra-articular oxygen–ozone therapy in rehabilitation of painful knee osteoarthritis by Teresa Paolucci, Francesco Agostini, Andrea Bernetti, Marco Paoloni, Massimiliano Mangone, Valter Santilli, Letizia Pezzi, Rosa Grazia Bellomo and Raoul Saggini in Journal of International Medical Research
Footnotes
Acknowledgement
We are grateful to Alessia Bramanti of the Institute for Treatment, Care and Research, Center of Neurolesi “Bonino Pulejo.” (Messina, Italy) for her collaboration and suggestions.
Data availability
The datasets that were used or analyzed during the present study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.