
Abstract
Objective
This study was performed to investigate the influence of a standard Oxford vertical cut on the coronal coverage and rotation of the tibial component and determine whether a relationship exists between coverage and rotation.
Methods
We retrospectively analyzed 71 patients with anteromedial osteoarthritis of the knee treated by Oxford unicompartmental knee arthroplasty in one center from October 2016 to October 2017. The distance of coronal coverage was measured on a postoperative anteroposterior view of the tibial component. Two different reference lines between the lateral wall of the tibial component were defined as rotation angle α and β, respectively, on a computed tomography scan.
Results
The mean distance was 0.3 ± 1.1 mm. The mean angle α and β were 5.7° ± 4.6° and 8.4° ± 4.6°, respectively. There were no significant differences in the distance according to the tibial component rotation or in the α and β angles according to the coronal coverage. No significant correlation was found between the α and β angles and the distance.
Conclusion
A standard tibial vertical cut caused various changes in coronal coverage and rotation of the tibial component. The rotation of the tibial component did not affect coverage within a certain range.
Keywords
Introduction
With the development and maturity of unicompartmental knee arthroplasty (UKA) technology, an increasing number of people with unicompartmental osteoarthritis of the knee have options other than total knee arthroplasty. Mobile-bearing medial UKA yields good clinical outcomes 1 and higher patient satisfaction 2 , 3 than total knee arthroplasty because of the following unique advantages: minimal invasiveness, ligament preservation, faster recovery, and near-natural knee kinematics. The Oxford Knee implant has had great clinical results since first launched 40 years ago. 4 With advances in the surgical technique and design of the Oxford Knee implant throughout three generations since the 1970s, 5 the Oxford Knee has become the most widely used and reliable UKA system worldwide.
One study showed that covering the tibial component on the tibia is one factor that affects the outcome of Oxford UKA (OUKA). 6 An overhang of the tibial component may lead to irritation of the medial collateral ligament and surrounding soft tissue. In addition, the relative decrease in the loading area of the tibia under the tibial plateau leads to an increase in bone stress under the tibial plateau and may cause pain. 7 Underhanging of the tibial component may increase the risk of subsidence, loosening, and other complications because of the lack of medial cortical support. Rotation of the tibial component is reportedly correlated with postoperative function after OUKA. 8 , 9 No consensus has been reached regarding rotational alignment of the tibial component. From a surgical perspective, the vertical cut of the tibia is the decisive maneuver that affects placement of the tibial component and therefore the coverage and rotation of the tibial component. In our clinical practice, we have also found that after standard Oxford operative procedures, some patients do not achieve perfect coverage of the tibial component, and the rotation angle of the tibial component significantly differs among individual patients.
We investigated the influence of a standard tibial vertical cut on the coronal coverage and rotation of the tibial component and examined whether a relationship exists between the coronal coverage and rotation of the tibial component.
Materials and methods
Patients
The clinical and radiographic data of patients who underwent OUKA with Microplasty Instrumentation (Zimmer Biomet, Warsaw, IN, USA) in our center were retrospectively reviewed. We performed the operation according to the Oxford standard operative procedure. A standard prosthetic anteroposterior radiograph was obtained immediately after the operation using a C-arm X-ray machine to measure coverage of the tibia. A postoperative computed tomography (CT) scan was performed after 3 days to evaluate the tibial component rotation. Data from the patients’ medical records, including sex, age, body mass index, operated side, and tibial component size, were collected with verbal consent from the patients. We de-identified the details such that the identity of the patient may not be ascertained in any way. The review board of our institution waived the requirement for ethical approval because of the nature of the study.
Operative procedure
All operations were performed at one institution by a senior surgeon (C.G.L.) according to the standard operative procedure established by Oxford. The subpatellar fat pad was partially excised to expose the medial compartment and medial proximal tibia. The strength of the anterior cruciate ligament was tested and the integrity of the lateral compartment cartilage was confirmed before the next procedure. Osteophytes were removed from the intercondylar fossa and medial femoral condyle using a narrow osteotome so that the osteotome could directly extend into the intercondylar fossa and point toward the anterior superior iliac spine (ASIS). The femoral medullary opening hole was situated 1.0 cm anterior to the anterior edge of the intercondylar notch and 0.5 cm lateral in line with the medial wall. The intramedullary rod was pointed toward the ASIS with help from the surgical assistant. An appropriate femoral sizing spoon was connected to the extramedullary tibial guide, creating a 7° posterior slope. The tibial vertical cut was medial to the apex of the medial tibial spine, and the blade was pointed toward the ASIS parallel to the intramedullary rod (Figure 1). The horizontal cut was made under the protection of a “Z” retractor. The remaining steps of the operation, including femoral drilling, femoral posterior condyle osteotomy, femoral grinding to balance the flexion and extension gap, installing the prosthesis just along the cuts without any adjustments, bone cement fixation, irrigation, and suturing of the wound, were performed as recommended by the manufacturer.

Tibial vertical cut. (a) The tibial vertical cut was medial to the apex of the medial tibial spine. (b) The blade was pointed toward the anterior superior iliac spine parallel to the intramedullary rod. (c) A too-deep vertical cut was avoided.
Imaging measurements
A standard prosthetic anteroposterior radiograph was obtained immediately after the operation using a C-arm X-ray machine. The patient was placed in the supine position with the knee straight. The tibial component was kept in the center under the beam, and the direction of the beam was adjusted until it was aligned with the tibial component. The image in which the tibial component achieved the thinnest contour was considered a standard prosthetic anteroposterior radiograph. All tibial position measurements were made using image processing software (ImageJ; National Institutes of Health, Bethesda, MD, USA) in the following five steps (Figure 2). First, a circle was drawn according to the arc of the lower edge of the femoral component. Second, the radius of the circle was measured. Third, magnification was corrected by scaling the radius of the curvature of the spherical femoral component on the digital image by the known component size. Fourth, the distance between the medial edge of the tibial component tray and the medial border of the proximal tibia at the resection level was measured. Finally, the actual distance (d) was calculated by magnification. We defined underhanging as a d of <1 mm, overhanging as a d of >1 mm, and perfect coverage as −1 ≤ d ≤ 1 mm.

Measurement of tibial component coverage using a standard prosthetic anteroposterior radiograph. Magnification was corrected by scaling the radius of curvature of the spherical femoral component on the digital image by the known component size. The distance between the medial edge of the tibial component tray and the medial border of the proximal tibia at the resection level was measured.
All patients underwent a CT scan of the knee joint on postoperative day 3. The patients were placed in the supine position with the knees fully extended during the CT scan. Image processing software (UniSight; EBM Technologies Incorporated, Taipei, Taiwan) was used to measure two rotation angles of the tibial component (Figure 3). The angle between the line perpendicular to the tangent of the posterior tibial cortex and the lateral wall of the tibial component was defined as angle α, and the angle between the line from the center of the posterior cruciate ligament tibial attachment and the medial edge of the patellar tendon (Akagi’s line) 10 and the lateral wall of the tibial component was defined as angle β. We assigned the angles to the following categories with reference to a previous report. 8 The neutral position was defined as −1° ≤ α and β ≤ 1°. Mild external rotation was defined as 1° < α and β ≤ 5°. Moderate external rotation was defined as 5° < α and β ≤ 10°. Severe external rotation was defined as α and β > 10°. Internal rotation was defined as α and β < −1°.

Measurement of the tibial component rotation using computed tomography. (a) The angle between the line perpendicular to the tangent of the posterior tibial cortex and the lateral wall of the tibial component was defined as angle α. (b) The angle between the line from the center of the posterior cruciate ligament tibial attachment to the medial edge of the patellar tendon (Akagi’s line) and the lateral wall of the tibial component was defined as angle β.
Two independent observers performed the radiologic measurements of the distances and angles twice to ensure reliability. The average results were collected.
Statistical analysis
Based on a previous study of the rotation of the tibial component (angle α = 8.0° ± 6.1°), 11 the sample size was calculated as 55 according to the formula (with α = 0.05, two-tailed, and power of 80%). We rounded this sample size up to 76 knees in our study. All values are presented as mean ± standard deviation. The reliability of the measurements was assessed by calculating the intraclass correlation coefficients. Inter- and intra-observer reliability was defined as follows: <0.20, poor; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, good; and 0.81 to 1.00, excellent. Analysis of variance was used to compare the difference in the covering distance and rotation angle between the groups. The chi-square test was used to compare the count data of each group. Linear regression analysis was performed to assess the correlation between coverage and rotation. A P value of <0.05 indicated statistical significance. Statistical analyses were performed using SPSS version 23.0.0 (IBM Corp., Armonk, NY, USA).
Results
Seventy-five patients who underwent OUKA were included in this study. Three patients (three knees) were excluded from the study because of nonstandard prosthetic anteroposterior radiographs exhibiting excessive rotation of the components (Figure 4), resulting in inaccurate measurement of the coverage. Another patient was excluded because of loss of radiographic data. Therefore, 71 patients (76 knees) were selected for our study from October 2016 to October 2017. The patient population comprised 50 women (55 knees) and 21 men (21 knees). The average patient age was 70.8 years (range, 54–89 years). The patients were divided into groups based on the distance (d) and angles (α and β), as described above. All inter- and intra-observer intraclass correlation coefficients for the distance (d) and angles (α and β) showed excellent agreement (Table 1). The mean d was 0.3 ±1.1 mm (range, −2.4–3.5 mm). The mean α and β angles were 5.7° ± 4.6° (range, −6.4°–18.9°) and 8.4° ± 4.6° (range, −1.0°–19.1°), respectively. No tibial component showed internal rotation using Akagi’s line as a reference. There were no statistically significant differences in the patients’ sex, age, body mass index, operated side, or tibial component size between the different groups (Table 2). There were also no statistically significant differences in the distance (d) of the tibial component between the rotation groups (Table 3) or in the rotation angles (α and β) between the coverage groups (Table 4). We found no correlation between the angles (α and β) and distance (d) (Table 5). There were statistically significant differences in the proportion of perfect coronal coverage between the rotation groups divided by angle α, but not between the groups divided by angle β (Table 6).

Assessment of prosthetic anteroposterior radiograph. (a) The non-standard prosthetic anteroposterior radiograph showed an excessive rotation or slope. (b) The standard prosthetic anteroposterior radiograph was that in which the contour of the tibial component was thinnest.
Intra- and inter-observer reproducibility of radiographic measurements.
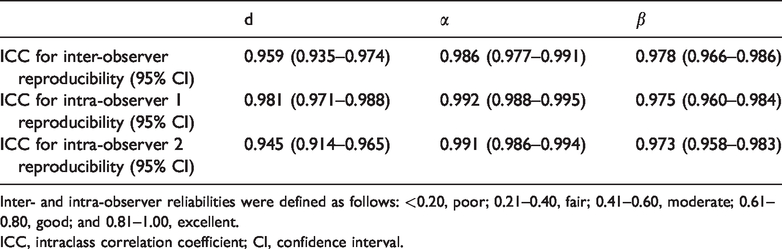
Inter- and intra-observer reliabilities were defined as follows: <0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good; and 0.81–1.00, excellent.
ICC, intraclass correlation coefficient; CI, confidence interval.
Baseline characteristics of different groups.

Data are presented as n or mean ± standard deviation.
Patients were divided into several groups based on the distance of coverage (d) and rotation angle (α and β). We defined underhang as d < 1 mm, overhang as d > 1 mm, and perfect coverage as −1 ≤ d ≤ 1 mm. A neutral position was defined as 1° ≤ α and β ≤ 1°. Mild external rotation was defined as 1° < α and β ≤ 5°, moderate external rotation was defined as 5° < α and β ≤ 10°, severe external rotation was defined as α and β > 10°, and internal rotation was defined as α and β < −1° was defined as internal rotation.
BMI, body mass index.
Comparison of distance of coverage according to rotation angle.

Data are presented as mean ± standard deviation.
Comparison of rotation angle according to distance of coverage.

Data are presented as mean ± standard deviation.
Correlation between rotation angle and distance of coverage of tibial component.

Ratio of perfect coverage according to angle rotation.
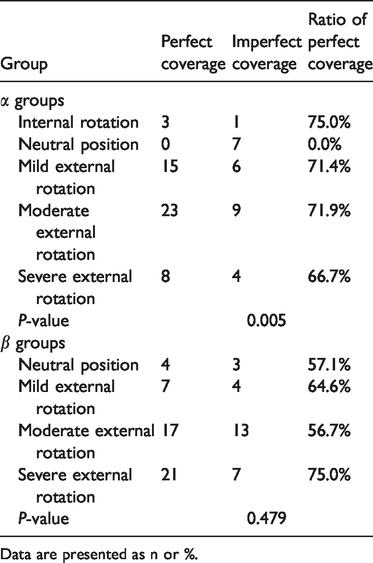
Data are presented as n or %.
Discussion
This study is the first to explore the effect of a standard Oxford tibial vertical cut on the coronal coverage and rotation of the tibial component in patients in clinical practice and to determine the presence of a relationship between the coverage and rotation. The most important finding of this study is the variability in coronal coverage and rotation of the tibial component caused by the standard tibial vertical cut in OUKA. In addition, we found that rotation of the tibial component did not affect the tibial coronal coverage when the external rotation did not exceed 20°. This finding indicates that OUKA has a greater tolerance of rotation of the tibial component and that the requirements for rotation of the tibial component are not limited to a certain position.
Coronal coverage of the tibial component in the patients in our study was not completely satisfactory. Perfect coronal coverage of the tibia was not achieved in 27 cases (35.5%). As noted by Chau et al., 6 the proportion of a “perfectly” fitting tibial component was only 3.1% under a standard vertical tibial cut in OUKA. Gudena et al. 12 reported that overhanging of the tibial component had a significant effect on the tension of the medial collateral ligament in a cadaveric study. They advised avoidance of >2-mm overhanging, 12 which is similar to the recommendation of the manufacturer. 13 When surgeons are unable to attain perfect coronal coverage of the tibia during the operation, they often follow the principle that overhanging is better than underhanging because minor overhanging may not affect patients’ outcomes or functions. Moreover, underhanging may increase the possibility of subsidence and loosening of the tibial component in the long term because of the lack of support provided to the tibial component by the medial cortex.
We evaluated the rotation of the tibial components using two reference lines. When the line perpendicular to the tangent of the posterior tibial cortex was used as the reference line, 7 tibial components (9.2%) were internally rotated (range, −6.4° to −0.4°), 69 tibial components (90.8%) were externally rotated (range, 0.3°–18.9°), 3 tibial components (3.9%) were internally rotated (range, −1.0° to −0.2°), and 73 tibial components (96.1%) were externally rotated (range, 0.3°–18.9°) relative to Akagi’s line. We found that regardless of which reference line was used to measure the rotation of the tibial component, most of the reference lines were in relative external rotation, and the maximum external rotation did not exceed 20° with large variability of the rotation angle.
Our findings are in agreement with previous reports. With respect to studies of fixed-bearing UKA with all-polyethylene tibial components, Campbell et al. 14 reported that the tibial component was externally placed at 6.59° ± 7.23° relative to the posterior tibial cortex line and at 5.68° ± 6.77° relative to the projected femoral transepicondylar axis. Two other studies showed that the external rotation angle was 6.5° ± 5.1° and 11.9° (range, −1°–32°) relative to the line perpendicular to the tangent of the posterior tibial cortex.8,15 With respect to the Oxford mobile-bearing tibial components, Lee et al. 11 reported that the tibial component was implanted with external rotation of 8.0° ± 6.1° and 8.7° ± 4.8° relative to the line perpendicular to the tangent of the posterior tibial cortex and Akagi’s line, respectively. Kamenaga et al. 9 reported that the tibial component was 4.00° ± 4.60° externally rotated relative to Akagi’s line and 8.7° ± 4.8° externally rotated relative to the line perpendicular to the surgical epicondylar axis. Notably, a standard tibial vertical cut was performed in both studies, and the variation of the tibial component rotation was distinct. This indicates that the direction of the standard tibial vertical cut did not guarantee a fixed rotation angle in which the tibial component was implanted.
We placed the tibial component just along the tibial vertical cut without adjusting its rotation and coronal coverage, and we found no statistically significant differences in the tibial component size between the groups. Therefore, the vertical cut was the sole factor affecting coronal coverage and rotation in our study. With respect to sagittal coverage, which was not evaluated, the tibial component was flush with the posterior cortex as recommended by the manufacturer. It was not affected by the vertical cut. Additionally, there is no evidence that sagittal coverage is related to complications or clinical outcomes.
No correlation was found between coverage and rotation of the tibial component in our study. However, we found a statistically significant difference in the proportion of perfect coverage between the rotation groups divided by angle α (P = 0.005) (Table 6). We believe that this difference was due to the component being in the neutral position (−1°–1°) in seven cases, all of which failed to achieve perfect coverage of the tibial component. This finding suggests that even when good results are achieved in controlling the rotation of the component, the coverage of the tibial component might remain unsatisfactory. Kamenaga et al. 16 first discovered that a correlation existed in a CT simulation study. External rotation of the tibial vertical cut can lead to overhanging of the tibial component. In contrast, internal rotation results in underhanging of the tibial component. We believe that this computer simulation of surgery is an idealized study; more factors are involved in the actual operation. An important factor that cannot be ignored is the difference in the tibial plateau anatomy between Chinese and Western populations. Evidence indicates that the anteroposterior and mediolateral lengths of the tibial plateaus of Chinese people are generally smaller than those of Westerners, and the design parameters of the Oxford prosthesis mainly refer to the anthropometric data of Westerners, leading to a low anatomic match between the design of the tibial component and the characteristics of Asians. 17 , 18
The standard tibial vertical cut is difficult to perform accurately because of the minimally invasive incision, small operative space, and difficulties in identification of anatomic markers. This causes variability in the coronal coverage and rotation of the tibial component in OUKA. Therefore, some surgeons select different tibial vertical cut directions according to different anatomic markers based on their own clinical experience. Some surgeons perform the tibial vertical cut along the anteroposterior line of the lateral wall of the medial femoral condyle, which Kawahara et al. 19 showed to be parallel to the anteroposterior line of the tibia. Shakespeare et al. 20 demonstrated a smaller variation in tibial component rotation by referring to the midline of the medial femoral condyle to perform the tibial vertical cut. Tsukamoto et al. 21 also achieved good clinical results by referring to the line connecting the medial border of the patellar tendon at the articular surface level and the medial intercondylar tubercle. In addition, Kawahara et al. 22 reported that the medial one-sixth of the patellar tendon at its attachment would be a useful landmark in aligning the tibial component, but the clinical value is not exact.
This study has several limitations. First, the study population comprised the first patients treated by OUKA in our hospital; therefore, the results may have been affected by the learning curve. Second, because of the lack of clinical outcomes, the study cannot provide strong clinical guidance. Finally, we paid more attention to the coronal coverage than sagittal coverage. On the one hand, the tibial component was planted flush with the posterior cortex as recommended by the manufacturer, preventing problems with sagittal coverage in the posterior region. On the other hand, few studies to date have been performed to assess the clinical outcome with sagittal coverage. Although we did not identify the ideal tibial component rotation without referring to the recommendation of the manufacturer, we still found that a standard tibial vertical cut caused variability in the coronal coverage and rotation of the tibial component. Our further research will focus on how to select a highly operable and repeatable position and direction of a vertical tibial cut using clear anatomic markers to ensure a good position of the tibial component and verify it with reliable follow-up results.
Conclusion
A standard tibial vertical cut caused variability in the clinical results of coronal coverage and rotation of the tibial component in OUKA. The rotation of the tibial component did not affect the coronal coverage within a specific range.