
Abstract
The majority of adults with mild osteogenesis imperfecta report significant functional impairment due to musculoskeletal concerns. Knee osteoarthritis is common in these patients. Although total knee arthroplasty has become a highly efficient surgical technique for osteoarthritis, this procedure remains uncommon in patients with osteogenesis imperfecta. This current case report describes the important clinical aspects of osteogenesis imperfecta that must be considered during the planning and performance of a total knee replacement. A 62-year-old female patient with a history of osteogenesis imperfecta suffered from severe osteoarthritis of the knee with valgus deformity. Two years after posterior stabilized total knee arthroplasty, her Hospital for Special Surgery knee score had improved from preoperative 53 points to 85 points at the final follow-up. The current case report describes the crucial technical aspects of a successful total knee replacement in this uncommon scenario. Underlying deformities and concomitant pathologies constitute specific surgical challenges. Special care should be taken to protect the patient from potential complications.
Introduction
Osteogenesis imperfecta comprises a phenotypically and molecularly heterogeneous group of inherited connective tissue disorders characterized by abnormal bone fragility resulting in easy susceptibility to fractures, bone deformities and growth deficiency. 1 Osteogenesis imperfecta has an estimated birth prevalence of approximately 6–7/100 000. 2 Historically, the Sillence classification categorized the disease into four types based on clinical and radiographic features. 3 Defects in proteins with miscellaneous functions, ranging from structural to enzymatic and from intracellular to chaperones, have been described in the sixteen currently recognized types of osteogenesis imperfecta. 4 Although the shorter survival of patients with osteogenesis imperfecta is associated with more severe phenotypes, osteogenesis imperfecta is a lifelong disorder with significant impairment throughout adulthood. 5 Depending on the location of the mutations, abnormal molecular characteristics of collagen type I increase the risk of periarticular and diaphyseal fractures that alter joint biomechanics. 6 Periarticular bone dysplasia with subchondral insufficiency may accelerate the development of osteoarthritis. 1 Conservative therapy of osteoarthritis is usually recommended in adults with osteogenesis imperfecta. 7 However, some patients may be dissatisfied with the results of conservative therapy alone. The implantation of a total knee arthroplasty is a highly efficient surgical technique but, to the best of our knowledge, very few cases of total knee arthroplasty in adult patients with osteogenesis imperfecta have been published to date.8,9
This current case report describes a patient with osteogenesis imperfecta that suffered from valgus deformity of the right knee with severe osteoarthritis that was corrected by total knee arthroplasty. In addition, the available literature and current technical remarks on the management of this uncommon scenario are reviewed.
Case report
In May 2019, a 62 year-old female patient with osteogenesis imperfecta presented at the Department of Orthopaedic Surgery, University Hospital in Hradec Kralove, Hradec Kralove, Czech Republic with a 5-year history of pain in the right knee. She was diagnosed with a mild form of osteogenesis imperfecta during childhood because of multiple fractures, blue sclerae and short stature. Recent fractures occurred in her left proximal tibia and left distal radius 5 years previously and in the right ankle 2 years ago previously. Before surgery, bone fragility was addressed with subcutaneous injection of 60 mg denosumab every 6 months for 12 months (Prolia®; Amgen, Thousand Oaks, CA, USA). At the time of presentation, the patient was 153 cm tall and weighed 85 kg. The medical comorbidities included hypertension, asthma, mechanical aortic valve replacement with long-term anticoagulation, mild mitral and tricuspid regurgitation, mild pulmonary hypertension and osteoporosis. The patient did not smoke. Bone mineral density of the upper femur evaluated by dual-energy X-ray absorptiometry was 0.523 g/cm2 and the T-score was 56%. Physical examination showed valgus deformity of the right knee with a range of motion from 0° to 100°. A long-standing anteroposterior radiograph revealed 25° of genu valgum deformity with osteoarthritis (Figures 1 and 2). Conservative management including 1–2 tablets daily of 37.5 mg tramadol/325 mg acetaminophen (Actavis Group, Hafnarfjördur, Iceland), a knee brace and physical therapy did not relieve her symptoms. The patient elected to proceed with right total knee replacement after discussing the risks and benefits of the surgery.

A preoperative long-standing anteroposterior radiograph of the lower extremity of a 62 year-old female patient with osteogenesis imperfecta that presented with a 5-year history of pain in the right knee shows a 25° of genu valgum deformity with osteoarthritis.

A preoperative lateral radiograph of the right knee of a 62 year-old female patient with osteogenesis imperfecta that presented with a 5-year history of pain in the right knee shows degenerative changes of the patellofemoral joint.
The right total knee arthroplasty (NexGen® Complete Knee Solution; Zimmer Biomet, Warsaw, IN, USA) was performed trough a midline longitudinal skin incision without tourniquet inflation. Once standard medial parapatellar arthrotomy was complete, the patella was everted and the distal part of the femur was osteotomized at 6° of valgus using conventional intramedullary femoral guide. After posterior cruciate ligament resection, the proximal tibia was cut utilizing an intramedullary guide with the goal of cutting the bone perpendicular to the upper tibial axis. The rotation was set referencing the middle of the tibial tubercle. When distal femoral and proximal tibial cuts were completed, the lateral osteophytes were removed and the extension gap was evaluated. As the knee was tighter in extension, the posterolateral capsule and the iliotibial band were released. After tibial sizing, a 30-mm stem extension was selected to support fixation in the tibia considering the presence of metaphyseal osteopenia and tibial extraarticular deformity not amenable to a diaphyseal engaging stem. The shaft was reamed gently without complications. The rotation of the femur was based on the transepicondylar axis. After sizing the distal femur, femoral chamfer and box cuts were made. Both trial components fitted adequately and in correct rotational alignment with good patella tracking; however, proper balance of the extension gap could not be achieved due to the tension of lateral structures. With regard to the identified tight knee in extension with the flexion gap balanced, strong fibrous strands of the iliotibial band attached to the distal femur were dissected. After placement of the trial posterior-stabilized implants, the extension and flexion gaps were balanced. Small cavitary defects in the medial femoral condyle and medial part of the upper tibia were filled with autologous bone grafts. A restrictor was placed to improve the cement mantle and prevent cement from extruding down the medullary canal. The cement was pressurized to achieve a robust cement mantle within the tibial metaphysis. The definitive tibial implant with a 30-mm tibial stem extension and posterior-stabilized femoral condylar implant were cemented. The patella was not resurfaced because degenerative changes were minimal. The wound was closed with a suction drain.
Antibiotic prophylaxis using 2 g cefazolin was administered intravenously 30 min prior to surgery and continued for 24 h (the same dose repeated after 4, 6 and 6 h). Subcutaneous injections of 0.4–1.0 ml/day of nadroparin (Fraxiparine®; 9500 AXa ICU; Sanofi, Paris, France) were given to prevent thromboembolic disease for 6 weeks proceeding to 3 mg/day of oral warfarin as long-term anticoagulation due to mechanical aortic valve replacement. Physiotherapy started at post-operative day 1. Partial weight-bearing walking was allowed immediately after surgery, proceeding to full weight-bearing at 6 weeks postoperatively.
After 6 weeks, the patient reported complete resolution of her right knee pain. She had a painless range of motion from 0° to 130°. Two years later, the patient had no pain and ambulated with the help of elbow crutches. Her Hospital for Special Surgery knee score increased from preoperative 52.5 points to 85.25 points at the final follow-up. Radiography revealed correct knee alignment without signs of implant loosening (Figure 3). The patient was satisfied with the therapeutic process and results because of the complete resolution of her knee pain, full correction of the valgus knee deformity and improved range of motion. No adverse and unanticipated events were identified.
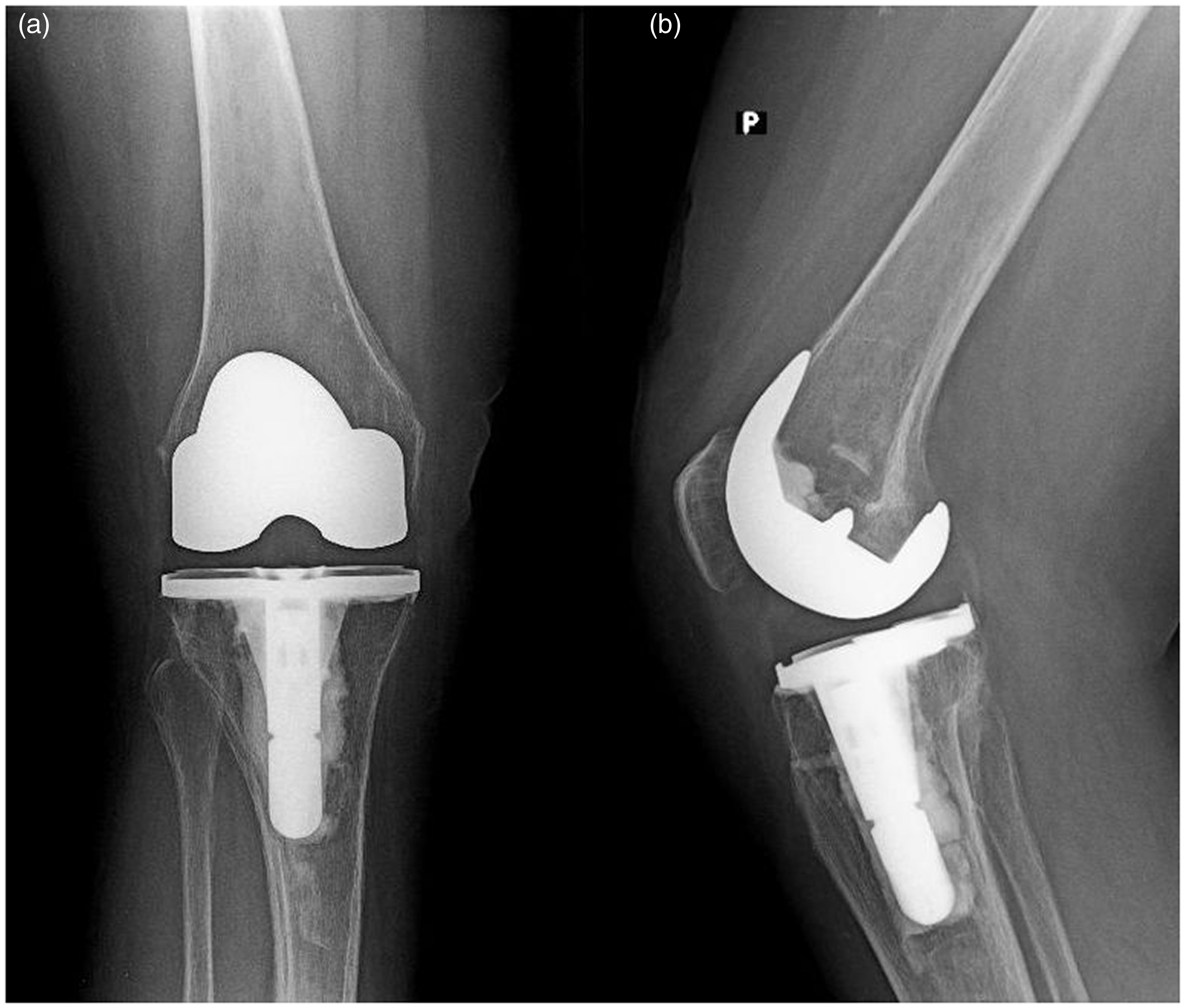
Postoperative radiographs of the right knee taken 2 years after surgery show correct knee alignment without signs of implant loosening: (a) anteroposterior and (b) lateral views.
Written informed consent was obtained from the patient. The approval of the institutional review board was not required in this regard. The patient provided approval for her images and information to be used in this work and for them to be published in this journal. The reporting of this study conforms with the CARE guidelines. 10
Discussion
Although most of the literature focuses on the paediatric manifestations of osteogenesis imperfecta, the disease is a lifelong disorder with significant impairment that presents throughout adulthood. 11 A multidisciplinary approach is necessary for the effective management of the disease. Medical therapy is focused on the increase of bone mineral density, reduction of fracture risk and pain management. 7 All but the most impaired patients benefit from maintaining a regular exercise programme and an active lifestyle. 12 Occupational therapists provide lifestyle modifications including aids to daily living and mobility. Multidisciplinary care includes nutritional consultation, psychological and social support. Regular monitoring of dentition, hearing, the cardiovascular system and pulmonary evaluation should be performed. 7
Although fracture rates decline considerably after reaching skeletal maturity, even adults with mild osteogenesis imperfecta continue to sustain fractures into adulthood. The majority of adults with mild osteogenesis imperfecta report significant functional impairment due to musculoskeletal concerns. 13 Knee osteoarthritis is common in patients with osteogenesis imperfecta. 8 Total knee replacement has become a highly efficient surgical technique for primary osteoarthritis but this procedure still remains uncommon in patients with osteogenesis imperfecta. To the best of our knowledge, only 12 total knee replacements in 10 patients with osteogenesis imperfecta and knee osteoarthritis have been reported in the existing literature.8,9,14–18 The characteristics of the previously published cases are presented in Table 1.8,9,14–18 One additional case report described a failed hip femoral revision component perforating the femoral trochlea due to poor bone quality that was treated by total femur replacement. 19
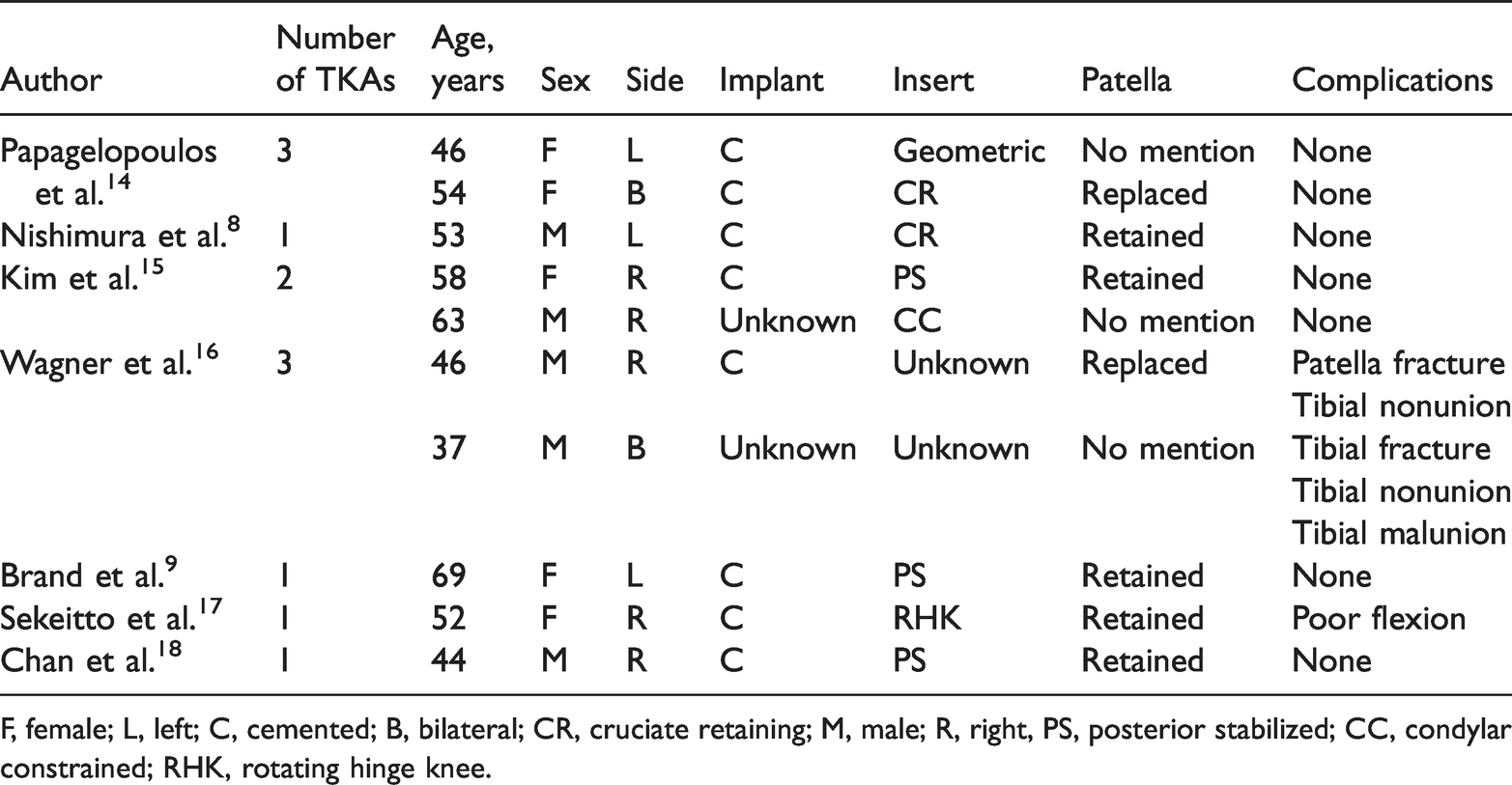
F, female; L, left; C, cemented; B, bilateral; CR, cruciate retaining; M, male; R, right, PS, posterior stabilized; CC, condylar constrained; RHK, rotating hinge knee.
Regarding joint replacement, patients with osteogenesis imperfecta require special care. Typically, patients with osteogenesis imperfecta are at risk for iatrogenic cervical fracture caused by manipulation of the cervical spine during general anaesthesia. Thus, epidural anaesthesia or regional block may be beneficial. Moreover, preoperative evaluations should include cervical spine imaging to identify subclinical fracture or instability. 14 To minimize the potential of other iatrogenic fractures, the operating table must be well padded and the patient should be handled cautiously. 14
Bowing and post-traumatic deformities, axis deviations, ligament laxity and small bone size should be considered during the preoperative planning. A full-length, weight-bearing lower extremity radiograph is required to properly evaluate the mechanical and anatomical axis alterations. The surgeon should ensure that a sufficient range of implant sizes is available preoperatively. 9 Subchondral bone in patients with osteogenesis imperfecta is less dense and possesses few trabeculae. 8 Thus, the use of cemented implants is recommended.7,8 Osteopenia is the most important risk factor for iatrogenic intraoperative and postoperative periprosthetic fractures. 7 Therefore, the surgical team should be vigilant in monitoring for such events during the procedure. Ligamentous laxity was reported in approximately 56% of patients with osteogenesis imperfecta. 11 Soft tissue balancing may be performed to achieve symmetrical extension and flexion gaps once the deformity is corrected. 20 When adequate soft tissue balancing is not obtained, then the use of constrained implants should be considered to achieve satisfactory stability. Unfortunately, the downside to this approach includes an increased risk of earlier aseptic loosening secondary to the increased inter-component constraint.
The current patient was satisfied with the short-term clinical result. Based on this case report, the surgeon should consider sacrificing the posterior cruciate ligament in total knee arthroplasty with intra-articular correction of severe valgus deformity of the knee to improve intra-operative tibial mobility with a decreased risk of intraoperative femoral condyle or tibial fracture. Despite the removal of the lateral osteophytes with release of the posterolateral capsule and the iliotibial band release from Gerdy’s tubercle, a tight knee in extension with balanced flexion gap was identified during surgery. Dissection of the strong fibrous strands of the iliotibial band attached to the distal femur was efficient in addition to soft tissue balancing. 21 To minimize the risk of patellar fracture, the patella was not resurfaced because of minimal degenerative changes of the patellar facets and lower thickness of the patella combined with osteopenia.
In conclusion, although there are only a few published cases of knee replacement in patients with osteogenesis imperfecta, total knee replacement may be a beneficial strategy for active patients with this disorder. Underlying deformities and concomitant pathologies constitute specific surgical challenges. Special care should be taken to protect the patient from potential complications. A clear emphasis should be placed on careful planning in the preoperative period and vigilant monitoring during and after the surgical intervention.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221097369 - Supplemental material for Challenges of total knee arthroplasty in osteogenesis imperfecta: case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221097369 for Challenges of total knee arthroplasty in osteogenesis imperfecta: case report and literature review by Pavel Sponer, Martin Korbel and Tomas Kucera in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cooperatio Program (research area SURG) and MHCZ – DRO (UHHK, no. 00179906).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.