
Abstract
Objective
This study aimed to determine the relationship between serum testosterone levels and depressive symptoms in an adult male population.
Methods
We conducted a cross-sectional study of 1166 male participants from Zunyi, Guizhou, China. Each participant completed a questionnaire, a brief clinical exam, and had a fasting blood sample taken. We measured serum testosterone, sex hormone-binding globulin, and luteinizing hormone levels. Multiple linear regression was used to evaluate the effect of demographic factors on the relationship between the depressive symptom score and serum sex hormone levels.
Results
Mean testosterone, sex hormone-binding globulin, and luteinizing hormone levels were significantly higher in the depressive symptom group than in the non-depressed group. The mean calculated free serum testosterone level and free testosterone index (FTI) were significantly lower in the depressive symptom group than in the non-depressed group. Additionally, the mean FTI was significantly negatively correlated with the Beck Depression Inventory scale score in the multiple linear regression model (95% confidence interval: −3.274 to −0.406).
Conclusions
Decreased bioactive testosterone levels might be a contributing factor of depression in adult men. The FTI could be the most sensitive biomarker reflecting the level of bioavailable testosterone in patients with depression.
Keywords
Introduction
Depression is a clinical manifestation of mood disorders and is characterized by a significant and persistent negative emotional state, with high morbidity, relapse, disability, and mortality rates. Various factors contribute to the occurrence of depression, and it constitutes the largest disease burden worldwide. 1 According to the latest report from the World Health Organization, by 2020, depression will be the second leading cause of disability worldwide. 2 Therefore, understanding the etiology of depression is critical for developing and identifying targeted and effective treatment strategies.
The underlying mechanisms of depression remain unclear. Risk factors for depression involve biological, psychological, and social factors. Among psychosocial factors, poor socioeconomic conditions, occupational and negative life events, and a history of major depression increase the risk for depression in men. 3 Notably, abnormal levels of physiological hormones, especially sex hormones, such as testosterone, are associated with male depression. In vivo studies have shown that intraperitoneal administration of testosterone rapidly activates the hippocampus and medial cortex areas. 4 Testosterone activation not only contributes to anxiolytic behavior in rodents, but also to antidepressive-like behavior. 5 However, whether testosterone levels are associated with depressive symptoms in population epidemiological studies remains controversial.6–19 Therefore, the association between testosterone levels and depressive symptoms requires further investigation.
Such inconsistent results are likely due to application of different indicators of testosterone levels. Only 2% to 3% of circulating plasma testosterone is in the free form. In men, approximately 44% to 65% of circulating testosterone is bound to sex hormone-binding globulin (SHBG) and 33% to 54% to albumin. Testosterone bound to SHBG loses its biological activity because of the tight binding. 5 Notably, testosterone levels are not completely correlated with bioavailable testosterone levels. Another reason for the inconsistent results is that most previous studies failed to adjust for confounders, which affect depressive symptoms and testosterone levels.20–23
The present study aimed to examine the levels of male androgens and free testosterone using large-sample, epidemiological, cross-sectional survey data. Demographic information, such as age, physical condition, and disease status of men, were collected, and the depression status of men was evaluated with the Beck Depression Inventory (BDI) scale to examine the association between bioactivity of testosterone levels and symptoms of depression. Additionally, a multivariate linear model was used to adjust for the effects of potential confounders.
Methods
Subjects
We conducted this cross-sectional study from August to September 2013 in Zunyi, which is located in the north of Guizhou Province, China. We used a stratified cluster design to select sample communities. According to the lifestyle and economic conditions of the residents, 80 communities within 50 km from the city center were divided into three areas of urban, suburban, and village, and seven communities were targeted (two urban communities, two suburban communities, and three village communities). Men older than 18 years from the seven communities participated in a questionnaire and a brief clinical exam voluntarily among those who were not taking antidepressants or other medications.
A total of 1213 participants were initially recruited. The exclusion criteria for this study were based on reports from previous studies. 24 Men were excluded for the following reasons: diagnosed cardiac, kidney, or liver disease (n = 11), pituitary-testicular disease (n = 1), and drug abuse (n = 4). Additional exclusion criteria included incomplete or illogical questionnaire responses (n = 29) and insufficient or non-fasting blood samples (n = 2). Forty-seven men were excluded because they did not have questionnaires, serum samples, or non-fasting blood samples. A flow chart of selection of the subjects is shown in Figure 1.

Flow chart of the participants.
Study design
This study was approved by the Ethical Committee Review Board of Tongji Medical College in the Huazhong University of Science and Technology. All participants were required to sign an informed consent form before inclusion in the study. Each person was anonymous for research and confidentiality purposes. Demographic information and socioeconomic data, such as age, medical history, smoking status, alcohol use, and occupation, which had been identified as significant factors affecting hormone concentrations, were also collected.25–28 All variables were classified using standard clinical classification or sociodemographic attributes.
Symptoms of depression were measured using the short 13-item BDI-13. This questionnaire includes 13 questions, and each question is scored between 0 and 3 for a maximum score of 39. Patients were classified according to their total scores on the BDI as follows: scores of 0 to 4, no depression; 5 to 7, mild depression; 8 to 15, moderate depression, and ≥16, severe depression.29–31 In this study, BDI scores of 0 to 4 were set as the criterion for inclusion in the non-depressed group, and scores of 5 to 39 were defined as the depressive symptom group.31–33
Trained researchers measured weight, height, waist circumference, systolic blood pressure (SBP), diastolic blood pressure (DBP), and the waist (cm)/height (cm) (WHR) ratio. Fasting venous blood samples were collected by trained nurses and centrifuged at 4°C for 15 minutes at 1728 ×g to obtain serum and stored at −80°C until later analysis.
Laboratory assessments
Chemiluminescent immune assays were used to measure testosterone, SHBG, and luteinizing hormone (LH) levels on a Beckman Access Immunoassay system (Beckman Coulter, Inc., Brea, CA, USA). Calculated free serum testosterone (cFT) was quantified using Vermeulen’s formula and calculated as follows: free testosterone (nmol/L) = −a +
Statistical analyses
Data were proofread, entered in EPIdata version 3.02 (Odense, Denmark), and analyzed using SPSS version 18.0 (IBM Corp., Armonk, NY, USA). Graphics were produced by using GraphPad Prism 7 (GraphPad Software Inc., La Jolla, CA, USA). We recoded independent variables in multiple models into binary variables. In all hypothesis testing, when the p value was <0.05, we rejected the null hypothesis.
Quantitative data are presented as mean ± standard deviation and categorical data as frequency (%). The t-test was used to assess differences between the groups regarding sex hormone levels, the BDI, age, WHR, blood glucose, SBP, DBP, occupation, education, marital status, smoking status, alcohol use, vasectomy, and symptoms of depression. One-way analysis of variance was used to assess differences between sex hormone levels and the BDI in relation to body mass index (BMI). Comparison of androgen levels and depressive symptom scores with BMI was performed used the SNK method of analysis of variance. The effect of hormone concentrations and other sociodemographic variables on BDI scores was assessed using a multiple linear regression model, and the results were presented as the beta value and 95% confidence interval (CI).
A multivariable linear regression model was developed for each hormone, which was regarded as a dependent variable, and the demographic and lifestyle characteristics were independent variables. The enter method was recruited in the model with entry level equal to 0.05 and removal level equal to 0.10. The adjusted models took into account age, BMI, WHR, blood glucose, SBP, DBP, occupation, education, marital status, smoking status, alcohol use, and vasectomy status. Independent variables for multivariable linear regression included age (continuous), BMI (continuous), WHR (≤0.5 vs. 0.5), blood glucose (continuous), SBP (continuous), DBP (continuous), occupation (farmer vs. not a farmer), education (≤6 vs. 6), marital status (married vs. not married), smoking status (current vs. never or former), alcohol use (current vs. never or former), and vasectomy status (yes vs. no).
Results
Demographic and lifestyle characteristics
Among the 1166 male subjects who were included, 310 were diagnosed as having depressive symptoms and 856 had no depressive symptoms, and the incidence of depression was 26.59%. The mean BDI score was 3.51 ± 4.29, the mean age was 51.6 ± 12.82 years, and the mean BMI was 23.84 ± 3.43 kg/m2. With regard to occupation, 81.99% of the participants were farmers, 43.14% had ≤6 years of education, 93.48% were married, 21.18% were current smokers, and 42.71% were currently drinking (Table 1).
Demographic and lifestyle characteristics.

SD = standard deviation; BDI = Beck Depression Inventory; BMI = body mass index; WHR = waist to height ratio; SBP = systolic blood pressure; DBP = diastolic blood pressure; BG = blood glucose; SBP = systolic blood pressure.
Serum testosterone levels and BDI scores related to lifestyle and demographics
The relationships between hormone concentrations, BDI, and categories of demographic and lifestyle variables are shown in Table 2. The mean testosterone level was significantly different according to BMI, WHR, SBP, DBP, occupation, and marital status (all p < 0.05). Furthermore, the mean SHBG level was significantly different according to age, BMI, WHR, blood glucose, DBP, occupation, education, and alcohol use (all p < 0.05). Additionally, the mean BDI was significantly different according to age, BMI, blood glucose, education, and marital status (all p < 0.05).
Sex hormones and BDI scale scores in relation to lifestyle and demographic factors.

Values are mean ± standard deviation. BDI = Beck Depression Inventory; TT = total testosterone; SHBG = sex hormone-binding globulin; cFT = calculated free testosterone; TSI = testosterone secreting index; LH = luteinizing hormone; BMI = body mass index; WHR = waist to height ratio; BG = blood glucose; SBP = systolic blood pressure; t (p) = the t-test value and p value; F (p) = one-way analysis of variance F value and p value. The model for each hormone includes all variables listed in the table. a: p < 0.05, compared with <65 years; b: p < 0.05, compared with a BMI <18.5 kg/m2; c: p < 0.05, compared with a BMI of 18.5 to 24.9 kg/m2; d: p < 0.05, compared with a WHR ≤0.5; e: p < 0.05, compared with BG levels ≤6.2; f: p < 0.05, compared with SBP ≤140 mmHg; g: p < 0.05, compared with DBP ≤90 mmHg; h: p < 0.05, compared with farmers; i: p < 0.05, compared with an education level of ≤6 years; j: p < 0.05, compared with married; k: p < 0.05, compared with current smoking; l: p < 0.05, compared with current alcohol use; m: p < 0.05, compared with having vasectomy.
Association between depressive symptomatology and serum testosterone levels
Mean testosterone, SHBG, and LH levels in the non-depressed group were significantly lower than those in the depressive symptom group (all p < 0.05). Furthermore, the mean cFT level and FTI in the non-depressed group were significantly higher than those in the depressive symptom group (both p < 0.05). Additionally, the mean TSI in the non-depressed group appeared to be higher than that in the depressive symptom group, but this was not significant (Figure 2).
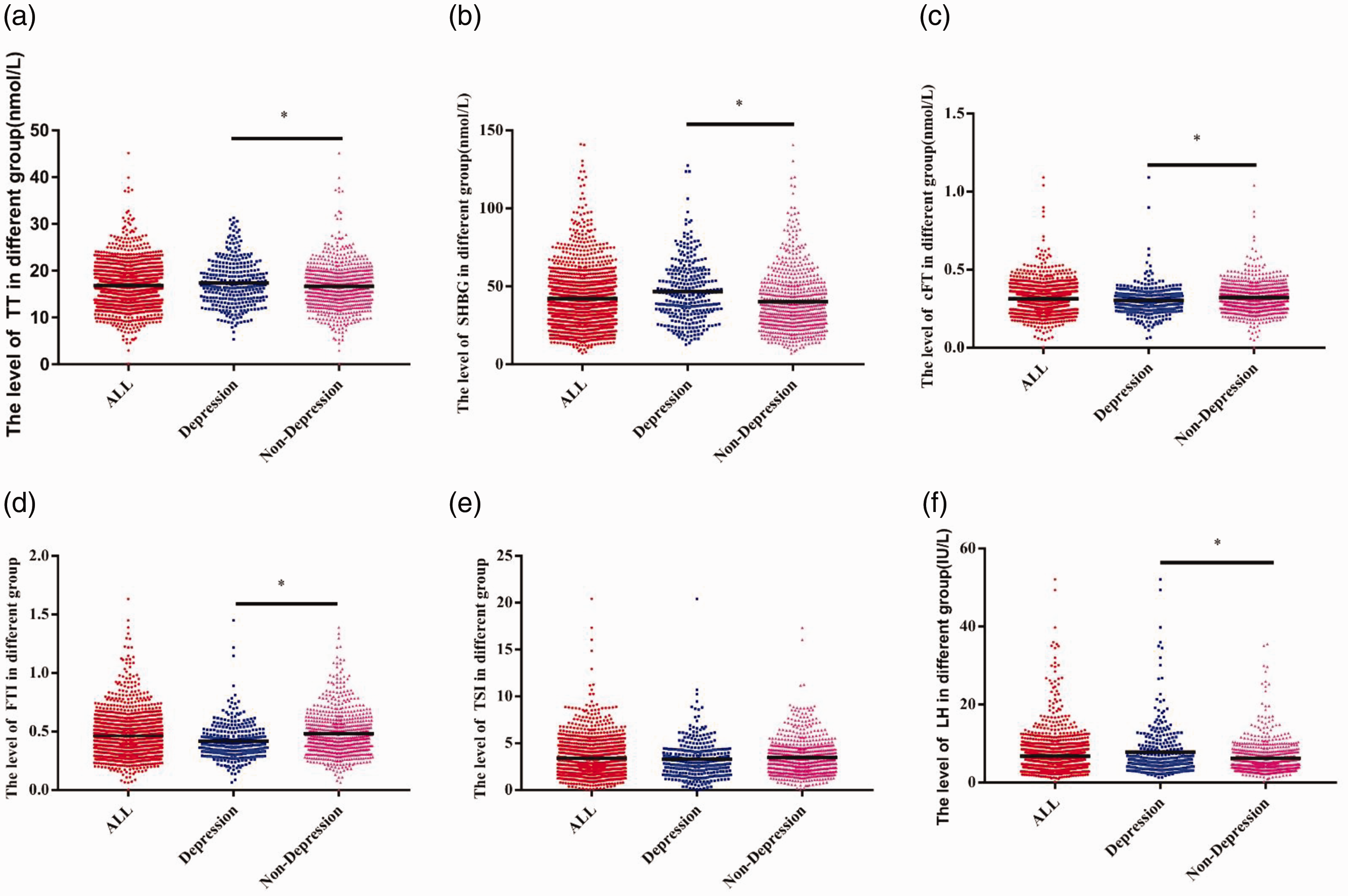
Association between depressive symptomatology and serum testosterone levels. (A) Testosterone levels in the different groups, (B) SHBG levels in the different groups, (C) cFT levels in the different groups, (D) FTI in the different groups, (E) TSI in the different groups, and (F) LH levels in the different groups.
Multivariable linear regression coefficients for hormone concentrations related to BDI scores
After adjusting for age, BMI, WHR, blood glucose, SBP, DBP, occupation, education, marital status, smoking status, alcohol use, and vasectomy status in the multiple linear regression model, only the FTI was significantly negatively correlated with the BDI score (95% CI: −3.274 to −0.406, p = 0.012) (Table 3).
Multivariable linear regression coefficients for sex hormone concentrations related to Beck Depression Inventory scale scores.

CI = confidence interval; TT = total testosterone; SHBG = sex hormone-binding globulin; cFT = calculated free testosterone; FTI = free testosterone index; TSI = testosterone secreting index; LH = luteinizing hormone.
Discussion
In this study, mean serum levels of testosterone, SHBG, and LH in the depressive symptom group were significantly higher than those in the non-depressed group. Additionally, mean serum cFT levels and the FTI were significantly lower in the depressive symptom group than in the non-depressed group. These results are consistent with Joshi et al.’s findings. 14 We found that the changes in testosterone and cFT were not consistent between the depressive symptom group and the non-depressed group. The reason for this finding may be that bioactive testosterone levels in the human body are not consistent with serum testosterone levels. 5 Another reason may be that the increase in circulating SHBG levels in patients with symptoms of depression decreases serum bioavailable testosterone levels,5,33 which excite negative feedback regulation. This then activates the hypothalamic–pituitary–gonadal axis and the hypothalamic–pituitary–adrenal axis and promotes secretion of testosterone. 34 The above-mentioned process regulates depression and anxiety and maintains stability of mood, as shown by increased testosterone, LH, and SHBG levels, and decreased cFT levels and the FTI in our study. Therefore, male patients with depression showed disordered hormone metabolism, which might be associated with the pathogenesis of depression.
Previous data have shown that testosterone can affect secretion of monoamine neurotransmitters, 35 which are associated with anxiety and depression. 36 Testosterone affects many monoamines involved in mental illness. In terms of depression, testosterone can increase dopamine neurotransmitter release in the limbic system of the midbrain, 37 which may prevent depression-induced pleasure disorders and a related reduction in dopamine activity in reward-related brain pathways. Additionally, blood testosterone levels inhibit re-uptake of serotonin, activate tyrosine hydroxylase, and increase the transport of 1-aminobutyric acid. Once the blood level of testosterone decreases, these neurotransmitter levels decrease, finally leading to depressive symptoms.38–40
The association between demographic factors and serum testosterone levels has been reported by some epidemiological studies. After 40 years old, cFT levels gradually decrease with age. 41 Similarly, the change in the TSI is consistent with that of cFT levels.24,42 In contrast, LH and SHBG levels increase with age. 43 Notably, testosterone levels may also be affected by lifestyle factors. Previous studies have shown that smoking increases serum testosterone levels, 44 while drinking affects male reproductive hormone levels. 45 Additionally, serum testosterone levels may be associated with high blood pressure, high BMI, and diabetes.22–25,46
The onset of depression is also affected by demographic factors, such as age, education level, marital status, vasectomy, smoking, drinking, blood glucose levels, and BMI.20–23 These factors may also be related to serum testosterone levels. Therefore, these potential demographic confounding factors might misrepresent the association between depression and testosterone levels. In view of these previous findings, we performed multiple linear regression to adjust for cofounding effects of independent variables on depression symptoms, such as age, height, weight, blood pressure, chest circumference, occupation, education level, marital status, smoking, drinking, vasectomy, blood glucose levels, and BMI. We found a negative correlation between the FTI and symptoms of depression, indicating that decreased levels of bioactive testosterone might be a risk factor for male depression. Our findings are consistent with those of the Rancho Bernardo Study and of Delhez et al.47,48
In late-onset hypogonadism, cFT levels are more strongly correlated with free testosterone and bioavailable testosterone levels than testosterone levels. Therefore, serum free testosterone is believed to be more representative in reflecting bioactive testosterone levels in the blood and possesses more clinical significance for diagnosing testosterone-related disease. 49 The present study showed that depressive symptoms decreased cFT levels. Although cFT levels are closely in line with bioavailable testosterone, they are still not a comprehensive index of sex hormone disorders. The FTI is calculated by integrating testosterone and SHBG levels. The FTI not only can be used to comprehensively assess bioavailable testosterone levels in vivo, but also reflect relative levels of testosterone and SHBG, as well as comprehensively reflect the overall status of sex hormone secretion and metabolic status. In our study, only the FTI was independently negatively correlated with male depression after adjustment. This finding suggests that imbalanced testosterone metabolism may be related to the occurrence and severity of male depressive symptoms. Collectively, the FTI may be a significant biomarker reflecting testosterone metabolism and decreased bioactive testosterone levels.
This study analyzed a large sample to determine the association between serum testosterone levels and the morbidity of depression in adult men. Nevertheless, biases of our study should be considered, such as the fact that all of the subjects were from Zunyi City, the majority of whom were farmers, and there may also have been regional differences in BDI scores. Multi-city, large-sample studies are required to confirm this study’s results and reduce regional bias. Cross-sectional data of this study indicate that the causal relationship between serum testosterone levels and depressive symptoms remains unclear.
Conclusions
Decreased levels of bioactive testosterone might contribute to depression in men. Importantly, our results indicate that the FTI could be the most sensitive biomarker reflecting the bioavailable testosterone level in patients with depression.
Footnotes
Acknowledgements
The authors are sincerely grateful to the research team and the seven communities for their support and cooperation.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Chinese “12th Five-Year Plan” Supporting Science and Technology Project (No. 2012BAI32B03) and the National Social Science Fund Project (No. 14BRK033).