
Abstract
Acrometastasis is an exceedingly rare condition and is often misdiagnosed or overlooked. We herein describe a 50-year-old patient who developed acrometastasis in the big toe from nasopharyngeal carcinoma. The treatment consisted of amputation through the proximal phalanx, and the patient recovered well. To our knowledge, only one case of acrometastasis from this origin has been reported in the literature to date. Acrometastasis indicates a poor prognosis, and we should choose appropriate treatment to relieve symptoms and benefit the patient.
Introduction
Metastasis to the foot and hand (acrometastasis) is an exceedingly rare condition, occurring in 0.07% to 0.30% of patients with malignancy. 1 Acrometastasis usually occurs as a rare preterminal event and is often part of widespread dissemination of metastases. Metastases to the feet are even rarer and have been reported at one-half to one-third the rate of metastases to the hand. Acrometastases are often misdiagnosed. Failure to recognize these lesions has led to delayed diagnosis and/or inappropriate treatment. Most cases published to date involved metastases from lung and genitourinary tract origins. To our knowledge, only one case of acrometastasis from nasopharyngeal carcinoma has been reported in the literature to date. 2
In this article, we report a rare case of acrometastasis from nasopharyngeal carcinoma and provide a reference for the diagnosis and treatment of acrometastasis.
Case report
A 50-year-old woman presented with a 6-week history of pain and swelling on her right first toe. The patient reported no preceding history of significant trauma or inflammation and no signs of arthritis of the right foot. Her medical history included diagnosis of an undifferentiated nasopharyngeal neoplasm 6 years previously. In 2011 she had undergone radiotherapy and chemotherapy, which is the standard treatment for nasopharyngeal cancer. 3 , 4 The initial response was complete, and the patient was followed up by clinical examination every 6 months. Pulmonary metastases and coughing were noted 1 year before the current presentation, and palliative care was instituted. The cough was relieved and the patient discontinued further treatment.
Physical examination revealed a tender, firm, red swelling on the right big toe (Figure 1). The pain increased when pressure was applied on the toe. The patient exhibited decreased active interphalangeal flexion. No loss of sensation or passive range of motion was found. The neurovascular status of the digit was normal. Blood tests revealed an inflammatory syndrome (C-reactive protein concentration of 35.25 mg/L). The patient’s symptoms were partially eased by anti-inflammatory drugs. Radiographs showed an osteolytic process involving the distal phalanx of the right big toe with no periosteal reaction (Figure 2). Magnetic resonance imaging (Siemens Essenza 1.5T scanner; Siemens Healthineers, Erlangen, Germany) showed a mass in the distal phalanx of the right big toe. The dimensions of the tumor were 2.3 × 2.0 × 2.1 cm. The mass showed equal signal intensity on T1-weighted images and high signal intensity on T2-weighted images. The tumor showed significant enhancement after administration of contrast agent (Figure 3).

Physical examination revealed a tender, firm, red swelling on the right big toe.

Radiograph of the right foot showed an osteolytic lesion (arrow) at the distal phalanx of the first metatarsal.
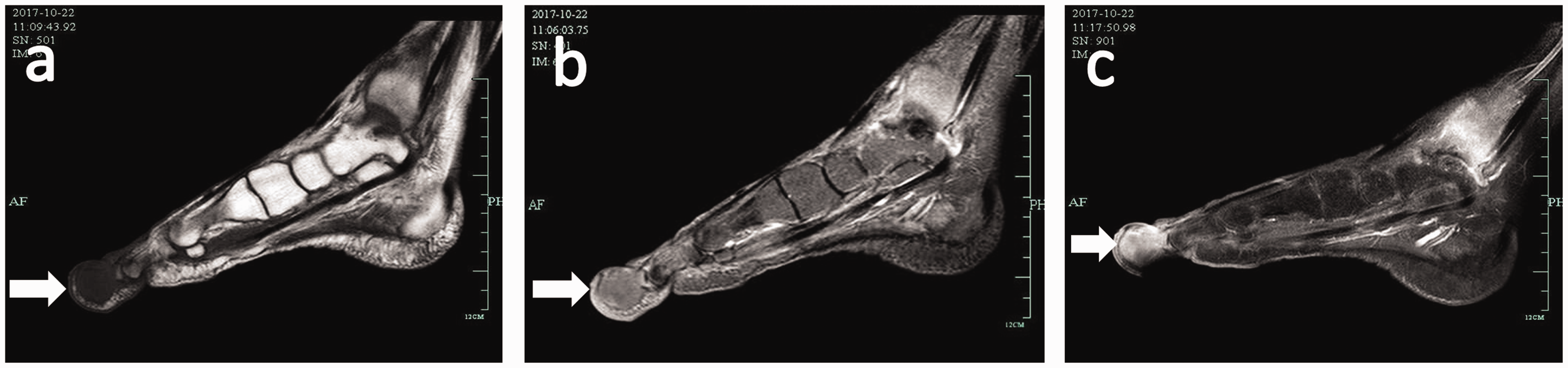
Sagittal magnetic resonance images showed a mass at the distal phalanx of the first metatarsal (a, b) The mass showed iso-signal intensity on T1-weighted imaging and high signal intensity on T2-weighted imaging. (c) The mass showed significant enhancement after administration of contrast agent (arrows).
Clinical evaluation indicated a malignant tumor. Options of amputation versus wide resection and toe salvage were discussed with the patient, and the decision was made to perform amputation through the first metatarsophalangeal joint. The surgical procedure was performed under general anesthesia. A tourniquet was used to avoid hemorrhage. After toe amputation, a piece of skin was used to cover the wound. Macroscopically, the lesion contained necrotic tissue with bony invasion. The lesion was referred for histologic analysis because of these atypical intraoperative findings.
Grossly, the tumor tissue appeared as a soft gray mass measuring 2.6 × 1.7 cm. Microscopically, invasive tumor growth was evident as shown by clusters of malignant cells featuring central necrosis. Immunohistochemical staining demonstrated positive expression of p63, CK5/6, and EBER and negative expression of CD56, CgA, and Syn (Figure 4). These findings were similar to the primary nasopharyngeal neoplasm diagnosed 6 years previously and confirmed the diagnosis of nasopharyngeal metastasis with negative surgical margins.

Photomicrograph of the tumor. (a, b) Microscopic specimen of the lesion showed strong immunoreactivity for EBER. (c, d) The tumor cells stained positive for CK5/6.
The patient underwent antibiotic therapy for 1 week after the surgery. The wound healed well, and no infection occurred. Two weeks after the surgery, the patient was able to walk and her pain had resolved. Her postoperative recovery was uneventful, and she was referred to an oncologist. The patient underwent a clinical follow-up examination every month. Six months after surgery, she had experienced no symptom recurrence.
This case report followed the CARE guidelines. The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University. Written informed consent was obtained from the patient.
Discussion
Acrometastasis to the feet or hands is an unusual cancer presentation with an extremely low incidence. It most commonly occurs between the ages of 40 to 80 years, and it mainly affects men. 5 Acrometastasis is often misdiagnosed or overlooked not only because of its rarity but also because most cases of acrometastasis remain asymptomatic. 6 Despite its rarity, it is important to recognize and diagnose acrometastasis because it may be the first manifestation of the primary tumor and because failure to recognize acrometastasis may lead to a delayed diagnosis and inappropriate treatment.
Acrometastasis is an unusual form of neoplastic dissemination with an incidence of only 0.007% to 0.300%. 5 Diagnosis of the neoplasm of origin based on the presence of acrometastasis is difficult because of its clinical features. The distal phalanges are the most common site of acrometastasis. 7 Acrometastases often remain asymptomatic; only 10% are symptomatic. Symptoms and signs are variable and may include swelling, erythema, fracture, pain, numbness, heat, or even persistent infection and ulceration, often leading to misdiagnosis of a metabolic condition or soft tissue infection. 8 Radiographs usually show osteolytic lesions except in some osteoblastic lesions of acrometastasis from prostatic cancer. Biopsy or fine-needle aspiration cytology leads to an accurate diagnosis.
Acrometastasis to the foot or hand is believed to spread through the blood, not the lymphatics. Any type of malignant tumor can produce acrometastasis, and metastasis from the lungs has been reported in >40% of cases. 8 Kidney and breast cancers are the next most common primary tumors. Malignant neoplasms from these three sites account for two-thirds of cases of acrometastasis. 2 , 9 In the present case, nasopharyngeal cancer produced acrometastasis to the distal phalanx of the right big toe. A previous case report by Plotkine et al. 2 discussed a similar case of acrometastasis to the right long finger from nasopharyngeal origin.
Acrometastasis to the hand and foot generally indicates a poor prognosis because it usually suggests that the primary cancer has become widespread. Once acrometastasis has manifested, most patients survive for an average of only 5 months. 2 Because of the poor prognosis, the main objective of treatment in these patients is pain control and maximal preservation of the function of the affected extremity. The most appropriate therapeutic strategy is determined by the origin of the cancer, the patient’s condition, and the location of the lesion.
Palliative care is most common in patients with acrometastasis. Radiotherapy is helpful in relieving pain due to a single intraosseous metastasis without additional surgical intervention. 5 Wide excision or amputation of apparently isolated metastatic hand lesions can produce long disease-free intervals. 7 , 10 If the hand lesion is symptomatic and distal, amputation through the proximal joint is generally performed. In our case, the patient underwent amputation through the first metatarsophalangeal joint. Her pain resolved and she was satisfied with the outcome of the surgery.
Footnotes
Acknowledgement
The corresponding author expresses his deepest gratitude to his colleagues and coauthors (Drs. Haiying Zhou, Hui Lu, Feixia Ma, and Hui Shen) for providing valuable assistance in every stage of the manuscript preparation. The corresponding author also thanks his friends and wife for providing encouragement and support.
Authors’ contributions
SJ drafted the manuscript and contributed to the revision of the manuscript. HZ and FM helped to draft the manuscript. HS contributed to the critical revision of the manuscript for intellectual content. HL conceived of the study and participated in its design and coordination. All authors read and approved the final manuscript.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article.
Consent to publish
All the authors consent to publication of the manuscript in this journal. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Natural Science Foundation of Zhejiang Province (grant no. LQ20H060008) and the Zhejiang Medicine and Hygiene Research Program (grant no. 2018KY055).